Download presentation
Presentation is loading. Please wait.

1
Are hospital readmissions in the elderly preventable? Antonio Sarría-Santamera MD PhD Institute of Health Carlos III University of Alcalá DUKE-NUS HSSR SEMINAR May 29 th, 2015

2
The Spanish health care system Should we care about this problem? What we did Some reflections

3
Spanish Health Care System National Health Care System Network of hospitals-specialists/GPs-PC centers Population based budget Doctors are salaried GPS: Gate-keeping for specialists Free at the point of service (no copayments for medical services) Copayment for medicines prescribed for ambulatory patients
 Copayment for medicines prescribed for ambulatory patients")
4
Prevention is worth The condition sought should be an important health problem There should be an accepted treatment. Facilities for diagnosis and treatment should be available. There should be a recognizable latent or early symptomatic stage. There should be a suitable test or examination. The test should be acceptable to the population. The natural history of the condition, including development from latent to declared disease, should be adequately understood. There should be an agreed policy on whom to treat as patients. The cost of case-finding (including diagnosis and treatment of patients diagnosed) should be economically balanced in relation to possible expenditure on medical care as a whole. Case-finding should be a continuing process and not a “once and for all” project. Wilson. JMG, Jungner G. Principles and practice of screening for disease. Geneva: WHO; 1968
 should be economically balanced in relation to possible expenditure on medical care as a whole. Case-finding should be a continuing process and not a once and for all project. Wilson. JMG, Jungner G. Principles and practice of screening for disease. Geneva: WHO;")
5
ARE READMISSIONS IN THE ELDERLY A PUBLIC HEALTH PROBLEM?

6
Evolution hospital readmissions

7
Hospital readmissions for specific conditions COPD HEART FAILURE

8
Hospital readmissions by age groups

9
Readmissions >74 year old

11
Complexity Aging, clinical conditions and functional status Social conditions Utilization of services Relationships across professionals and levels of care Methodological approaches

12
Observational study Systematic review of evidence Qualitative study

13
COHORT STUDY

14
METHODS Patients >74 year old discharged from HUPA Index admission: no admission in the previous 6 months All patients were followed for 6 months. Source of information: – EMR PC + hospital

15
RESULTS 1.051 included 22,6% readmission in 6 months after the index admission Variables associated with an increased risk: – LOS – Number of prescriptions – Hypertension – Heart failure – Ischemic heart disease Variables associated with a protective effect: – Visits at nurses at PC

16
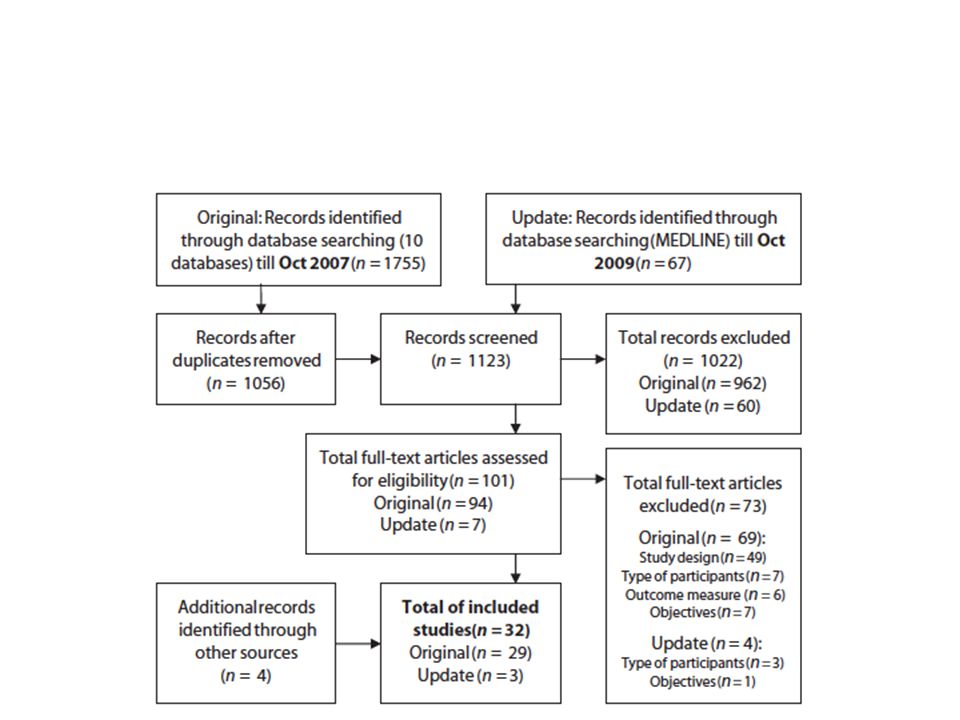
SYSTEMATIC REVIEW FACTORS ASSOCIATED WITH READMISSIONS

17
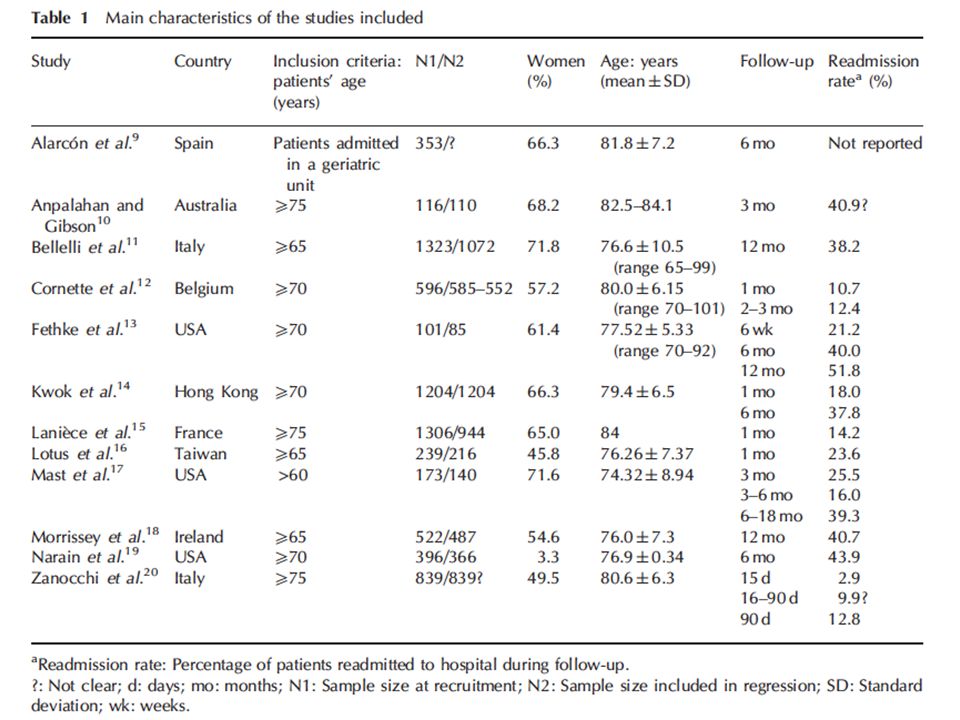
Inclusion criteria Prospective studies with appropriate statistical analysis, that explored the relationship between risk of readmission with clinical, socio-demographic or other factors in elderly patients (aged at least 75 years) admitted to hospital.
 admitted to hospital.")
18
Exclusion criteria Studies that focused on patients with specific diseases or conditions (terminal patients, psychiatric patients, heart failure, chronic obstructive pulmonary disease, etc.) Studies where >50% of the patients or the average age was <75 years.
 Studies where >50% of the patients or the average age was <75 years.")
21
LIMITATIONS Methodological aspects Different periods of time: – Short (2 weeks-30 days) – Long (2-3 months)
 – Long (2-3 months)")
22
FACTORS ASSOCIATED WITH READMISSION 1.An admission before the index admission 2.Length of stay 3.Multi-morbidity poly-pharmacy 4.Functional capacity 5.Social factors

23
Systematic review Functional status score, illness severity, co- morbidity, polypharmacy, and age. Campbell. Age and Ageing 2004; 33: 110–115

24
SYSTEMATIC REVIEW EFFECTIVE INTERVENTIONS TO PREVENT READMISSION

25
Inclusion criteria Controlled trials, both randomized as well as nonrandomized, which assessed an intervention carried out during admission and/or the follow-up in order to reduce readmissions of elderly patients admitted to hospital for any medical problem (studies focusing on a specific disease were excluded). One of the outcome measures (not necessarily the primary one) had to be unplanned hospital readmission (absolute differences, risk ratio, odds ratio). Studies were excluded if more than half of participants were younger than 75 years or if the average age of all participants was less than 75 years.
 had to be unplanned hospital readmission (absolute differences, risk ratio, odds ratio). Studies were excluded if more than half of participants were younger than 75 years or if the average age of all participants was less than 75 years..")
27
LIMITATIONS Complexity and variability of the interventions reviewed in this work, and of their methodologies: it was not possible to make direct comparisons between studies. Strong variability in the indicators used to measure readmissions, which can be expressed in terms of the number (or percentage) of events or the number of patients readmitted during a given period. Some studies measured the number of days from the admission to the first readmission, others counted patients according to their number of readmissions. Distinct lengths of the follow-up period and of the measurement times, which ranged from 15 days to 1 year post discharge. Differences in the treatment provided to the control groups, although the majority of the studies compared the intervention with ‘usual care’ (almost never described in detail). Hence, this care may vary according to the health care system of each country and it may include some components of geriatric management.
 of events or the number of patients readmitted during a given period. Some studies measured the number of days from the admission to the first readmission, others counted patients according to their number of readmissions. Distinct lengths of the follow-up period and of the measurement times, which ranged from 15 days to 1 year post discharge. Differences in the treatment provided to the control groups, although the majority of the studies compared the intervention with ‘usual care’ (almost never described in detail). Hence, this care may vary according to the health care system of each country and it may include some components of geriatric management..")
28
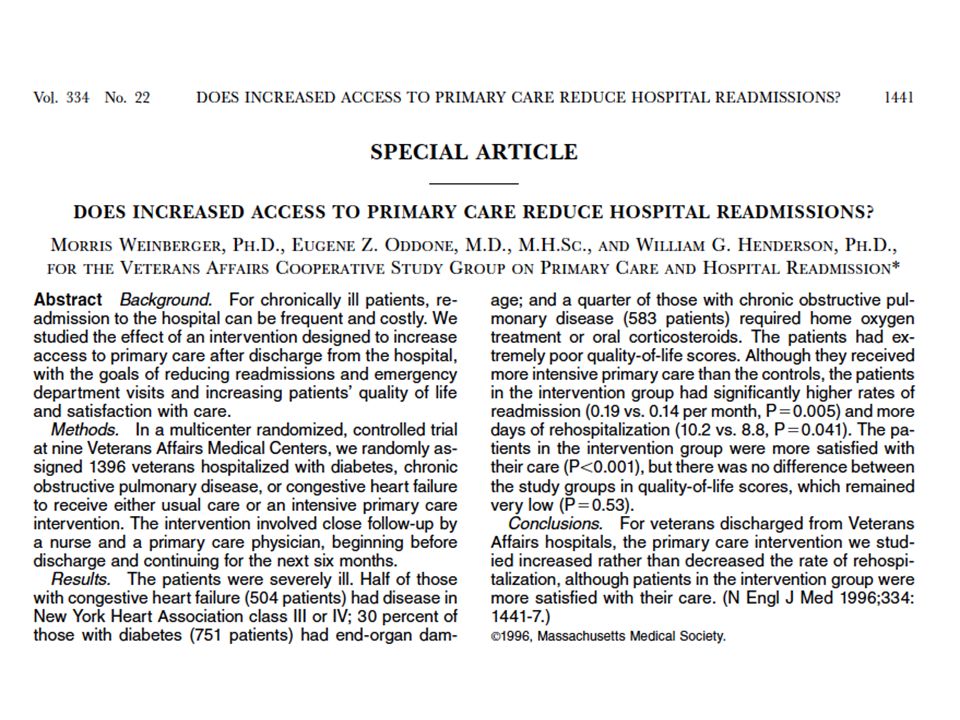
EFFECTIVE INTERVENTIONS 1.Coordination hospital-PC 2.Home care component

29
Interventions with many components, involving more individuals in care delivery, and supporting patient capacity for self-care. Leppin AL. JAMA Intern Med. 2014 Jul;174(7):1095-107
:")
30
Home or community care of patients led to a significant reduction of readmissions. Benbassat. Israel Journal of Health Policy Research 2013, 2:1

31
QUALITATIVE STUDY

32
Qualitative study: problems No formal communication between PC and hospitals EMR in PC is connected with EMR in hospitals, but there is no information PC receive when a patient is admitted to the hospital Information from patients when they are discharged Patients have new medicines prescribed PC have to reevaluate patients based on the new information Believe that at the hospital there is a view of hospitalizations as acute events, not as a manifestation of the continuous process of losing functional capacity There is the possibility of home visits, but the lack of communication limits an appropriate scheduling Continuity of care of a continuous process limited by this communication barrier

33
Qualitative study: proposals Individualize care to specific patient situation Improve opportunities for home care Self-management Coordinated and shared care between PC- hospitals

34
COMMENTS

36
Questions Are hospital readmissions in the elderly preventable? Hospital readmissions measure hospital quality? Do we really know the “natural history” of the disabilitating process related with the advancement of chronic conditions?

37
Are readmissions preventable? Systematic review

38
Complex interventions MRC Difficulty of standardizing the design and delivery of the interventions. Sensitivity to features of the local context. Organizational and logistical difficulty of applying experimental methods to service or policy change. Length and complexity of the causal chains linking intervention with outcome.

39
CONCLUSIONS Increased risk of readmission: – Short term: 1.Number of previous hospital admissions 2.Length of stay – Long term: 1.Multi-morbidity/poly-pharmacy 2.Functional capacity 3.Social factors Effective preventive interventions: 1.Coordination hospital-PC 2.Home care component 3.Self-management

40
Systemic perspective The process of care can not be fragmented into different to some extent independent components. Most of the factors associated with a higher risk of readmission require to take into consideration a broad systemic approach. The specific characteristics of how to resolve this problem are yet to be understood

Similar presentations





 Dr Ian Williams Greater Metro South Brisbane Medicare.>")





 Data: A Researcher’s Perspective Judith H. Lichtman, PhD MPH Associate.>")


 Hsiao,>")





