Download presentation
Presentation is loading. Please wait.

1
Urinary System Tutorial Glomerulonephritis

2
The renal biopsy Glomeruli Renal tubules and Interstitium Vasculature
Glomerulonephritis Renal tubules and Interstitium Acute tubular necrosis Acute interstitial nephritis Chronic tubulointerstitial nephritis Vasculature Nephrosclerosis Renal artery sclerosis

3
Normal structure of the glomerulus

4
Presentation of glomerular disease
Nephrotic syndrome / Proteinuria Proteinuria (> 3.5g protein / day) Hypoproteinaemia Oedema Hyperlipidaemia Nephritic syndrome / Haematuria Haematuria Lesser amounts of proteinuria Hypertension Progressive renal failure
 Hypoproteinaemia. Oedema. Hyperlipidaemia. Nephritic syndrome / Haematuria. Haematuria. Lesser amounts of proteinuria. Hypertension. Progressive renal failure.")
5
Pathogenesis of glomerular disease
Immune mediated Immune complex formation/deposition Intrinsic glomerular antigens (anti-GBM) Circulating antigens deposited in glomerulus (Membranous) Circulating immune complexes deposited in glomerulus Activation of complement Cytokine release Neutrophil / macrophage recruitment and activation Activation of coagulation system
 Circulating antigens deposited in glomerulus (Membranous) Circulating immune complexes deposited in glomerulus. Activation of complement. Cytokine release. Neutrophil / macrophage recruitment and activation. Activation of coagulation system.")
6
Pathogenesis of glomerular disease
Immune mediated Subepithelial immune complexes less inflammation BM alterations +/- podocyte damage Proteinuria Subendothelial immune complexes “inflammatory GN” more inflammation and cellular proliferation Vessel damage Haematuria BM complexes Either presentation, usually haematuria

7
Pathogenesis of glomerular disease
Non-immune mediated Activation of complement “inflammatory GN” like picture but no immune deposits Epithelial cell injury Toxins / cytokines / unknown factors Loss of foot processes Detachment from BM Proteinuria

8
Glomerular response to injury
Increased cells (Hypercellularity) Seen in “inflammatory diseases” Proliferation of mesangial and endothelial cells Inflammatory cells Proliferation of epithelial cells +/- crescent formation Increased matrix / connective tissue (Hyalinization / Fibrosis) Hyalinization = accumulation of pink homogenous material Plasma protein/BM/Mesangial matrix Eventually leads to Fibrosis Increased basement membrane Thickened capillary loops Increased BM / immune deposits
 Seen in inflammatory diseases Proliferation of mesangial and endothelial cells. Inflammatory cells. Proliferation of epithelial cells +/- crescent formation. Increased matrix / connective tissue (Hyalinization / Fibrosis) Hyalinization = accumulation of pink homogenous material. Plasma protein/BM/Mesangial matrix. Eventually leads to Fibrosis. Increased basement membrane. Thickened capillary loops. Increased BM / immune deposits.")
9
Investigation of glomerular disease
Histopathology / Light microscopy Glomeruli Hypercellularity Increased matrix / Hyalinization / Fibrosis) Thickened basement membrane Secondary changes in tubules/interstitium Amount of tubular atrophy and fibrosis is a sensitive indicator of prognosis Associated large vessel disease
 Thickened basement membrane. Secondary changes in tubules/interstitium. Amount of tubular atrophy and fibrosis is a sensitive indicator of prognosis. Associated large vessel disease.")
10
Investigation of glomerular disease
Immunofluorescence Formation of immune complexes with deposition of antibodies in glomerulus IgG, IgA, IgM Basement membrane, mesangium Linear or granular pattern Electron microscopy Changes in podocytes, basement membranes and mesangium Location and presence of immune deposits (subepithelial, subendothelial, basement membrane)
")
11
Classification of glomerular disease
How many glomeruli? Focal = only some glomeruli Diffuse = all glomeruli affected How much of a single glomerulus? Segmental = only part of the glomerulus Global = the entire glomerulus Primary vs Secondary primarily renal disease vs renal complication of systemic disease

12
Glomerular diseases associated with nephrotic syndrome
Primary Minimal change disease Membranous GN Focal segmental glomerulosclerosis (FSGS) Secondary Diabetic nephropathy Amyloidosis
 Secondary. Diabetic nephropathy. Amyloidosis.")
13
Glomerular diseases associated with nephritic syndrome
Primary Postinfectious / Diffuse proliferative GN Membranoproliferative GN IgA nephropathy (Mesangioproliferative GN) Crescentic GN Secondary HSP Systemic vasculitis SLE Systemic sclerosis
 Crescentic GN. Secondary. HSP. Systemic vasculitis. SLE. Systemic sclerosis.")
14
Causes of the nephrotic syndrome
(Minimal change disease)
")
15
Minimal change disease
Commonest cause of nephrotic syndrome in children Can occur in adults Characterised by Lack of glomerular changes on light microscopy Lack of immune deposits Good response to steroids Pathogenesis Circulating factor causing damage to podocytes (glomerular epithelial cells)
")
16
Minimal change disease
Light microscopy (LM) – Normal Immunofluorescence (IF) – Normal (no immune deposits) Electron microscopy (EM) – Fusion of podocyte foot processes
 – Normal. Immunofluorescence (IF) – Normal (no immune deposits) Electron microscopy (EM) – Fusion of podocyte foot processes.")
19
Membranous GN Commonest cause of nephrotic syndrome in adults
Idiopathic (85%) or secondary (15%) to: Neoplasms (lung, colon, melanoma) Autoimmune disease (SLE, thyroiditis) Infections (Hep B, syphilis, malaria) Drugs (Penicillamine, gold) 40% progress to chronic renal failure (CRF) Pathogenesis Subepithelial immune deposits Thickening of BM between deposits – eventually envelopes and covers the deposits
 or secondary (15%) to: Neoplasms (lung, colon, melanoma) Autoimmune disease (SLE, thyroiditis) Infections (Hep B, syphilis, malaria) Drugs (Penicillamine, gold) 40% progress to chronic renal failure (CRF) Pathogenesis. Subepithelial immune deposits. Thickening of BM between deposits – eventually envelopes and covers the deposits.")
20
Membranous GN Light microscopy (LM)
Thickened capillary BM BM spikes on silver stain Immunofluorescence (IF) – diffuse granular GBM staining Electron microscopy (EM) – subepithelial deposits
 – diffuse granular GBM staining. Electron microscopy (EM) – subepithelial deposits.")
25
FSGS Idiopathic or secondary to: Characterised by:
Other glomerular disease (IgA) Other renal disease (chronic reflux / pyelonephritis / interstitial nephritis) Systemic disorder (HIV) Drugs (Heroin) Characterised by: Sclerosis of portions of some, not all glomeruli Often progresses to chronic renal failure (CRF) Recurs in 25-50% renal transplants
 Other renal disease (chronic reflux / pyelonephritis / interstitial nephritis) Systemic disorder (HIV) Drugs (Heroin) Characterised by: Sclerosis of portions of some, not all glomeruli. Often progresses to chronic renal failure (CRF) Recurs in 25-50% renal transplants.")
26
FSGS Light microscopy (LM) Immunofluorescence (IF)
Focal segmental sclerosis Some normal glomeruli Immunofluorescence (IF) IgM and C3 deposition in sclerotic areas Electron microscopy (EM) Fusion of podocyte foot processes
 IgM and C3 deposition in sclerotic areas. Electron microscopy (EM) Fusion of podocyte foot processes.")
28
Postinfectious / Diffuse proliferative GN
Characterised by Onset 1 – 4 weeks after upper respiratory / cutaneous infection with Group A -haemolytic streptococci Can occur after a number of other bacterial, viral and parasitic infections Elevated antistreptococcal antibody and decreased C3 Secondary to anti-strep antibodies binding to glomerular components Usually resolves within 6 weeks

29
Postinfectious / Diffuse proliferative GN
Light microscopy (LM) Diffuse glomerular proliferation Immunofluorescence (IF) Granular BM IgG, IgM, C3 Electron microscopy (EM) Subepithelial deposits
 Diffuse glomerular proliferation. Immunofluorescence (IF) Granular BM IgG, IgM, C3. Electron microscopy (EM) Subepithelial deposits.")
32
Membranoproliferative GN
Type I: Immune complex disease Idiopathic or secondary to Neoplasm, Autoimmune disease, Infections, Drugs Subendothelial immune complexes Type II: Complement activation BM deposits (dense deposit disease) 50% progress to chronic renal failure (CRF) High recurrence rate in renal transplants Characterised by Thickened capillary loops Glomerular hypercellularity due to mesangial proliferation Mesangial interposition – double GBM’s (Type I)
 50% progress to chronic renal failure (CRF) High recurrence rate in renal transplants. Characterised by. Thickened capillary loops. Glomerular hypercellularity due to mesangial proliferation. Mesangial interposition – double GBM’s (Type I)")
33
Membranoproliferative GN
Light microscopy (LM) Mesangial proliferation Thickened capillary BM Double BM’s on silver stain (Type I) Immunofluorescence (IF) Type I: Granular BM and mesangial IgG, IgM, C3 Type II: Granular BM C3 Electron microscopy (EM) Type I: Subendothelial deposits and mesangial interposition Type II: Dense deposits in GBM
 Mesangial proliferation. Thickened capillary BM. Double BM’s on silver stain (Type I) Immunofluorescence (IF) Type I: Granular BM and mesangial IgG, IgM, C3. Type II: Granular BM C3. Electron microscopy (EM) Type I: Subendothelial deposits and mesangial interposition. Type II: Dense deposits in GBM.")
37
IgA Nephropathy Mesangioproliferative GN
Pathogenesis Increased mucosal IgA secretion in response to inhaled/ingested antigens Glomerular (mesangial) deposition of IgA Characterised by episodic haematuria following respiratory tract infections 50% progress to chronic renal failure (CRF) Recurs in 20-60% of transplants Varying histology
 deposition of IgA. Characterised by episodic haematuria following respiratory tract infections. 50% progress to chronic renal failure (CRF) Recurs in 20-60% of transplants. Varying histology.")
38
Mesangioproliferative GN
Light microscopy (LM) Increased mesangial matrix Mesangial proliferation Focal sclerosis (FSGS) Immunofluorescence (IF) – mesangial IgA Electron microscopy (EM) – mesangial deposits
 Increased mesangial matrix. Mesangial proliferation. Focal sclerosis (FSGS) Immunofluorescence (IF) – mesangial IgA. Electron microscopy (EM) – mesangial deposits.")
41
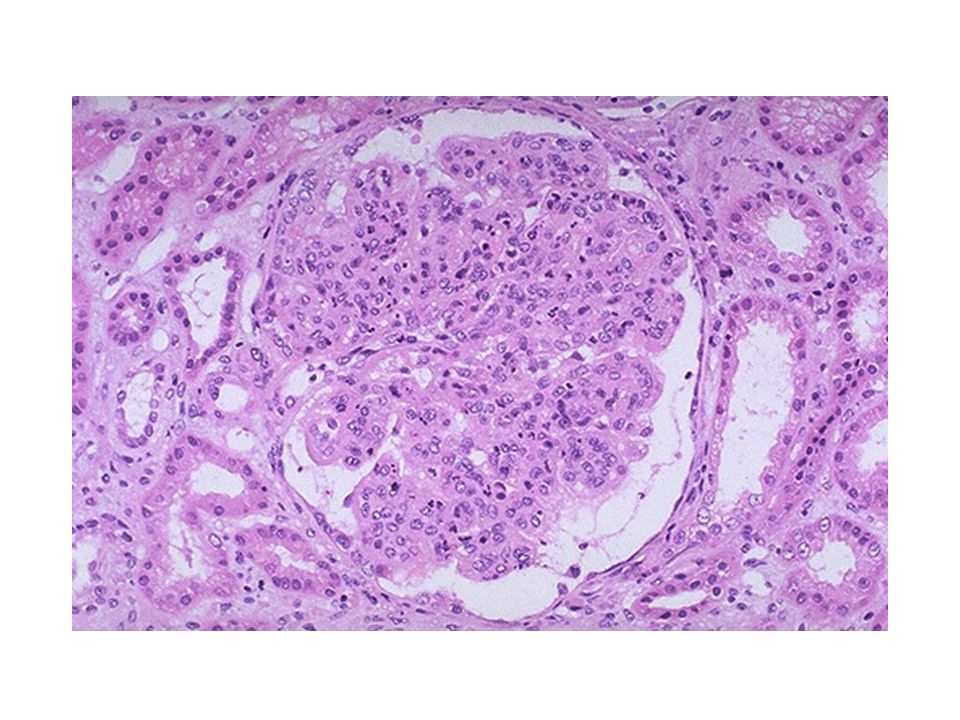
Crescentic GN Rapidly progressive GN
Characterised by Glomerular crescents Accumulation of cells in Bowman’s space Inflammatory cells, fibrin and epithelial cell proliferation Compression of glomerulus Rapidly progressive clinical course Pathogenesis Damage to glomerular vessels Egress of inflammatory cells and fibrin into Bowman’s space Proliferation of epithelial cells

42
Crescentic GN Rapidly progressive GN
Pathogenesis Type I – anti-GBM antibodies linear deposition of IgG May bind to alveolar BM in lung = Goodpasture’s disease Type II – immune complexes Idiopathic or secondary to autoimmune disease or other GN SLE HSP IgA nephropathy Postinfectious GN Type III – pauci-immune Idiopathic or secondary to systemic vasculitis Wegeners PAN

43
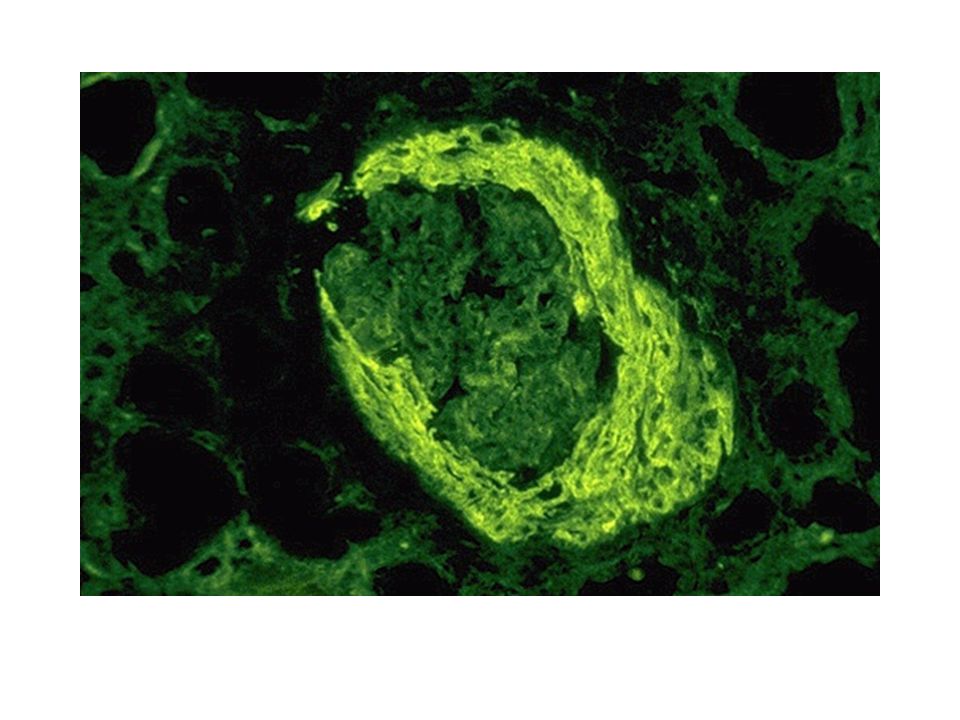
Crescentic GN Light microscopy (LM) Immunofluorescence (IF)
Cellular crescents of epithelium and inflammatory cells Fibrotic crescents Immunofluorescence (IF) Type I: linear IgG Type II: granular IgG Type III: no deposits Electron microscopy (EM) Type II: subendo, mesangial and subepi deposits
 Type I: linear IgG. Type II: granular IgG. Type III: no deposits. Electron microscopy (EM) Type II: subendo, mesangial and subepi deposits.")
Similar presentations



























 Membranous glomerulonephritis Focal segmental glomerulosclerosis.>")

 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")



 is the sudden onset of: – Haematuria (macroscopic/microscopic)>")

