Download presentation
Presentation is loading. Please wait.

1
Basics of EKG Interpretation
Michael Rochon-Duck July 6, 2015 Slideset adapted from: Jennifer Ballard-Hernandez, DNP

2
Goals Understand the normal electrical activation of the heart
Correlate the ECG to the timing and direction of cardiac electrical activity Gain confidence with recognizing common ECG findings Start interpreting ECGs

3
What is an ECG? Noninvasive test that examines the electrical conduction of the heart Measures the amount of electrical voltage generated by depolarization of the heart muscle Sum of all electrical forces (vectors) at a given moment in time Voltage may be a negative of positive value
 at a given moment in time. Voltage may be a negative of positive value.")
4
12 Leads = 12 Vantage Points

5
Limb Leads: Vertical Plane

6
Precordial Leads: Horizontal Plane

7
Munshi 2012

9
Impulse Conduction & the ECG
Sinoatrial node AV node Bundle of His Bundle Branches Purkinje fibers

10
The “PQRST” P wave - Atrial depolarization
QRS - Ventricular depolarization T wave - Ventricular repolarization

11
The ECG Paper Horizontally Vertically One small box - 0.04 sec.
One large box sec. Vertically One large box mV

12
You Must Have a Method to Your Madness!
To eliminate potential errors and avoid missed data – you MUST have a protocol in your interpretation of ECG’s The protocol must be easy, logical and sequential

13
ECG Analysis Step 1: Rate Step 2: Rhythm Step 3: Intervals-PR
Step 4: Intervals-QRS Step 5: Axis Step 6: ST Segment / Waves Step 7: Overall Interpretation

14
Step 1: Calculate Rate Option 1 Interpretation? 11 x 6 = 66 bpm
Count the # of R waves in a 10 second rhythm strip, then multiply by 6. This method should be used for all irregular rhythms Interpretation? 11 x 6 = 66 bpm

15
Step 1: Calculate Rate Option 2 R wave
Find a R wave that lands on a bold line. Count the # of large boxes to the next R wave. If the second R wave is 1 large box away the rate is 300, 2 boxes - 150, 3 boxes - 100, 4 boxes - 75, etc. (cont) R wave
 R wave.")
16
Step 1: Calculate Rate Option 2 (cont) Interpretation?
300 150 100 75 60 50 Option 2 (cont) Memorize the sequence: Interpretation? Approx. 1 box less than 100 = 95 bpm
 Memorize the sequence: Interpretation Approx. 1 box less than 100 = 95 bpm.")
17
Step 1: Calculate Rate Option 3 (Jen’s favorite ) Interpretation?
Count the number of small boxes between two R waves and divide into 1500 Interpretation? 1500/16=93.75 HR=94

18
What is the rate?

19
What is the rate? 2

20
What is the rate? 3

21
Abnormalities in Rate >100/min = tachyarrhythmia
<60/min = bradyarrhythmia Further defined by site of origin Sinus node Atrial Junctional Ventricular

22
The Fastest Pacemaker Captures the Heart

23
Step 2: Determine regularity
Look at the R-R distances (using a caliper or markings on a pen or paper). Regular (are they equidistant apart)? Occasionally irregular? Regularly irregular? Irregularly irregular? Interpretation? Regular
. Regular (are they equidistant apart) Occasionally irregular Regularly irregular Irregularly irregular Interpretation Regular.")
24
Step 2: Rhythm Assess the P waves
Are there P waves? Morphology: Do P waves all look alike? Is there one P wave before each QRS? P waves upright in I, II, aVF? Is the PR interval constant? Interpretation? Normal P waves with 1 P wave for every QRS

25
Step 3: Determine PR interval
Normal: 120 – 200 ms (3 - 5 boxes) Interpretation? 0.12 seconds
 Interpretation 0.12 seconds.")
26
Step 4: Determine the QRS Interval
Normal: 40 – 100 ms (1 – 2.5 boxes) Interpretation? 0.08 seconds
 Interpretation 0.08 seconds.")
27
Bundle Branch Blocks

28
Bundle Branch Blocks Turning our attention to bundle branch blocks…
Remember normal impulse conduction is SA node AV node Bundle of His Bundle Branches Purkinje fibers

29
Normal Impulse Conduction
Sinoatrial node AV node Bundle of His Bundle Branches Purkinje fibers

30
Bundle Branch Blocks So, depolarization of the Bundle Branches and Purkinje fibers are seen as the QRS complex on the ECG. Right BBB Therefore, a conduction block of the Bundle Branches would be reflected as a change in the QRS complex.

31
Bundle Branch Blocks With Bundle Branch Blocks you will see two changes on the ECG. QRS complex widens (> 0.12 sec). QRS morphology changes (varies depending on ECG lead, and if it is a right vs. left bundle branch block).
.")
32
Bundle Branch Blocks Why does the QRS complex widen?
When the conduction pathway is blocked it will take longer for the electrical signal to pass throughout the ventricles because the impulse has to travel from cell to cell inefficiently.

34
Right Bundle Branch Blocks
What QRS morphology is characteristic? For RBBB the wide QRS complex assumes a unique, virtually diagnostic shape (upright “rabbit ears”) in those leads overlying the right ventricle, V1. V1 “Rabbit Ears”
 in those leads overlying the right ventricle, V1. V1. Rabbit Ears")
35
Left Bundle Branch Blocks
What QRS morphology is characteristic? For LBBB the wide QRS complex assumes a wide predominantly downward deflection leads opposite the left ventricle, i.e., V1 and V2 (right ventricular leads) and the QRS is upright and wide in V5 and V6 (may or may not be notched)
 and the QRS is upright and wide in V5 and V6 (may or may not be notched)")
36
Bundle Branch Block RBBB QRS > 0.12
V1 rsR’ pattern and T wave inversion V6 widened S wave and upright T LBBB QRS > 0.12 V1 QS pattern V6 notched R Wave and inverted T wave

37
What causes BBBs? Hypertension Coronary artery disease
Thickened, stiffened or weakened heart muscle (cardiomyopathy) Infection (myocarditis) of the heart muscle Scar tissue after heart surgery Congenital abnormality
 Infection (myocarditis) of the heart muscle. Scar tissue after heart surgery. Congenital abnormality.")
38
BBB Left or Right?

39
BBB Left or Right?

42
Intervals PR QRS QT Normal < .2 sec (1 large box)
> .2 sec = 1st degree AV block Causes: ischemia, senescence, medications QRS Normal < .12 sec (3 small boxes) > .12 sec = IVCD; bundle branch block Causes: congenital, ischemia/infarct, LVH, pacemaker QT Varies with rate Normal < ½ R-R interval > 450 msec (QTc) = abnormal; predisposition to ventricular arrhythmias Causes: medications, Genetic disorders
 > .12 sec = IVCD; bundle branch block. Causes: congenital, ischemia/infarct, LVH, pacemaker. QT. Varies with rate. Normal < ½ R-R interval. > 450 msec (QTc) = abnormal; predisposition to ventricular arrhythmias. Causes: medications, Genetic disorders.")
43
Step 5: Axis The mean direction of electrical forces in the frontal plane (limb leads) as measured from the point of zero We like to know the QRS axis because an abnormal axis can suggest disease Normal QRS Axis: -30 to 90

44
Axis

45
Axis: Quick and Easy Lead I and Lead II

46
Left Axis Deviation Mechanical shifts: Expiration, high diaphragm (pregnancy, ascites) Left bundle branch block Left anterior fascicular Emphysema Hyperkalemia Wolff-Parkinson-White syndrome Congenital heart disease: Primum ASD

47
Right Axis Deviation Normal finding in children and tall thin adults
Mechanical shifts: Inspiration Right ventricular hypertrophy Right bundle branch block Left posterior fascicular block Chronic lung disease COPD Dextrocardia Pulmonary embolus

48
Is the QRS axis normal in this ECG?
The QRS is positive in I and negative in II. No, there is left axis deviation.

49
Step 6: ST Segments and waves
The ST segment is the flat isoelectric section of the ECG between the end of the S wave and start of the T wave Myocardial ischemia tends to be a regional event MI and injury cause a variety of changes in ST segments T waves and QRS complexes ECG changes that are global are rarely cause by ischemia i.e.pericarditis

50
Step 6: ST Segments and waves
Questions to ask: Is there ST segment elevation or depression? Are the T waves inverted? Are there pathological Q waves?

51
ST Segment

52
Waves/Complexes T Wave
Peaked: hyperkalemia, hypocalcemia, hyperacute MI Flat w/ U wave – hypokalemia w/o U wave –ischemia (if 2 or more contiguous leads) Inverted Symmetric: more likely to be ischemia (if 2 or more contiguous leads) Assymetric: drugs, strain (LVH/subendocardial strain) Biphasic Ischemia (if 2 or more contiguous leads)
 Inverted. Symmetric: more likely to be ischemia (if 2 or more contiguous leads) Assymetric: drugs, strain (LVH/subendocardial strain) Biphasic. Ischemia (if 2 or more contiguous leads)")
53
ST Elevation Infarction
The ECG changes seen with a ST elevation infarction are: Before injury Normal ECG Ischemia ST depression, peaked T-waves, then T-wave inversion Infarction ST elevation & appearance of Q-waves Fibrosis ST segments and T-waves return to normal, but Q-waves persist

54
ST Elevation Infarction
Here’s a diagram depicting an evolving infarction: A. Normal ECG prior to MI B. Ischemia from coronary artery occlusion results in ST depression (not shown) and peaked T-waves C. Infarction from ongoing ischemia results in marked ST elevation D/E. Ongoing infarction with appearance of pathologic Q-waves and T-wave inversion F. Fibrosis (months later) with persistent Q- waves, but normal ST segment and T- waves
 and peaked T-waves. C. Infarction from ongoing ischemia results in marked ST elevation. D/E. Ongoing infarction with appearance of pathologic Q-waves and T-wave inversion. F. Fibrosis (months later) with persistent Q- waves, but normal ST segment and T- waves.")
55
ST Segment Significant Elevation Depression
> 1mm above or below isoelectric 2 or more contiguous leads Elevation Infarct *Exception: Global ST elevation in pericarditis Depression Ischemia Drug effect Electrolytes

56
Contiguous Leads Inferior Lateral Anterior Septal Posterior
II, III, aVF Lateral I, aVL V5, V6 Anterior V1-V4 Septal V2, V3 Posterior V1, V2, V3

57
Contiguous Leads

58
ST Segment Depression

59
ST Elevation One way to diagnose an acute MI is to look for elevation of the ST segment.

60
ST Elevation (cont) Elevation of the ST segment (greater than 1 small box) in 2 leads is consistent with a myocardial infarction.
 Elevation of the ST segment (greater than 1 small box) in 2 leads is consistent with a myocardial infarction.")
61
Locating Myocardial Damage
Remember that the 12-leads of the ECG look at different portions of the heart. The limb and augmented leads “see” electrical activity moving inferiorly (II, III and aVF), to the left (I, aVL) and to the right (aVR). Whereas, the precordial leads “see” electrical activity in the posterior to anterior direction. Limb Leads Augmented Leads Precordial Leads
, to the left (I, aVL) and to the right (aVR). Whereas, the precordial leads see electrical activity in the posterior to anterior direction. Limb Leads. Augmented Leads. Precordial Leads.")
62
The 12-Leads The 12-leads include: 3 Limb leads (I, II, III)
3 Augmented leads (aVR, aVL, aVF) 6 Precordial leads (V1- V6)
 6 Precordial leads (V1- V6)")
63
Views of the Heart Lateral portion of the heart
Some leads get a good view of the: Anterior portion of the heart Inferior portion of the heart

64
Anterior MI The anterior portion of the heart is best viewed using leads V1- V4. Left Coronary Artery Limb Leads Augmented Leads Precordial Leads

65
Lateral MI The Lateral wall of the heart is best viewed using leads Leads I, aVL, and V5- V6 Circumflex Artery Limb Leads Augmented Leads Precordial Leads

66
Inferior MI The Inferior wall of the heart is best viewed using leads Leads II, III and aVF Right Coronary Artery Limb Leads Augmented Leads Precordial Leads

67
Q Waves Q wave Late evolving or chronic stage of myocardial infarction
Significance > 1 small box wide > ¼ of R wave height 2 or more contiguous leads

69
Putting it all Together
Do you think this person is having a myocardial infarction. If so, where?

70
Interpretation Yes, this person is having an acute anterior wall myocardial infarction.

71
Putting it all Together
Now, where do you think this person is having a myocardial infarction?

72
Inferior Wall MI This is an inferior MI. Note the ST elevation in leads II, III and aVF.

73
Putting it all Together
How about now?

74
Anterolateral MI This person’s MI involves both the anterior wall (V2-V4) and the lateral wall (V5-V6, I, and aVL)!
 and the lateral wall (V5-V6, I, and aVL)!")
75
Diagnosing a MI To diagnose a myocardial infarction you need to go beyond looking at a rhythm strip and obtain a 12-Lead ECG. 12-Lead ECG Rhythm Strip

76
Left Ventricular Hypertrophy

77
Left Ventricular Hypertrophy
Compare these two 12-lead ECGs. What stands out as different with the second one? The QRS complexes are very tall (increased voltage) Normal Left Ventricular Hypertrophy Answer:
 Normal. Left Ventricular Hypertrophy. Answer:")
78
Left Ventricular Hypertrophy
Why is left ventricular hypertrophy characterized by tall QRS complexes? Increased QRS voltage As the heart muscle wall thickens there is an increase in electrical forces moving through the myocardium resulting in increased QRS voltage. LVH ECHOcardiogram

79
Left Ventricular Hypertrophy
Specific criteria exists to diagnose LVH using a 12-lead ECG. For example: The R wave in V5 or V6 plus the S wave in V1 or V2 exceeds 35 mm.

80
Now that we have the basics down
Lets do some rhythm strip analysis!

81
Sinus Rhythms Sinus Bradycardia Sinus Tachycardia

82
Rhythm #1 Rate? 30 bpm Regularity? regular P waves? normal
PR interval? 0.12 s QRS duration? 0.10 s Interpretation? Sinus Bradycardia

83
Sinus Bradycardia Deviation from NSR - Rate < 60 bpm

84
Sinus Bradycardia Etiology: SA node is depolarizing slower than normal, impulse is conducted normally (i.e. normal PR and QRS interval).
.")
85
Rhythm #2 Rate? 130 bpm Regularity? regular P waves? normal
PR interval? 0.16 s QRS duration? 0.08 s Interpretation? Sinus Tachycardia

86
Sinus Tachycardia Deviation from NSR - Rate > 100 bpm

87
Sinus Tachycardia Etiology: SA node is depolarizing faster than normal, impulse is conducted normally. Remember: sinus tachycardia is a response to physical or psychological stress, not a primary arrhythmia.

88
Premature Beats Premature Atrial Contractions (PACs)
Premature Ventricular Contractions (PVCs)
")
89
Rhythm #3 Rate? 70 bpm Regularity? occasionally irreg. P waves?
2/7 different contour PR interval? 0.14 s (except 2/7) QRS duration? 0.08 s Interpretation? NSR with Premature Atrial Contractions
 QRS duration 0.08 s. Interpretation NSR with Premature Atrial Contractions.")
90
Premature Atrial Contractions
Deviation from NSR These ectopic beats originate in the atria (but not in the SA node), therefore the contour of the P wave, the PR interval, and the timing are different than a normally generated pulse from the SA node.
, therefore the contour of the P wave, the PR interval, and the timing are different than a normally generated pulse from the SA node.")
91
Premature Atrial Contractions
Etiology: Excitation of an atrial cell forms an impulse that is then conducted normally through the AV node and ventricles.

92
Teaching Moment When an impulse originates anywhere in the atria (SA node, atrial cells, AV node) and then is conducted normally through the ventricles, the QRS will be narrow ( s).
 and then is conducted normally through the ventricles, the QRS will be narrow ( s).")
93
Rhythm #4 Rate? 60 bpm Regularity? occasionally irreg. P waves?
none for 7th QRS PR interval? 0.14 s QRS duration? 0.08 s (7th wide) Interpretation? Sinus Rhythm with 1 PVC
 Interpretation Sinus Rhythm with 1 PVC.")
94
PVCs Deviation from NSR
Ectopic beats originate in the ventricles resulting in wide and bizarre QRS complexes. When there are more than 1 premature beats and look alike, they are called “uniform”. When they look different, they are called “multiform”.

95
PVCs Etiology: One or more ventricular cells are depolarizing and the impulses are abnormally conducting through the ventricles.

96
Teaching Moment When an impulse originates in a ventricle, conduction through the ventricles will be inefficient and the QRS will be wide and bizarre.

97
Ventricular Conduction
Normal Signal moves rapidly through the ventricles Abnormal Signal moves slowly through the ventricles

98
Rhythm #5 Rate? 110 bpm Regularity? P waves? none PR interval?
Irregularly irregular P waves? none PR interval? Unable to determine QRS duration? 0.08 s Interpretation? Afib

99
Rhythm #6 Rate? 90 bpm Regularity? Regular P waves? none PR interval?
Unable to determine QRS duration? 0.08 s Interpretation? Aflutter

100
AV Nodal Blocks 1st Degree AV Block 2nd Degree AV Block, Type I
2nd Degree AV Block, Type II 3rd Degree AV Block

101
Rhythm #7 Rate? 60 bpm Regularity? regular P waves? normal
PR interval? 0.36 s QRS duration? 0.08 s Interpretation? 1st Degree AV Block

102
1st Degree AV Block Deviation from NSR PR Interval > 0.20 s

103
1st Degree AV Block Etiology: Prolonged conduction delay in the AV node or Bundle of His.

104
Rhythm #8 Rate? 50 bpm Regularity? regularly irregular P waves?
nl, but 4th no QRS PR interval? lengthens QRS duration? 0.08 s Interpretation? 2nd Degree AV Block, Type I

105
2nd Degree AV Block, Type I
Deviation from NSR PR interval progressively lengthens, then the impulse is completely blocked (P wave not followed by QRS).
.")
106
2nd Degree AV Block, Type I
Etiology: Each successive atrial impulse encounters a longer and longer delay in the AV node until one impulse (usually the 3rd or 4th) fails to make it through the AV node.
 fails to make it through the AV node.")
107
Rhythm #9 Rate? 40 bpm Regularity? regular P waves? nl, 2 of 3 no QRS
PR interval? 0.14 s QRS duration? 0.08 s Interpretation? 2nd Degree AV Block, Type II

108
2nd Degree AV Block, Type II
Deviation from NSR Occasional P waves are completely blocked (P wave not followed by QRS).
.")
109
2nd Degree AV Block, Type II
Etiology: Conduction is all or nothing (no prolongation of PR interval); typically block occurs in the Bundle of His.
; typically block occurs in the Bundle of His.")
110
Rhythm #10 Rate? 40 bpm Regularity? regular P waves?
no relation to QRS PR interval? none QRS duration? wide (> 0.12 s) Interpretation? 3rd Degree AV Block
 Interpretation 3rd Degree AV Block.")
111
3rd Degree AV Block Deviation from NSR
The P waves are completely blocked in the AV junction; QRS complexes originate independently from below the junction.

112
3rd Degree AV Block Etiology: There is complete block of conduction in the AV junction, so the atria and ventricles form impulses independently of each other. Without impulses from the atria, the ventricles own intrinsic pacemaker kicks in at around beats/minute.

113
Remember When an impulse originates in a ventricle, conduction through the ventricles will be inefficient and the QRS will be wide and bizarre.

114
VT

115
VF

116
Summary of Arrhythmias & Blocks Supraventricular
Atrial Sinus Tach (>100) Sinus Brady (<60) Sinus Arrest PAC Atrial Tach ( ) Atrial Flutter ( ) Atrial Fib Wandering Atrial Pacemaker Multifocal Atrial Tachycardia AV Nodal PSVT Blocks 1st Degree 2nd Degree Mobitz I (Wenchebach) Mobitz II 3rd Degree Junctional Junctional Escape (40-60) Accelerated Junctional
 Sinus Brady (<60) Sinus Arrest. PAC. Atrial Tach ( ) Atrial Flutter ( ) Atrial Fib. Wandering Atrial Pacemaker. Multifocal Atrial Tachycardia. AV Nodal. PSVT. Blocks. 1st Degree. 2nd Degree. Mobitz I (Wenchebach) Mobitz II. 3rd Degree. Junctional. Junctional Escape (40-60) Accelerated Junctional.")
117
Summary of Arrhythmias & Blocks Ventricular
PVC V Tach Unifocal Multifocal (Torsade de Pointe) V Fib Idioventricular Rhythm (20-40) Blocks Left Bundle Branch Left anterior fascicular block Left posterior fascicular block Right Bundle Branch
 V Fib. Idioventricular Rhythm (20-40) Blocks. Left Bundle Branch. Left anterior fascicular block. Left posterior fascicular block. Right Bundle Branch.")
118
ECG Case Studies

119
56 y.o. male here for preop clearance for TKR. Hx of HTN

120
23 y.o. female presents with “racing heart”

121
72 y.o. male presents with dizziness

122
80 y.o. female presents with SOB and fatigue
A flutter Left axis deviation

123
46 y.o male presents with sternal CP

124
65 y.o. male with diabetes presents with nausea, abdominal pain

125
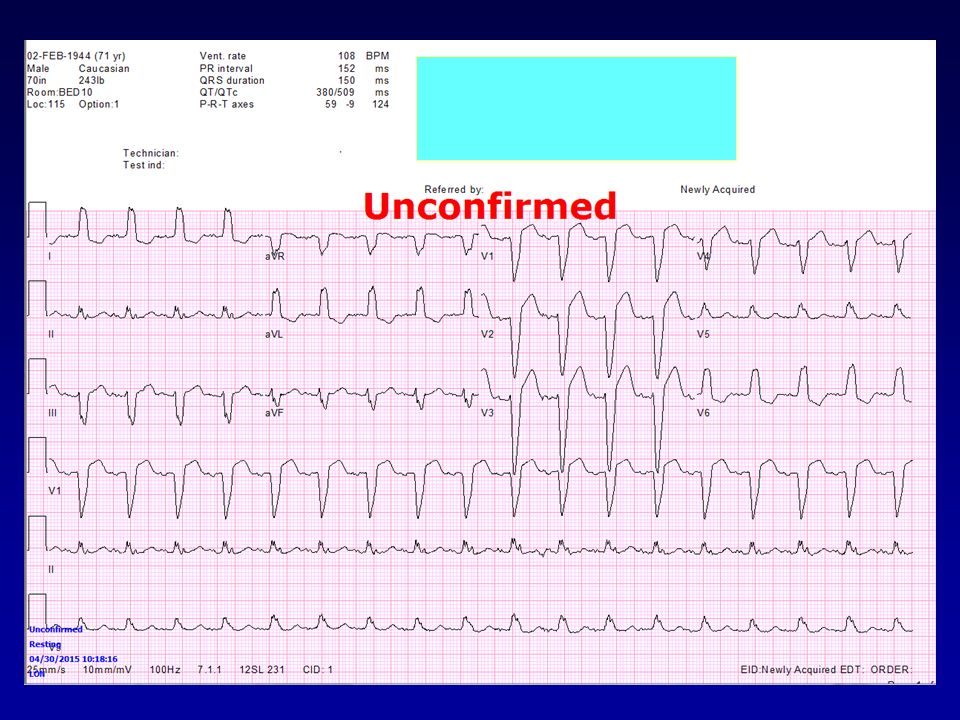
65M with asystolic cardiac arrest with Epi, bicarb, and chest compressions. He was in shock
Hyperkalemia, pH 6.6, post code

126
45M admitted with on-and-off chest pain

127
29F from Jamaica with sharp constant chest pain

Similar presentations






















>")
