Download presentation
Presentation is loading. Please wait.

1
Electrodiagnostic Studies (more than you ever cared to know)
Pete Vonderau, MD Physical Medicine and Rehabilitation THE REHAB DOCTORS

2
Objectives Review pertinent neuromusculoskeletal anatomy
Explain how nerve conduction studies and needle examinations are performed Review common indications for NCS/EMG studies

3
Electrodiagnostic Studies
Two parts (often collectively referred to as “EMG”) Nerve Conduction Studies = Nerve Stimulation EMG (Electromyography) = Needle Exam Why is it performed? To evaluate nerve function (assess for nerve or muscle injury) MRI only evaluates structure Also for localization of injury, severity, prognosis, ruling out other disease Commonly indicated for peripheral nerve injury Performed by physiatrists and neurologists
 Nerve Conduction Studies = Nerve Stimulation. EMG (Electromyography) = Needle Exam. Why is it performed To evaluate nerve function (assess for nerve or muscle injury) MRI only evaluates structure. Also for localization of injury, severity, prognosis, ruling out other disease. Commonly indicated for peripheral nerve injury. Performed by physiatrists and neurologists.")
4
Interpreting EMG/NCS studies requires a solid understanding of Neuromusculoskeletal Anatomy

5
Spine Anatomy Primary motor neuron is the anterior horn cell
Resides in the ventral gray matter of SC Axons exit as motor roots, combine to form peripheral nerves, innervate muscle Primary sensory neuron is DRG Resides in intervertebral foramen Accepts sensory input from body via pre-ganglionic fibers Spinal nerves Composed of ventral (motor) and dorsal (sensory) nerve roots Divides into dorsal and ventral rami Ventral rami combine to form plexuses
 and dorsal (sensory) nerve roots. Divides into dorsal and ventral rami. Ventral rami combine to form plexuses.")
6
Nerve Anatomy Each motor (AHC) or sensory neuron (DRG) has one axon (fiber through which impulses are sent) Each axon surrounded by Schwann cell (makes myelin) Motor axons and large sensory axons (proprioception) are myelinated (electrically insulated) Small nerves lack insulation (pain, temperature, autonomic) Axons are bundled into fascicles Peripheral Nerve is composed of many fascicles
 Motor axons and large sensory axons (proprioception) are myelinated (electrically insulated) Small nerves lack insulation (pain, temperature, autonomic) Axons are bundled into fascicles. Peripheral Nerve is composed of many fascicles.")
7
Nerve Physiology All Cells (including axons of neurons) maintain an Equilibrium Potential Na/K Pump, cell membrane permeability, and diffusion potentials work together, resulting in the inside of the cell having a negative potential compared to outside (-70mV)
")
8
Nerve Physiology: Conduction
Nerves transmit information via Action Potentials Electrical stimulation of nerve causes inside to become more + Threshold reached at which voltage-gated Na+ channels open briefly, charge inside ↑ rapidly (cell depolarizes) Na+ flows down nerve to propagate the action potential along nerve (voltage change) Then gates close and membrane potential increases again This AP can be measured
 Na+ flows down nerve to propagate the action potential along nerve (voltage change) Then gates close and membrane potential increases again. This AP can be measured.")
9
Nerve Physiology: Saltatory Conduction
A Schwann cell surrounds each axon and can myelinate the axon Myelin electrically insulates motor axons and larger sensory axons (not small sensory fibers) Na+ channels are not continuous down nerve but are clustered at Nodes of Ranvier Conduction jumps from node to node, which is much faster than unmyelinated nerves (10-20x)
 Na+ channels are not continuous down nerve but are clustered at Nodes of Ranvier. Conduction jumps from node to node, which is much faster than unmyelinated nerves (10-20x)")
10
Motor Nerves: Muscle Contraction
Signal sent from AHC in spinal cord, down axon At the Neuromuscular Junction, Ach is released Ach binds muscle membrane, opening Na+ channels, thus depolarizing muscle fiber membrane (voltage change) Sarcoplasmic reticulum releases Ca++, which binds troponin to start muscle contraction via overlap of actin and myosin
 Sarcoplasmic reticulum releases Ca++, which binds troponin to start muscle contraction via overlap of actin and myosin.")
11
Motor Unit Skeletal muscle composed of many fascicles Motor Unit
Fascicles contain thousands of muscle fibers (muscle cells) Motor Unit Defined as the motor neuron, its axon, and the muscle fibers it innervates These fibers depolarize nearly simultaneously, creating a motor unit action potential (electric potential) We can place a needle into the muscle and measure this electric potential
 Motor Unit. Defined as the motor neuron, its axon, and the muscle fibers it innervates. These fibers depolarize nearly simultaneously, creating a motor unit action potential (electric potential) We can place a needle into the muscle and measure this electric potential.")
12
Sensory Nerves Activated by sensory input
Mechanoreceptors Light touch, pressure, muscle stretch (proprioception) Myelinated fibers Nociceptors Pain (unmyelinated) Thermoreceptors Temperature (unmyelinated) Action potentials travel proximally to the DRG, then on to spinal cord
 Myelinated fibers. Nociceptors. Pain (unmyelinated) Thermoreceptors. Temperature (unmyelinated) Action potentials travel proximally to the DRG, then on to spinal cord.")
13
Nerve Conduction Studies

14
Nerve Stimulation We can stimulate a nerve by sending negative charges around the nerve Reduces the resting membrane potential and cause the action potential to start anywhere along the nerve Motor or sensory nerves can be stimulated Stimulating a motor nerve can result in muscle contraction Stimulating a sensory nerve gives a buzzing sensation We attempt to stimulate all of the axon fibers of the target nerve

15
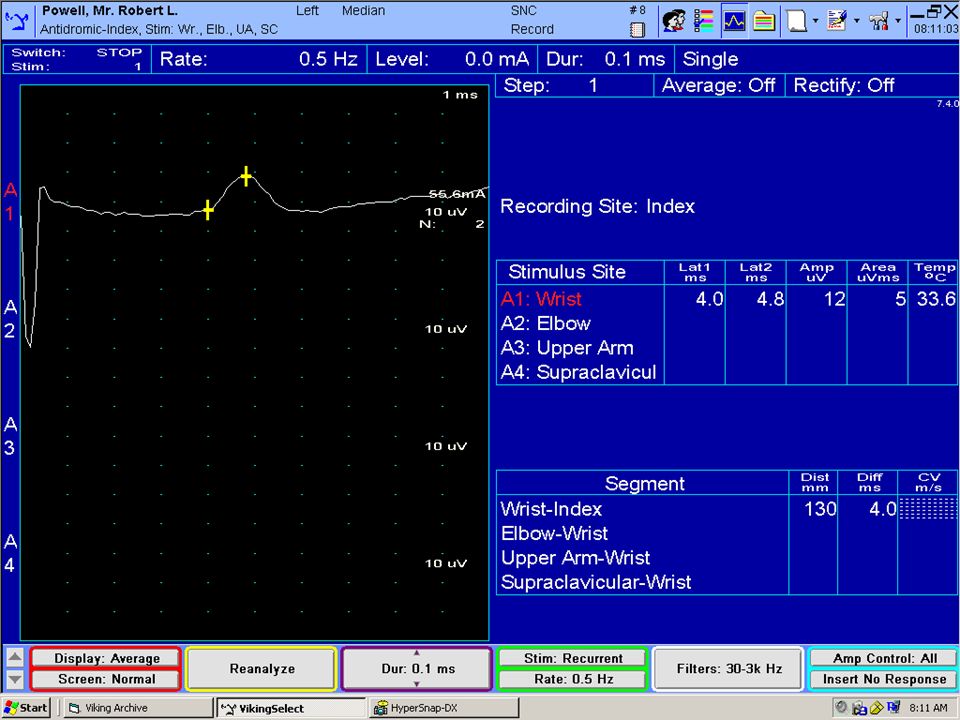
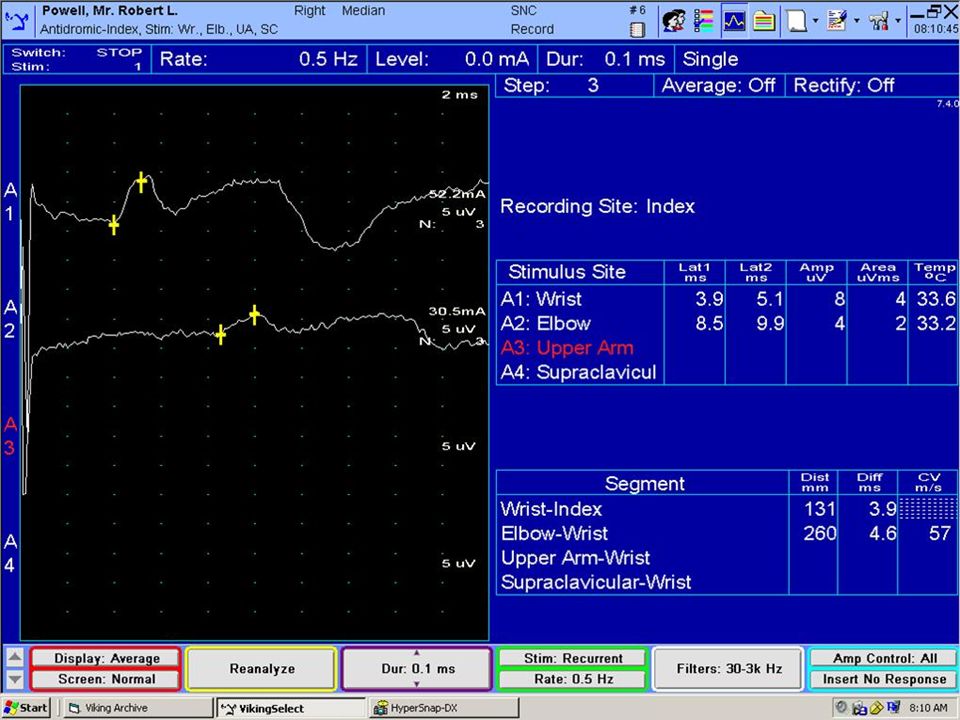
Sensory Nerve Conduction Studies
We measure the electric potentials farther along the nerve with skin electrodes The computer amplifies the potentials and records them on the computer screen Recorded values Distal latency (conduction time over distal limb to electrodes) Amplitudes (functioning axons) Conduction Velocity (dist/time) Compare to normal values or other limb
 Amplitudes (functioning axons) Conduction Velocity (dist/time) Compare to normal values or other limb.")
16
Sensory Nerve Conduction Studies: Uses
Most sensitive for focal mononeuropathies (CTS) Sensory nerves more prone to injury The only test for pure sensory cutaneous nerve (cheiralgia paresthetica) Sensory peripheral neuropathy Localization: Separating pre-DRG from post-DRG injury Sensory NCS will be normal if lesion proximal to DRG
 Sensory nerves more prone to injury. The only test for pure sensory cutaneous nerve (cheiralgia paresthetica) Sensory peripheral neuropathy. Localization: Separating pre-DRG from post-DRG injury. Sensory NCS will be normal if lesion proximal to DRG.")
17
Normal Values (Sensory NCS)
Sensory Nerve Distal Latency Amplitude Cond. Veloc. Median Antidromic (II) <3.6 msec >15 μV >56 m/s Ulnar Antidromic (V) <3.1 msec >10 μV >54 m/s Median Palmar <2.3 msec >50 μV Ulnar Palmar >55 m/s Diff ≤ 0.3 Dorsal Ulnar Cutaneous <2.6 msec >8 μV Superficial Radial Antidromic <2.9 msec >20 μV >49 m/s
 <3.6 msec. >15 μV. >56 m/s. Ulnar Antidromic (V) <3.1 msec. >10 μV. >54 m/s. Median Palmar. <2.3 msec. >50 μV. Ulnar Palmar. >55 m/s. Diff ≤ 0.3. Dorsal Ulnar Cutaneous. <2.6 msec. >8 μV Superficial Radial Antidromic. <2.9 msec. >20 μV. >49 m/s.")
19
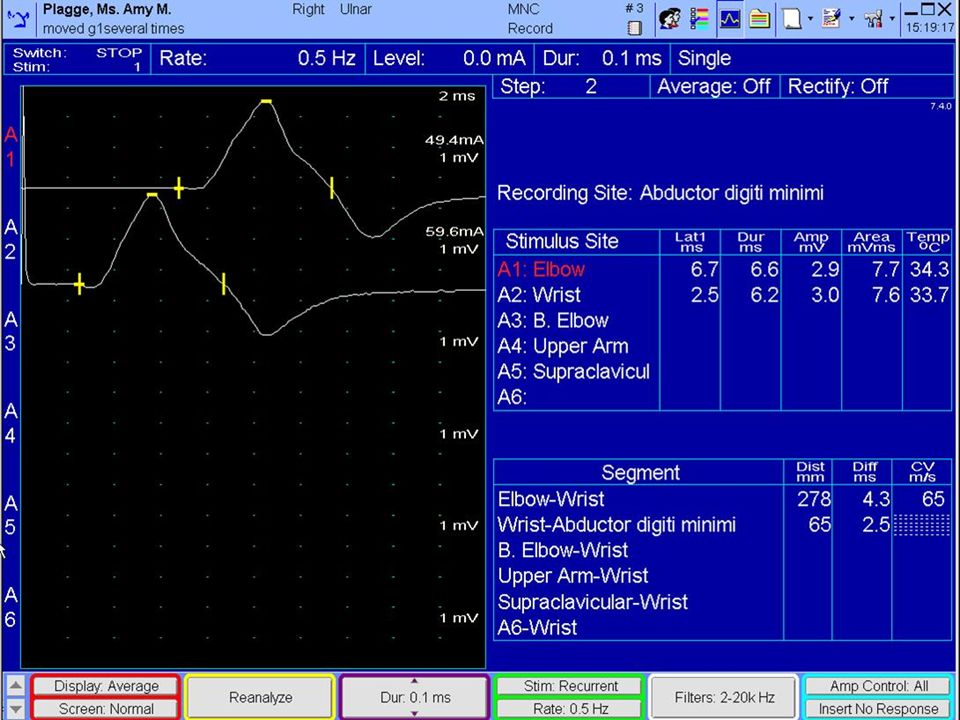
Motor Nerve Conduction Studies
Stimulate over a motor nerve Action Potential travels down motor nerve, depolarizes muscle, resulting in a muscle contraction The electric potential (mV) from muscle contraction is recorded on the skin over the muscle belly Attempt to activate all the axons of the nerve Increase stimulation until amplitude no longer increases
 from muscle contraction is recorded on the skin over the muscle belly. Attempt to activate all the axons of the nerve. Increase stimulation until amplitude no longer increases.")
20
Motor Nerve Conduction Studies: Measurements
Motor Distal Latency: reflects time for nerve conduction + NMJ transmission + Muscle conduction Amplitude: reflects the summation of potentials from all functioning motor units Amplitudes can be low due to injury to AHC, nerve root, peripheral nerve axon, demyelination, NMJ dysfunction, myopathies

21
Normal Values (Motor NCS)
Motor Nerve Dist. Lat. Amplitude Cond Velocity Median (APB) < 4.5 msec >4.0 mV >48 m/s Ulnar (ADM) <3.6 msec >6.0 mV >51 m/s Radial (EDC) <3.1 msec >67 m/s Peroneal (EDB) <6.6 msec >2.0 mV >41 m/s Tibial (AH) <6.1 msec >40 m/s
 < 4.5 msec. >4.0 mV. >48 m/s. Ulnar (ADM) <3.6 msec. >6.0 mV. >51 m/s. Radial (EDC) <3.1 msec >67 m/s. Peroneal (EDB) <6.6 msec. >2.0 mV. >41 m/s. Tibial (AH) <6.1 msec. >40 m/s.")
23
F waves This is a way of assessing the proximal motor nerve
With distal stimulation, 1-2% of motor fibers will carry signal proximally to SC, then back down to muscle We can measure the latency (response time) Prolonged latency may be due to proximal nerve injury: radiculopathy, plexopathy, GBS Not a very sensitive test
 Prolonged latency may be due to proximal nerve injury: radiculopathy, plexopathy, GBS. Not a very sensitive test.")
24
Pathophysiology: Axonal Injury
AKA Axonotmesis “Defective wires” Individual axons no longer function Fewer axons remain within each nerve fascicle For sensory nerves, there may be some impairment of sensation (numbness, tingling, absent reflexes) For motor nerves, there may be weakness and ATROPHY Atrophy due to muscle cells no longer being innervated
 For motor nerves, there may be weakness and ATROPHY. Atrophy due to muscle cells no longer being innervated.")
25
Pathophysiology: Axonal Injury
Causes Nerve trauma or compresssion, metabolic disorders (DM), congenital disease, etc Nerve Conduction Studies Low amplitudes, both proximal and distal Amplitude loss proportional to axon loss Complete nerve trans-section results in no distal response Relatively preserved DL and CV Prognosis Guarded Intact axons can slowly sprout to denervated muscle fibers
, congenital disease, etc. Nerve Conduction Studies. Low amplitudes, both proximal and distal. Amplitude loss proportional to axon loss. Complete nerve trans-section results in no distal response. Relatively preserved DL and CV. Prognosis. Guarded. Intact axons can slowly sprout to denervated muscle fibers.")
26
Pathophysiology: Demyelinating Injury
AKA Neurapraxia “Defective insulation” Axons are intact, but the myelin sheath (insulation) is damaged May result in numbness or tingling (sensory nerves), or weakness (motor nerves) but NO atrophy because the axon is still intact
 is damaged. May result in numbness or tingling (sensory nerves), or weakness (motor nerves) but NO atrophy because the axon is still intact.")
27
Demyelinating Injury: NCS
Stimulating PROXIMAL to injury reveals slowed CV and prolonged DL Low proximal amplitude if conduction block (complete conduction block possible=no proximal response) Stimulating distal to the lesion will elicit a normal response If you cannot stimulate proximal to the lesion, NCS will be normal (radic) Causes: compression, ischemia, autoimmune, congenital disorders Prognosis is good if nerve can be decompressed (remyelination often occurs over 4-6 weeks)
 Stimulating distal to the lesion will elicit a normal response. If you cannot stimulate proximal to the lesion, NCS will be normal (radic) Causes: compression, ischemia, autoimmune, congenital disorders. Prognosis is good if nerve can be decompressed (remyelination often occurs over 4-6 weeks)")
28
NCS Examples A: Normal B: Axonal Loss C: Uniform Demyelination
Low amplitude prox & distal, Normal DL Poor prognosis C: Uniform Demyelination Prolonged DL, Slow CV, normal amplitude (seen in CMT) D: Focal Demyelination with Conduction Block Low amplitude with proximal stimulation, slow CV, temporal dispersion Better prognosis than B
 D: Focal Demyelination with Conduction Block. Low amplitude with proximal stimulation, slow CV, temporal dispersion. Better prognosis than B.")
29
Needle Exam This is done to analyze the electrical activity of voluntary muscle A needle electrode is placed into the muscle Extracellular potentials created by muscle depolarization are recorded, then amplified and converted to audible sound Electrical activity is assessed at rest and while the muscle is contracted

30
Needle Exam: Spontaneous Activity
Muscle at rest (not contracting) is at electrochemical equilibrium There are no action potentials, so the needle should record no activity (silence) Axonal Injury (Denervation injury) Due to injury to AHC, nerve root, peripheral nerve Muscle fibers that lack innervation will fire spontaneously in an regular pattern called a fibrillation potential (abnormal) Takes 3-4 weeks for these to develop, resolve if sprouting occurs Demyelinating disorders will NOT cause fibrillation potentials
 is at electrochemical equilibrium. There are no action potentials, so the needle should record no activity (silence) Axonal Injury (Denervation injury) Due to injury to AHC, nerve root, peripheral nerve. Muscle fibers that lack innervation will fire spontaneously in an regular pattern called a fibrillation potential (abnormal) Takes 3-4 weeks for these to develop, resolve if sprouting occurs. Demyelinating disorders will NOT cause fibrillation potentials.")
31
Needle Exam: Fibrillation Potentials

32
Needle Exam: Voluntary Activity
Ask patient to contract muscle Needle records extracellular potentials from one motor unit (all fibers innervated by one axon), all firing in near synchrony near the needle tip Amplified and displayed on monitor
, all firing in near synchrony near the needle tip. Amplified and displayed on monitor.")
33
Needle Exam: Voluntary Activity
Assess the following: Number of units firing Frequency Duration of waveform Configuration of waveform Biphasic, Triphasic Phases Amplitude Recruitment

34
Needle: Abnormal Voluntary Activity
Axonal Injury (Denervation) In the subacute period (4-6 weeks, get polyphasic motor unit potentials as other intact axons send new sprouts to denervated fibers, which must myelinate Beyond 6 weeks, the amplitude increases and duration increases as remaining intact axons now command more fibers at one time
 In the subacute period (4-6 weeks, get polyphasic motor unit potentials as other intact axons send new sprouts to denervated fibers, which must myelinate. Beyond 6 weeks, the amplitude increases and duration increases as remaining intact axons now command more fibers at one time.")
35
Radiculopathy This is injury to the spinal nerve root
Many causes, but most common is nerve impingement by herniated disc Impingement can affect ventral (motor) or dorsal (sensory) nerve root, or both Routine NCS of Lumbar Radic: Peroneal and Tibial Motor NCS with F Sural and Peroneal Sensory NCS Needle: Tibialis Anterior, Medial Gastrocnemius, Peroneus Longus, Vastus Medialis, TFL, Gluteus Maximus, Paraspinal muscles
 or dorsal (sensory) nerve root, or both. Routine NCS of Lumbar Radic: Peroneal and Tibial Motor NCS with F. Sural and Peroneal Sensory NCS. Needle: Tibialis Anterior, Medial Gastrocnemius, Peroneus Longus, Vastus Medialis, TFL, Gluteus Maximus, Paraspinal muscles.")
36
Radiculopathy Nerve Conduction Studies are often normal
Sensory studies are normal because the sensory nerve is proximal to the DRG Motor are normal unless there is a severe axonal injury (because muscles are innervated by multiple roots) So why do NCS? – to rule out plexus or peripheral nerve injury Needle examination is the key Axonal injury will demonstrate fibrillation potentials after 3-4 weeks Later, polyphasic motor unit potentials are seen, followed by long duration/high amplitude motor units Diagnosis requires abnormalities in at least 2 muscles innervated by same root but different nerves
 So why do NCS – to rule out plexus or peripheral nerve injury. Needle examination is the key. Axonal injury will demonstrate fibrillation potentials after 3-4 weeks. Later, polyphasic motor unit potentials are seen, followed by long duration/high amplitude motor units. Diagnosis requires abnormalities in at least 2 muscles innervated by same root but different nerves.")
37
Myotomes and Dermatomes
Iliopsoas L 2 3 4 Rectus Femoris Adductor Longus Gracilis Vastus Lateralis Vastus Medialis Tibialis Anterior L 4 5 EHL Peroneus Tertius L 5 1 EDB L 4 5 1 Peroneus Longus Internal Hamstrings (SM/ST) External Hamstring (BFLH) External Hamstring (BFSH) L 5 Gluteus Medius TFL Gluteus Maximus L 5 1 2 Tibialis Posterior FDL Abductor Hallucis S 1 2 Abductor Digiti Minimi Pedis Gastrocnemius (Medial) Gastrocnemius (Lateral) Soleus Reflexes Patellar L 3 4 Internal Hamstring L 5 Achilles S1
 External Hamstring (BFLH) External Hamstring (BFSH) L 5. Gluteus Medius. TFL. Gluteus Maximus. L Tibialis Posterior. FDL. Abductor Hallucis. S 1 2. Abductor Digiti Minimi Pedis. Gastrocnemius (Medial) Gastrocnemius (Lateral) Soleus. Reflexes. Patellar. L 3 4. Internal Hamstring. L 5. Achilles. S1.")
38
Radiculopathy: Caveats
Pure sensory radiculopathy will result in a normal study Pre-ganglionic fibers intact Pure demyelinating radiculopathy will result in a normal study What is the diagnostic sensitivity of EMG? Estimated to be 60-70% based upon AANEM review of literature

39
Carpal Tunnel Syndrome
Injury to the median nerve within the carpal tunnel of the wrist, typically due to compression Routine Study Sensory NCS: Median and Ulnar antidromics, Palmar studies Motor NCS: Median and Ulnar Motor with F waves Needle Exam: Deltoid, Triceps, Pronator Teres, FDI, APB Rule out ALS, Cervical radiculopathy, brachial plexopathy, proximal median neuropathy, peripheral neuropathy

42
Carpal Tunnel Syndrome: Classification
Mild CTS Prolonged sensory (or palmar) distal latency Compare median and ulnar palmar DL Reduced sensory (or palmar) amplitude Moderate CTS Prolonged motor distal latency Severe CTS Absent sensory response Reduced motor amplitude Needle evidence of fibrillation potentials or long duration/high amplitude motor unit potentials
 distal latency. Compare median and ulnar palmar DL. Reduced sensory (or palmar) amplitude. Moderate CTS. Prolonged motor distal latency. Severe CTS. Absent sensory response. Reduced motor amplitude. Needle evidence of fibrillation potentials or long duration/high amplitude motor unit potentials.")
43
Carpal Tunnel Syndrome
What is the diagnostic sensitivity of NCS? Sensory antidromics: 65% sensitivity for CTS Palmar studies: 74% sensitivity for CTS (Mayo)
")
44
Summary: What you need to know
EMG/NCS is useful to further evaluate complaints of numbness, tingling, weakness, and atrophy thought to be related to the peripheral nervous system Indications Peripheral nerve injury Carpal Tunnel Syndrome, Ulnar neuropathy, Peroneal Neuropathy Peripheral Neuropathy Plexopathy (Brachial, Lumbosacral) Radiculopathy Motor Neuron Disease (ALS) Myopathy NMJ Junction Disorders (Academic Centers?)
 Radiculopathy. Motor Neuron Disease (ALS) Myopathy. NMJ Junction Disorders (Academic Centers )")
45
What you need to know (Cont)
Wait 3-4 weeks after nerve injury before ordering an EMG test Fibrillation potentials take time to develop Anti-coagulation may limit needle examination Nerve conduction studies are falsely reduced in obese, edematous limbs EMG/NCS does not evaluate injury to the central nervous system (stroke, spinal cord injury, etc) EMG/NCS cannot assess for small fiber peripheral neuropathies (unmyelinated nerves) Demyelinating nerve injuries have a much better prognosis Improvement over 4-6 weeks if decompressed Axonal nerve injuries have a more guarded prognosis 1-2 years to see maximum improvement
 EMG/NCS cannot assess for small fiber peripheral neuropathies (unmyelinated nerves) Demyelinating nerve injuries have a much better prognosis. Improvement over 4-6 weeks if decompressed. Axonal nerve injuries have a more guarded prognosis. 1-2 years to see maximum improvement.")
46
My Perspective on EMG/NCS
A thorough history and comprehensive musculoskeletal exam will yield the diagnosis >90% of time EMG is useful in the following situations When the patient’s presentation is non-physiologic or their effort on exam is unreliable (EMG is objective) When imaging findings do not match clinical findings
 When imaging findings do not match clinical findings.")
47
Thank You!

Similar presentations








.>")











 )and Electromyography ( EMG) Dr Taha Sadig Ahmed Physiology Department, College of Medicine,>")