Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2014 年 9 月 25 日 8:30-8:55 8階 医局 Eng C, Kramer CK, Zinman B, Retnakaran R. Glucagon-like peptide-1 receptor agonist and basal insulin combination treatment for the management of type 2 diabetes: a systematic review and meta-analysis. Lancet. 2014 Sep 11. pii: S0140-6736(14)61335-0. doi: 10.1016/S0140- 6736(14)61335-0. [Epub ahead of print]
 doi: /S (14) [Epub ahead of print].")
2
a Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, Toronto, ON, Canada b Lunenfeld-Tanenbaum Research Institute, Mount Sinai Hospital, Toronto, ON, Canada c Division of Endocrinology, University of Toronto, Toronto, ON, Canada Lancet. 2014 Sep 11. pii: S0140-6736(14)61335-0. doi: 10.1016/S0140-6736(14)61335-0.
 doi: /S (14)")
3
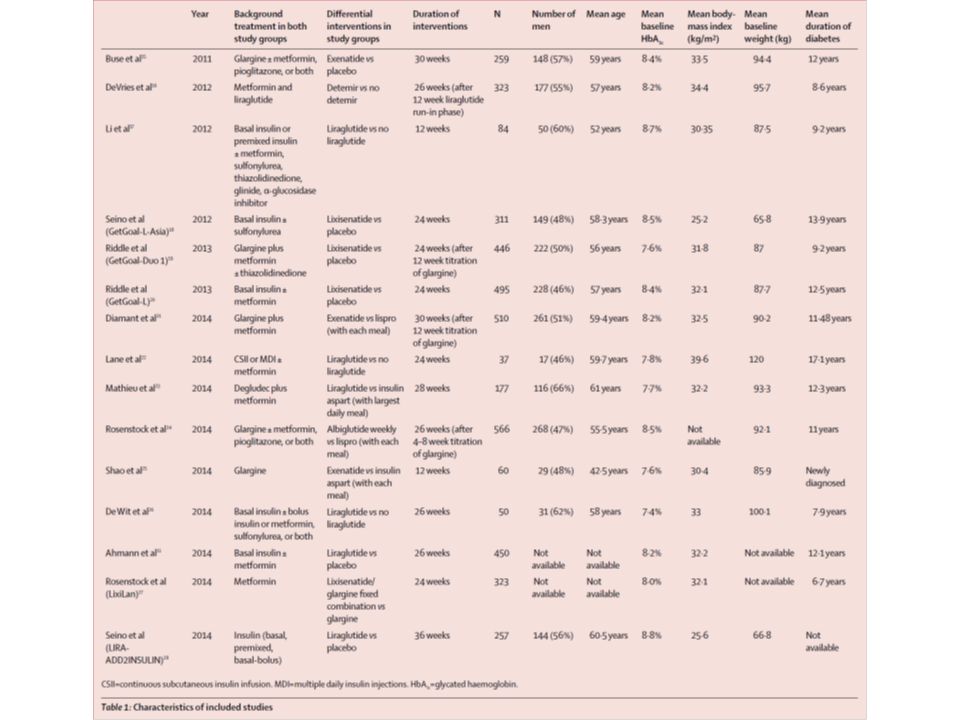
Background Combination treatment with a glucagon-like peptide-1 (GLP-1) agonist and basal insulin has been proposed as a treatment strategy for type 2 diabetes that could provide robust glucose- lowering capability with low risk of hypoglycaemia or weight gain. We thus did a systematic review and meta-analysis of randomised controlled trials to assess the effect of this combination treatment on glycaemic control, hypoglycaemia, and weight gain in patients with type 2 diabetes.

4
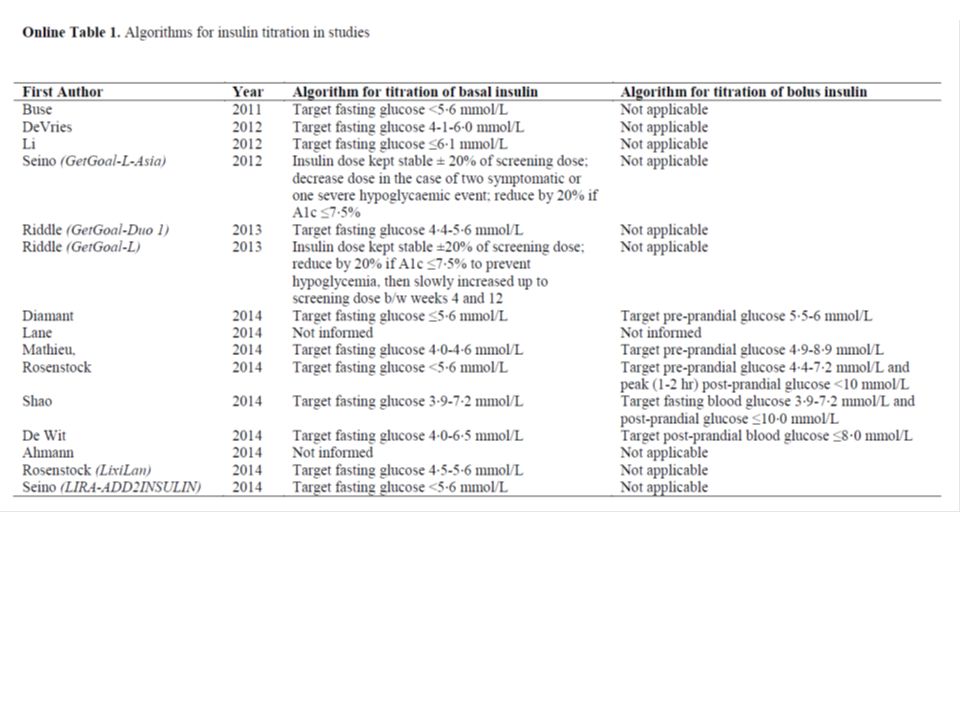
Methods We systematically searched PubMed, Embase, Cochrane, Web of Knowledge, FDA.gov, and ClinicalTrials.gov for randomised controlled trials (published between Jan 1, 1950, and July 29, 2014; no language restrictions) comparing GLP-1 agonist and basal insulin combination treatment to other anti-diabetic treatments. Our main endpoints were glycaemic control, hypoglycaemia, and change in weight. We assessed pooled data by use of a random-effects model.

5
Figure 1: Study selection process

9
Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect. Outcomes assessed are: (A) HbA1c
 HbA1c.")
10
Outcomes assessed are: (B) HbA1c (%) in studies that compared combination treatment with basal- bolus insulin treatment Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 HbA1c (%) in studies that compared combination treatment with basal- bolus insulin treatment Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.")
11
Outcomes assessed are: (C) proportion of participants with HbA1c ≤7 ・ 0% at the end of intervention Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 proportion of participants with HbA1c ≤7 ・ 0% at the end of intervention Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.")
12
Outcomes assessed are: (D) proportion of participants with HbA1c ≤7 ・ 0% at the end of intervention in studies that compared combination treatment with basal-bolus insulin treatment. Figure 2: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing HbA1c concentrations For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect..")
13
Outcomes assessed are (A) hypoglycaemia Figure 3: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 hypoglycaemia Figure 3: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.")
14
Outcomes assessed are (B) hypoglycaemia in studies that compared combination treatment with basal-bolus insulin treatment
 hypoglycaemia in studies that compared combination treatment with basal-bolus insulin treatment")
15
Outcomes assessed are (C) change in weight (kg) at the end of intervention Figure 3: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 change in weight (kg) at the end of intervention Figure 3: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.")
16
Outcomes assessed are (D) change in weight (kg) at the end of intervention in studies that compared combination treatment with basal-bolus insulin treatment. Figure 3: Meta-analyses of glucagon-like peptide-1 (GLP-1) agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect.
 agonist and basal insulin combination treatment versus other anti-diabetic treatments, comparing hypoglycaemia and change in weight For each estimate, the grey shaded area is the weight of the estimate in proportion to the overall effect..")
18
メタアナリシス論文の中に頻出する funnel plot をどう読むか。 funnel plot とはメタアナリシス中で偏った論文が集められていないかを検証するための方法。 図の中央の実線がメタアナリシスで得られた OR を示している。縦軸が標準偏差の大きさを示す。 なので、サンプルサイズが大きくて標準偏差が小さい研究ほど上側に分布、小規模研究ほど下側に 分布する。 論文が偏りなく集められているとすると、サンプリングエラーだけが残るので通常は中央の実線か ら対称性に論文が散らばるはずである。 逆に片方の介入に都合のいい論文だけを集めているとプロットが非対称性になってしまう。 なので、 funnel plot をおこなって左右対称にプロットされていれば publication bias など受けずに適 切に論文収集がおこなわれているという証明になる。 それを数字で表したのが Egger's test 。これは対称に分布しているという帰無仮説と非対称に分布 しているという対立仮説を用いて疫学的に対称性を証明する手法。 まぁ要するに p 値が 0.05 以上だと対称性分布っぽいなぁと言える。 (もっとちゃんと言うと、 5% を有意とした検定において対称性分布であるという帰無仮説を棄却 できない) 以上からもわかるように funnel plot はある程度のプロット数がないと対称かどうかわからなくなっ てしまう。 通常は 10 以上の論文が集められている前提で使われる手法である。 (BMJ 2013; 346: f1342)
 以上からもわかるように funnel plot はある程度のプロット数がないと対称かどうかわからなくなっ てしまう。 通常は 10 以上の論文が集められている前提で使われる手法である。 (BMJ 2013; 346: f1342)")
19
Findings Of 2905 identified studies, 15 were eligible and were included in our analysis (N=4348 participants). Compared with other anti-diabetic treatments, GLP-1 agonist and basal insulin combination treatment yielded an improved mean reduction in glycated haemoglobin (HbA1c) of −0·44% (95% CI −0·60 to −0·29), an improved likelihood of achieving the target HbA1c of 7·0% or lower (relative risk [RR] 1·92; 95% CI 1·43 to 2·56), no increased relative risk of hypoglycaemia (0·99; 0·76 to 1·29), and a mean reduction in weight of −3·22 kg (−4·90 to −1·54). Furthermore, compared with basal-bolus insulin regimens, the combination treatment yielded a mean reduction in HbA1c of −0·1% (−0·17 to −0·02), with lower relative risk of hypoglycaemia (0·67, 0·56 to 0·80), and reduction in mean weight (−5·66 kg; −9·8 to −1·51).
 of −0·44% (95% CI −0·60 to −0·29), an improved likelihood of achieving the target HbA1c of 7·0% or lower (relative risk [RR] 1·92; 95% CI 1·43 to 2·56), no increased relative risk of hypoglycaemia (0·99; 0·76 to 1·29), and a mean reduction in weight of −3·22 kg (−4·90 to −1·54). Furthermore, compared with basal-bolus insulin regimens, the combination treatment yielded a mean reduction in HbA1c of −0·1% (−0·17 to −0·02), with lower relative risk of hypoglycaemia (0·67, 0·56 to 0·80), and reduction in mean weight (−5·66 kg; −9·8 to −1·51)..")
20
Interpretation GLP-1 agonist and basal insulin combination treatment can enable achievement of the ideal trifecta in diabetic treatment: robust glycaemic control with no increased hypoglycaemia or weight gain. This combination is thus a potential therapeutic strategy that could improve the management of patients with type 2 diabetes.

21
Message 2 型糖尿病( DM )管理におけるグルカゴン様ペ プチド -1 ( GLP-1 )受容体作動薬+基礎インス リン併用療法の効果を、無作為化比較試験 15 件 (被験者 4348 人)のシステマティックレビュー とメタ解析で検証。他の治療法に比べ併用療法で HbA1c の平均低下値と 7.0 %未満達成率が改善 し、低血糖リスクや体重の増加は見られなかった。 このままゆくと、超速効型インスリンの売り上げ が減る?
管理におけるグルカゴン様ペ プチド -1 ( GLP-1 )受容体作動薬+基礎インス リン併用療法の効果を、無作為化比較試験 15 件 (被験者 4348 人)のシステマティックレビュー とメタ解析で検証。他の治療法に比べ併用療法で HbA1c の平均低下値と 7.0 %未満達成率が改善 し、低血糖リスクや体重の増加は見られなかった。 このままゆくと、超速効型インスリンの売り上げ が減る?")
Similar presentations







行列式の定義には、数学的な概念がいろいろ必要である。まずそれらを順に見ていく。>")


 玉岡賀津雄(名古屋大学) 木山幸子(麗澤大学大学院生) 言語科学会第 11 回年次国際大会 (JSLS2009)>")




 ・Excelによる演習>")
 入力データに含まれる、本来ほしくない 成分.>")
を体験したことにより興味を惹かれ るきっかけとなった。主な目的は、これ.>")



を生かした 確かな学力を形成する授業づく り ② 家庭との連携を図った家庭学習の習慣化.>")
