Download presentation
Presentation is loading. Please wait.

1
WASHTENAW COUNTY PUBLIC HEALTH DIANA TORRES-BURGOS, MEDICAL DIRECTOR RICHARD FLEECE, INTERIM HEALTH OFFICER CINDRA JAMES, EP COORDINATOR WISD 8/5/09 H1N1 Influenza A Updates: Schools & Fall Flu Season

2
Overview H1N1 Influenza A and Seasonal Influenza H1N1 Activity Statistics and Updates Influenza Prevention Strategies Antivirals Vaccines Public Health Preparation & Planning School Preparation & Planning Recommendations Discussions/ Q & A

3
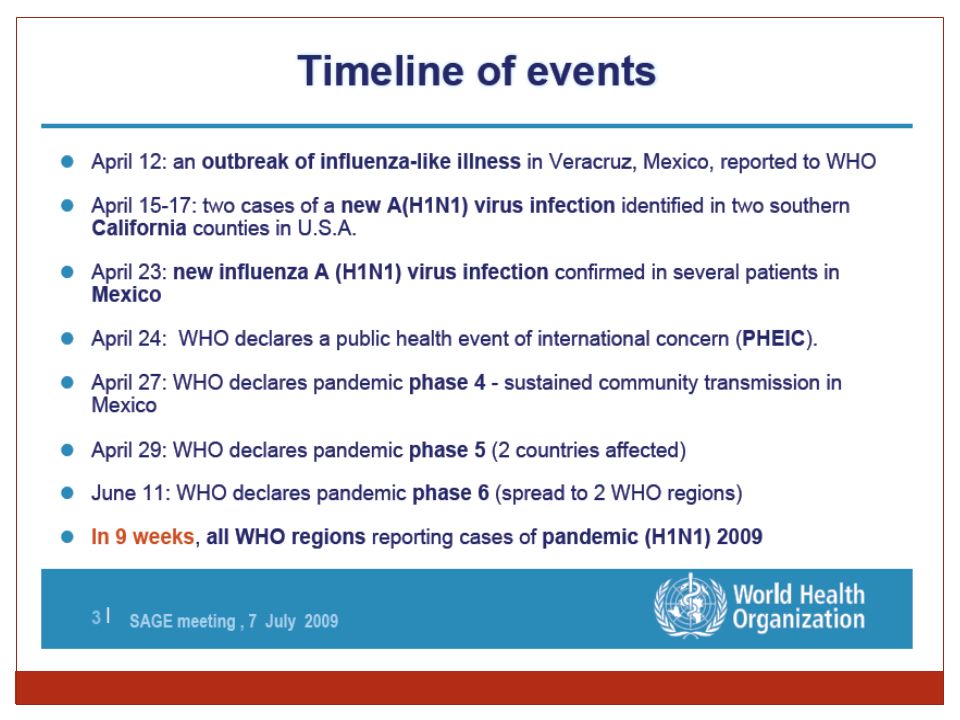
What is Novel Influenza A H1N1? Pandemic Influenza A H1N1 is a new strain of the flu that contains genetic fragments from birds, pigs, and humans and was first detected in April, 2009.

5
Signs and Symptoms Fever Cough Sore Throat Vomiting Body ache Diarrhea Lethargy

6
How does it spread? Thought to be spread in the same way that seasonal flu spreads Mainly from person to person when an infected person coughs or sneezes and spreads tiny particles into the air Sometimes by touching contaminated surfaces with flu viruses, and then touching one’s mouth, nose or eyes

7
How long is a person infectious and can spread to others? Up to 7 days after they become sick Children, especially infants, may be contagious for longer periods Viruses can live 2 - 8 hours on surfaces like tables, desks, and doorknobs On hard non porous surfaces may live up to 48-72 hours

8
Influenza A H1N1 and Seasonal Flu H1N1 influenza A is different from seasonal flu because: It is a new strain of the virus Most people do not have immunity to it Immunizations received last fall or this winter do not offer protection against the H1N1 swine flu Children and young adults at higher risk for disease and complications from H1N1

10
H1N1 Statistics Note: before reports changes* Confirmed and Probable cases Deaths International134,503*816 United States43,771*353 Michigan3,166*10 Washtenaw County940

11
US Hospitalizations and Deaths As of August 6 th, in U.S. - 6,506 hospitalizations and 436 deaths

12
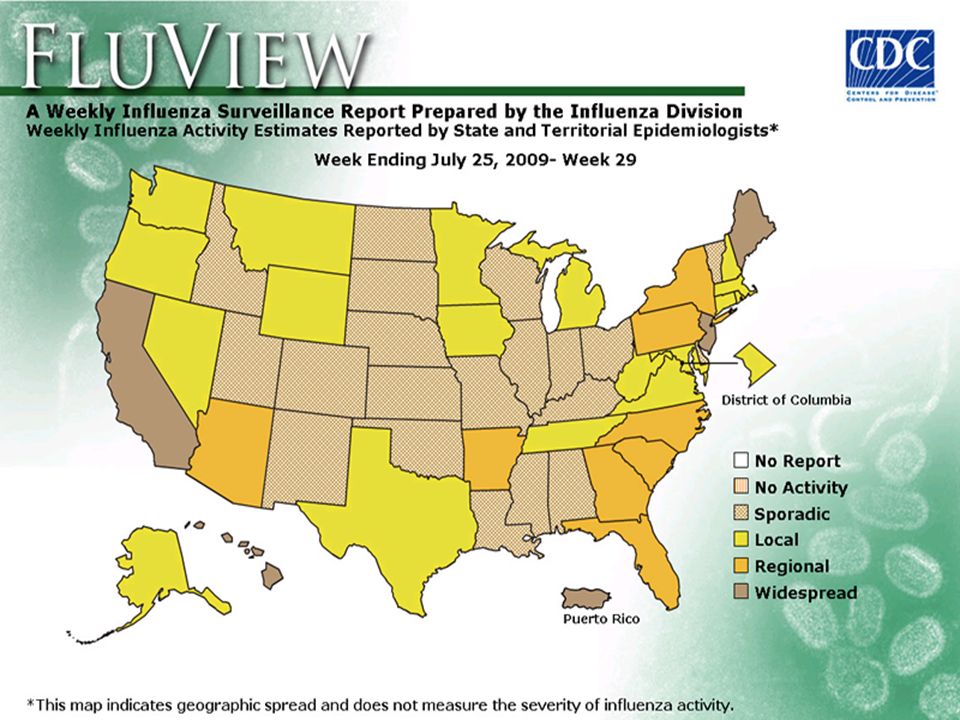
National Influenza Positive Tests

13
Respiratory illness in WC schools and Child Care

14
H1N1: What We Do Know Novel H1N1 viruses make up 99% of all influenza A viruses currently We are seeing co-circulation of seasonal H1N1, H3N2 and novel H1N1 virus, though in some places novel H1N1 virus are becoming dominant No change in virus characteristics or disease patterns Causes more severe pneumonia than seasonal flu

15
H1N1:What We Know-Cont’d Novel H1N1 transmission ongoing Majority of deaths in individuals with underlying medical conditions No significant difference in rates between males and females Most common underlying conditions: Asthma, Diabetes, and immune disorders Fourfold hospitalization in pregnant women

16
H1N1: What We Know-Cont’d Most reported cases: Highest in 5-24 years old, Next highest in the 0-4 year olds Lowest reported cases in 65+ years old Hospitalization rates: Highest in 0-4 years of age, Next highest 5-24 years, Lowest hospitalizations rates in 65+years old Death rates: Highest people aged 25-49 years of age (39%) Next highest people aged 50-64 (25%) People aged 5-24 (16%) Note: Usually 90% of seasonal influenza-related deaths occur in people aged 65 and older
 Next highest people aged (25%) People aged 5-24 (16%) Note: Usually 90% of seasonal influenza-related deaths occur in people aged 65 and older")
17
What we don’t know! Influenza viruses are unpredictable and can change in severity Anticipate CDC guidelines updates as new information becomes available Exact date of vaccine availability (mid-October) 2 doses (anticipated) vs. 1 dose Supply versus demand Amount and types of vaccine combinations we will receive Single filled syringe Multi-dose vials Nasal spray Preservative free
 2 doses (anticipated) vs. 1 dose Supply versus demand Amount and types of vaccine combinations we will receive Single filled syringe Multi-dose vials Nasal spray Preservative free.")
18
Public Health Planning Meeting weekly with PH Emergency Response Team Monitoring State and Federal Guidelines Preparing for delivery of large #s of vaccines Developing agreements for vaccination centers Developing Communications Plan Developing internal policy to require sick employees to stay home Developing Voluntary Medical Reserve Corps Communicating with Health Care Providers and Emergency Responders Seasonal flu vaccines available earlier this year in preparation for H1N1 vaccines

19
Public Health Authorized Intervention Options To help contain or limit the spread of infections as effectively as possible The Health Department has the authority to: Treat sick and exposed individuals with antivirals Isolate sick people in hospitals, homes or other facilities Identify and quarantine exposed people Close schools and workplaces as needed Cancel public events Restrict Travel

20
Funding State and local funding Uncertain Governors Executive Order Both House and Senate version increase funding Governors preliminary budget cuts PH funding by 17% Federal Emergency Preparedness Funding available for planning Federal funding available for vaccines and supplies Uncertain if funding will be available to administer vaccine but assumption is it will be

21
Communications to Schools School Web Portal Frequent fax updates (daily if warranted) Nurse of the Day available to answer questions Presentations Letters Fact Sheets School reporting summaries
 Nurse of the Day available to answer questions Presentations Letters Fact Sheets School reporting summaries")
22
Strategic National Stockpile

23
Antivirals Methods of dispensing Criteria PPE –face masks

24
H1N1 Vaccine Novel H1N1 vaccine is being purchased by the Federal Government Allocation to States in proportion to population States will allocate to LHD for distribution to vaccination partners Timing of availability – earliest in mid-October Vaccines remains the single best means for protection

25
H1N1 Vaccine Priority Groups On 7/29/09, CDC/ACIP recommendations for equal focus due to at risk conditions and burden of disease: 1. Pregnant women 2. People who live with or care for children younger than 6 months age 3. Health care and emergency services personnel 4. Persons between the ages of 6 months – 24 years of age 5. People from ages 25 – 64 years who are at higher risk for H1N1 complications due to chronic health diseases or compromised immune systems

26
Alternate/Closed PODs Agreements School Districts What we need from schools and what you can expect from us (PODs – Points of Distribution)
")
27
Influenza Prevention Strategies Personal hygiene Social Distancing Antivirals drugs Vaccines

28
What Can Schools do to prepare for the Fall Flu Season?

29
Update Communication Networks Identify key contacts/authorities responsible for case identification, isolation, quarantine, movement restriction, healthcare services, emergency care, and mutual aid. Communications and education about influenza and preparation for Staff/ Students/Parents Keep in contact with us-Your Local Health Department

30
Diversify Communication Venues Consider use of social media sites such as ‘Twitter’ and ‘Facebook’ to educate and communicate Specially appealing to school aged children Use of http://twitter.com/cdcemergency increased from 2500 followers before H1N1 to 370,000 and now up to 624,000http://twitter.com/cdcemergency PH/School health portal RSS feed - twitter

31
Review Emergency Plans and Policies Review school emergency plans and update contact information Support a policy that stresses employees and students with flu like illness to stay home Review capacity for distance education Review guidelines and consider policies for exclusion Strongly advise staff and students to get the seasonal flu when available

32
Promote Respiratory Hygiene Allow regular breaks for students and staff to wash hands using soap and water Waterless hand gels sanitizers may be used in the classroom to minimize disruptions Check sink locations and restrooms regularly to ensure they are stocked with soap, paper towels or working hand dryers Cough etiquette education posters throughout school

33
Disinfecting Facilities Viruses commonly live on surfaces from 2-8 hours When schools reopen, Commonly hand touched surfaces such as stairways, railings, elevator buttons should be kept clean by wiping with detergent-based cleaners or EPA registered disinfectants used in the school settings

34
School Mass Vaccination Clinics Schools –potential site for mass vaccination clinics –CDC/DOE (further guidance expected by end of week) School nurses MOU/Agreements with VNA, other nursing associations Need to address spectrum of issues related to school based vaccinations such as: Logistics Communication with parents Consent forms Develop relationships with volunteer organizations to get volunteers to assist with mass vaccination
 School nurses MOU/Agreements with VNA, other nursing associations Need to address spectrum of issues related to school based vaccinations such as: Logistics Communication with parents Consent forms Develop relationships with volunteer organizations to get volunteers to assist with mass vaccination")
35
School Closures CDC/ DOE: New guidelines anticipate not advising school closure unless magnitude of absenteeism interferes with the school function Decisions will be made at the local level and on a case by case basis Schools may need to close depending on the severity of the pandemic Local and state health department will work with schools to make a decision consistent with community health needs. To aid this process: Reporting of respiratory and GI symptoms to local health department and increased rates of absenteeism to local health department Please Call Early & Often!

36
CDC Revised Recommendations for Schools K-12 8/5/09- CDC revises guidelines for the exclusion of persons with influenza-like illness “CDC recommends that people with influenza-like illness remain at home until at least 24 hours after they are free of fever (100 degrees F), or signs of a fever without the use of fever-reducing medications.”
, or signs of a fever without the use of fever-reducing medications.")
37
CDC Recommendations for Schools Isolate those with flu like symptoms promptly in a room separate from other students while waiting to be sent home Do Not administer Aspirin or aspirin-containing products to <18 years age Ill students should not attend alternative child care or congregate in the community

38
CDC Recommendations for Schools School administrator’s should communicate regularly with local public health officials to obtain guidance about reporting of influenza-like illnesses in the school Changes in frequency of IP-10 reporting can be expected Key messages: Keep ill students and staff at home Wash hands frequently Cover cough and sneezes

39
Conclusion Planning and preparing now is important to be ready for the fall flu season Ongoing communications will be essential

40
Public Health Contacts Public Health Communicable Disease Department Office hours: 734 - 544- 6770 After hours: 734 - 891- 4327 Donna Nussdorfer, CD Coordinator 544-6880 Email: nussdorferd@ewashtenaw.orgnussdorferd@ewashtenaw.org Laura Bauman, Epidemiologist 544-6763 Email: baumanl@washtenaw.orgbaumanl@washtenaw.org Diana Torres-Burgos, Medical Director 544-3058 Email: torresburgosd@ewashtenaw.orgtorresburgosd@ewashtenaw.org Richard Fleece, Health Officer 544-2959 Email: fleecer@ewashtenaw.orgfleecer@ewashtenaw.org Cindra James, Emergency Preparedness Coordinator 544- 2979 Email: jamesc@ewashtenaw.orgjamesc@ewashtenaw.org

41
Resources The Centers of Disease Control and Prevention www.flu.gov www.flu.gov www.cdc.gov/h1n1flu/schools/schoolguidance.htm www.cdc.gov/h1n1flu/schools/schoolguidance.htm www.cdc.gov/h1n1flu/schools/toolkit www.cdc.gov/h1n1flu/schools/toolkit The Department of Education www.ed.gov www.ed.gov Michigan Department of Community Health www.michigan.gov/h1n1 www.michigan.gov/h1n1 Washtenaw County Public Health http://publichealth.ewashtenaw.org http://publichealth.ewashtenaw.org Public Health - School Portal

42
Q & A Communications Education of Staff/students/Parents Screening and implementation ill staff/students to stay at home Mass vaccination clinics Best sites, staffing, logistics Private, Charter, Child care centers Schools and Public Health Expectations Challenges Capabilities

Similar presentations





 Information>")










 is a respiratory disease of pigs caused by type A influenza virus that regularly causes outbreaks of influenza in pigs. Swine.>")


 Management Presentation>")