Download presentation
Presentation is loading. Please wait.

1
Management of Obstetrical Hemorrhage Jeffrey L. Stern, M.D.

2
Management of Obstetrical Hemorrhage VS q 15 minutes, oxygen by mask 10 liter/min. – to keep O2 saturation > 94% 1st IV: LR w/ Pitocin 20-40 units at 1000 ml/ 30 minutes Start 2 nd, 18 G IV: warm LR - administer wide open CBC, fibrinogen, PT/PTT, platelets, T&C 4u PRBCs Monitor I&O, urinary Foley catheter Get help –Anesthesia,Interventional Radiology, GYN ONC, Intensivist, etc.

3
Management of Obstetrical Hemorrhage LR or NS replaces blood loss at 3:1 Volume expander 1:1 (albumin, hetastarch, dextran) Administer uterotonic medications Anticipate disseminated Intravascular coagulapathy (DIC) Verify complete removal of placenta, may need ultrasound Inspect for bleeding –episiotomy, laceration, hematomas, inversion, rupture Emperic transfusion –2 u PRBC; FFP 1-2 u/4-5 u PRBC –Cryo 10 u, uncrossed (O neg.) PRBC Warm blood products and I.V.infusions – prevent hypothermia, coagulopathy, arrhythmias
 Administer uterotonic medications Anticipate disseminated Intravascular coagulapathy (DIC) Verify complete removal of placenta, may need ultrasound Inspect for bleeding –episiotomy, laceration, hematomas, inversion, rupture Emperic transfusion –2 u PRBC; FFP 1-2 u/4-5 u PRBC –Cryo 10 u, uncrossed (O neg.) PRBC Warm blood products and I.V.infusions – prevent hypothermia, coagulopathy, arrhythmias")
4
Target Values Invasive monitoring: central/ arterial lines Maintain systolic BP>90 mmHg Maintain urine output > 0.5 ml per kg per hour Hct > 21% Platelets > 50,000/ul Fibrinogen > 100 mg/dl PT/PTT < 1.5 times control Repeat labs as needed – every 30 minutes

5
Blood Component Therapy Fresh Frozen Plasma (45 minutes to thaw) –INR > 1.5 - 2u FFP –INR 2-2.5 - 4u FFP –INR > 2.5 - 6u FFP Cryoprecipitate (1 hour to thaw) –Fibrinogen < 100 mg/dl – 10u cryo –Fibrinogen < 50 mg/dl – 20u cryo Platelets (5 minutes when in stock) –Platelet. count. < 100,000 – 1u plateletpheresis –Platelet. count. < 50,000 – 2u plateletpheresis

6
Blood Component Therapy Blood CompContentsVolume (ml) Effect Packed RBCsRBC, Plasma300Inc. Hgb by 1 g/dl PlateletsPlatelets, Plasma250Inc. count by 25,000 FFP Fibrinogen, antithrombin III, clotting factors, plasma 250Inc. Fibrinogen 10 mg/dl Cryoprecipitate Fibrinogen, antithrombin III, clotting factors, plasma 40Inc. Fibrinogen 10 mg/dl

7
Uterine Atony: 1 in 20 to 1 in 100 deliveries (80% of PPH) Uterine over distension –Polyhydramnios, Multiple gestations, Macrosomia Prolonged labor: “uterine fatigue” (3.4 odds ratio) Precipitory labor High parity Chorioamnionitis Halogenated anesthetic Uterine inversion
 Uterine over distension –Polyhydramnios, Multiple gestations, Macrosomia Prolonged labor: uterine fatigue (3.4 odds ratio) Precipitory labor High parity Chorioamnionitis Halogenated anesthetic Uterine inversion")
8
Treatment of Uterine Atony Message fundus continuously Uterotonic agents Foley catheter/ Bakri balloon (500cc) Uterine packing usually ineffective- can temporize Modified B-Lynch stitch (#2chromic) Uterine/ utero-ovarian artery ligation Hypogastric artery ligation Subtotal or Total abdominal hysterectomy
 Uterine packing usually ineffective- can temporize Modified B-Lynch stitch (#2chromic) Uterine/ utero-ovarian artery ligation Hypogastric artery ligation Subtotal or Total abdominal hysterectomy")
9
Treatment of Uterine Atony Oxytocin – 90% success –10-40 units in 1 liter NS or LR rapid infusion Methylergonovine (Methergine) - 90% success –0.2 mg IM q 2-4 hours max. 5 doses; avoid with hypertension Prostaglandin F2 Alpha (Hemabate) - 75% success –250 mcg IM; intramyometrial, repeat q 20-90 min; max 8 doses. –Avoid if asthma/Hi BP. Prostaglandin E2 suppositories (Dinoprostone, Prostin E2) - 75% success –20 mg per rectum q 2 hours; avoid with hypotension Prostaglandin E1 Misoprostol (Cytotec): 75 -100% success –1000 mcg per rectum or sublingual (100 or 200 mcg tabs)
 - 75% success –250 mcg IM; intramyometrial, repeat q min; max 8 doses. –Avoid if asthma/Hi BP. Prostaglandin E2 suppositories (Dinoprostone, Prostin E2) - 75% success –20 mg per rectum q 2 hours; avoid with hypotension Prostaglandin E1 Misoprostol (Cytotec): % success –1000 mcg per rectum or sublingual (100 or 200 mcg tabs).")
10
Uterine Inversion: 1 in 2500 Deliveries Risk factors: Abnormal placentation, excessive cord traction Treatment –Manual replacement –May require halothane/ general anesthesia –Remove placenta after re-inversion –Uterine tonics and massage after placenta is removed –May require laparotomy

11
Uterine Rupture Etiology Previous uterine surgery - 50% of cases –C-section, Hysterotomy, Myomectomy Spontaneous (1/1900 deliveries) Version-external and internal Fundal pressure Blunt trauma Operative vaginal delivery Penetrating wounds
 Version-external and internal Fundal pressure Blunt trauma Operative vaginal delivery Penetrating wounds")
12
Uterine Rupture Etiology Oxytocics Grand multiparity Obstructed labor Fetal abnormalities-macrosomia, malposition, anomalies Placenta percreta Tumors: Trophoblastic disease, cervical cancer Extra-tubal ectopic pregnancy

13
Classic Symptoms of Uterine Rupture Fetal distress Vaginal bleeding Cessation of labor Shock Easily palpable fetal parts Loss of uterine catheter pressure

14
Uterine Rupture Myth: Uterine incisions that do not enter the endometrial cavity will not rupture in the future Type of closure: no relation to tensile strength –Continuous or interrupted sutures: chromic, Vicryl, Maxon –Inverted or everted endometrial closure Degree of complications –Inciting event- spontaneous, traumatic –Gestational age –Placental site in relation to rupture site –Presence or absence of uterine scar Scar: 0.8 mortality rate No scar: 13% mortality rate –Location of scar Classical scar- majority of catastrophic ruptures Transverse scar- less vascular; less likely to involve placenta –Extent of rupture

15
Uterine Scar Dehiscence Separation of scar without rupture of membranes –2-4% of deliveries after previous transverse uterine incision –Morbidity is usually minimal unless placenta is underneath or it tears into the uterine vessels –Diagnosis after vaginal delivery Often asymptomatic, incidental finding Difficult to diagnose- lower uterine segment is very thin Therapy is expectant if defect small and asymptomatic –Diagnosed at C-section: Simple debridement and layered closure

16
Management of Uterine Rupture Laparotomy –Debride and repair in 2-3 layers of Maxon/PDS –Subtotal Hysterectomy –Total Hysterectomy

17
Pregnancy After Repair of Uterine Rupture Not possible to predict rupture by HSG/Sono/MRI Repair location –Classical -------------------------48% –Low transverse------------------16% –Not recorded---------------------36% Re-rupture-------------------12% Maternal death--------------1% Perinatal death--------------6% Plauce WC, 1993

18
Prepare for Laparotomy General anesthesia usually best Allen or Yellowfin stirrups Uterine cavity manual exploration for retained placenta with ultrasound present/ uterine rupture Uterine inversion Uterine packing (treatment vs. temporizing) –4” gauze (Kerlex) soaked in 5000 u of thrombin in 5ml of sterile saline –24 Fr. Foley with 30ml balloon filled with 30-80 ml of saline (may need more than one) –Bakri (intrauterine) balloon - 500 cc –Antibiotics –Remove in 24-48 hours
 –4 gauze (Kerlex) soaked in 5000 u of thrombin in 5ml of sterile saline –24 Fr. Foley with 30ml balloon filled with ml of saline (may need more than one) –Bakri (intrauterine) balloon cc –Antibiotics –Remove in hours.")
19
Intraoperatively Consider vertical abdominal incision General anesthesia usually best Get Help! Avoid compounding problems by making major mistakes Direct manual uterine compression / uterotonics Direct aortic compression Modified B-Lynch Suture for atony: #2 chromic Ligation of uterine and utero-ovarian vessels: #1 chromic

20
Intraoperatively Internal iliac (hypogastric) artery ligation ( 50% success) –Desirous of children –Experience of surgeon –Palpate common iliac bifurcation –Ligate at least 2-3 cm from bifurcation –#1 silk. Do not divide vessel Interventional Radiology: uterine artery embolization (catheters placed pre-op) Hysterectomy/ subtotal hysterectomy (put ring forceps on anterior lip of dilated cervix, to help identify it) Cell saver: investigational (amniotic fluid problems)
 Hysterectomy/ subtotal hysterectomy (put ring forceps on anterior lip of dilated cervix, to help identify it) Cell saver: investigational (amniotic fluid problems).")
21
Modified B-Lynch Suture

22
Artery Ligation

23
Management of Abnormal Placentation Placenta will not separate with usual maneuvers Curettage of uterine cavity Localized resection and uterine repair: (Vasopressin 1cc/10cc N.S-sub endometrial) Leave placenta in situ –If not bleeding: Methotrexate –Uterus will not be normal size by 8 weeks Uterine, utero-ovarian, hypogastric artery ligation Subtotal/ total abdominal hysterectomy
 Leave placenta in situ –If not bleeding: Methotrexate –Uterus will not be normal size by 8 weeks Uterine, utero-ovarian, hypogastric artery ligation Subtotal/ total abdominal hysterectomy")
24
Post-Hysterectomy Bleeding Patient usually has DIC – Rx with whole blood, FFP, platelets, etc. Military Anti-Shock Trousers (MAST) –Increases pelvic and abdominal pressure to reduce bleeding –Can use at any point in the procedure Transvaginal or transabdominal (pelvic) pressure pack –Bowel bag with opening pulled through vagina cuff/ abd. wall –Stuff with 4 inch gauze tied end-to-end until pelvis packed tight –Tie to 10-20 lbs. Weight and hang over edge of bed to help keep constant pressure May have to leave clamps or accept ligation of ureter or a major side wall vessel Interventional Radiology
 –Increases pelvic and abdominal pressure to reduce bleeding –Can use at any point in the procedure Transvaginal or transabdominal (pelvic) pressure pack –Bowel bag with opening pulled through vagina cuff/ abd. wall –Stuff with 4 inch gauze tied end-to-end until pelvis packed tight –Tie to lbs. Weight and hang over edge of bed to help keep constant pressure May have to leave clamps or accept ligation of ureter or a major side wall vessel Interventional Radiology.")
25
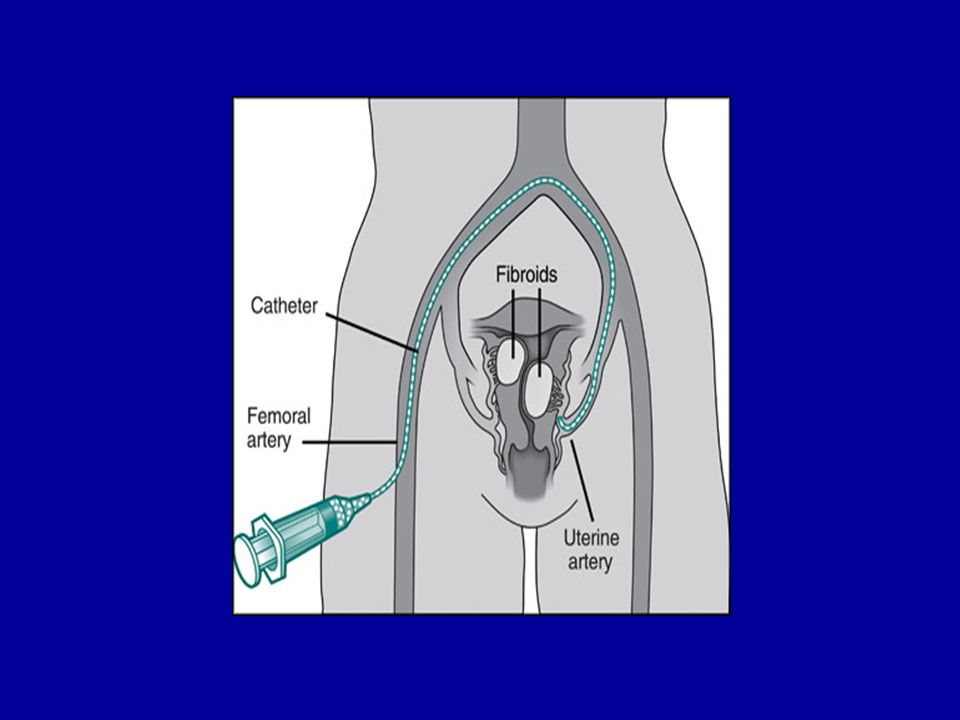
Selective Artertial Embolization by Angiography Clinically stable patient – Try to correct coagulopathy Takes approximately 1-6 hours to work Often close to shock, unstable, require close attention Can be used for expanding hematomas Can be used preoperatively, prophylactically for patients with placenta accreta Analgesics, anti-nausea medications, antibiotics

26
Selective Artertial Embolization by Angiography Real time X-Ray (Fluoroscopy) Access right femoral artery Single bleeding blood vessel is best Embolize: - Both uterine or hypogastric arteries - May need to treat entire anterior division or all of internal iliac artery - Sometimes need a small catheter distally to prevent reflux into non-target vessel Risks: Can embolize nearby organs and presacral tissue, resulting in tissue necrosis Technique: –Gelfoam pads/slurry – Temporary, allows recanalization –Autologous blood clot or tissue –Vasopressin, dopamine, Norepinephrine –Balloons, steel coils
 Access right femoral artery Single bleeding blood vessel is best Embolize: - Both uterine or hypogastric arteries - May need to treat entire anterior division or all of internal iliac artery - Sometimes need a small catheter distally to prevent reflux into non-target vessel Risks: Can embolize nearby organs and presacral tissue, resulting in tissue necrosis Technique: –Gelfoam pads/slurry – Temporary, allows recanalization –Autologous blood clot or tissue –Vasopressin, dopamine, Norepinephrine –Balloons, steel coils")
28
Evaluate for Ovarian Collaterals May need to embolize

29
Mid-Embolization “Pruned Tree Vessels”

30
Post Embolization

31
Pre EmboPost Embo

Similar presentations

: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")

 产后出血 林建华. Major causes of death for pregnancy women ( maternal mortality) Postpartum hemorrhage ( 28%) heart diseases pregnancy-induced.>")


 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")












