Download presentation
Presentation is loading. Please wait.

1
Peter Emery, MD Specialist in Clinical Hypertension InterMed Portland, ME

2
Epidemiology of Hypertension Hypertension Practice Guidelines Experience of Kaiser Permanente Experience of InterMed

3
58-78 Million American Adults 29-31% of American Adults $69.9 Billion in 2008 ◦ Direct and indirect (CAD, stroke, renal failure) costs 15% of the 2.4 Million Deaths in 2009
 costs 15% of the 2.4 Million Deaths in 2009")
4
Control of hypertension is inadequate 81.5% are aware they have it 74.9% are being treated 52.5% are under control

5
Date of download: 11/12/2014 Copyright © 2014 American Medical Association. All rights reserved. From: US Trends in Prevalence, Awareness, Treatment, and Control of Hypertension, 1988-2008 JAMA. 2010;303(20):2043-2050. doi:10.1001/jama.2010.650 Data are presented as means with 95% confidence intervals (error bars). For all curves, the statistical significance of change over time between 1988-1994 and 2007-2008 was P ≤.04, except for hypertension awareness for individuals aged 18 to 39 years (P =.36) and hypertension prevalence, treated, treated and controlled, and controlled for individuals aged 18 to 39 years (insufficient data to reliably calculate significance using weighted linear regression). Figure Legend:
: doi: /jama Data are presented as means with 95% confidence intervals (error bars). For all curves, the statistical significance of change over time between and was P ≤.04, except for hypertension awareness for individuals aged 18 to 39 years (P =.36) and hypertension prevalence, treated, treated and controlled, and controlled for individuals aged 18 to 39 years (insufficient data to reliably calculate significance using weighted linear regression). Figure Legend:.")
6
Coronary Artery Disease Stroke Renal failure Congestive Heart Failure

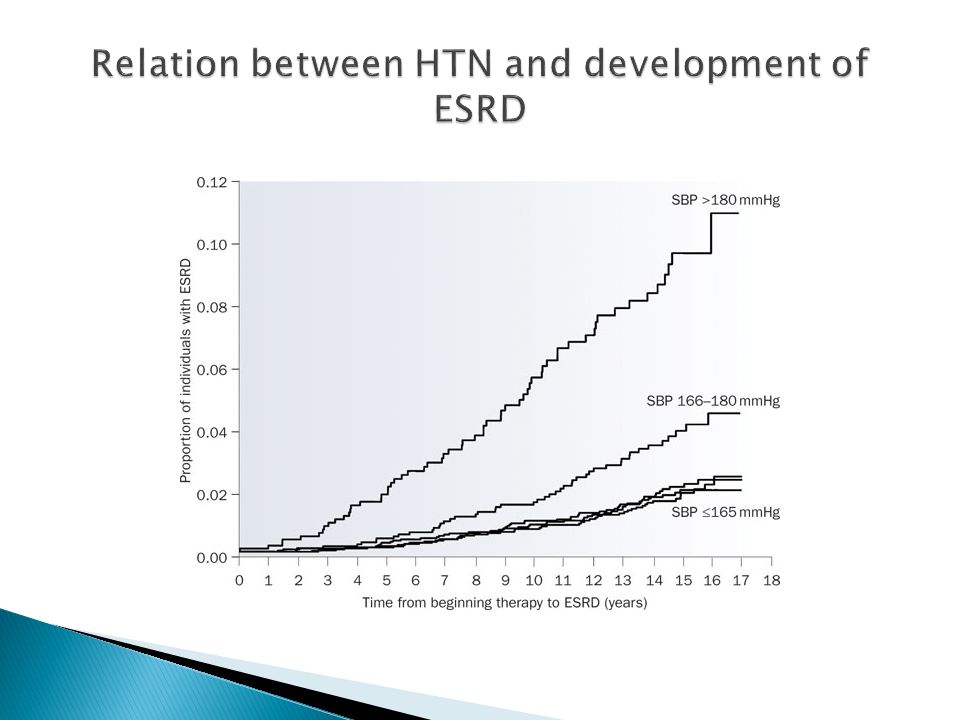
7
Lancet 2002;360:1903

9
JNC 7- 2003 Over the past year ◦ JNC 8 ◦ ASH ◦ AHA/ACC

12
Goal BP of <150 systolic for 60 or older- JNC 8 Staging of hypertension- AHA/ACC, ASH ◦ Stage 1: 140-159/90-99 ◦ Stage 2: >160/100 Initiate therapy with 2 agents Initial Therapy for Black Patients- JNC 8, ASH ◦ Thiazide diuretic or CCB “Compelling Indications”- JNC 8, AHS ◦ JNC 8- CKD ◦ ASH- CKD, DM, CAD, Stroke, CHF Beta blockers not first line therapy- all 3

13
Mixed Messages What are we supposed to do?

15
Poor outcomes- only 50% controlled Multiple guidelines

16
Best evidence: ◦ organized, comprehensive system of regular population review and intervention Cochrane Database Syst Rev. 2010;(3)CD005182
CD")
17
LOWER THE BP AT THE POPULATION LEVEL

19
“High-quality blood pressure management is multifactorial and requires engagement of patients, families, providers, healthcare delivery systems, and communities.” ◦ Science Advisory from AHA/ACC, CDC J Am Coll Cardiol. April 1, 2014, 63(12)
.")
20
Large Managed Care Consortium based in CA ◦ 9.3 Million health plan members

21
HTN control as defined by NCQA HEDIS KP Northern California HTN registry ◦ 652,763 patients in 2009 out of 2.3 million adult patients 2006-2009 ◦ HTN control at KPNC increased from 43.6% to 80.4% ◦ Nationally 55.4% to 64.1% JAMA. 2013;310(7):699-705
:")
22
System-wide hypertension program 5 components ◦ Registry of hypertensive patients ◦ Development and sharing of performance metrics Internal control reports every 1-3 months Successful practices were identified and adopted across the system ◦ Evidence-based guidelines ◦ MA visits for BP measurement every 2-4 weeks NO CHARGE for visit Medications adjusted by primary care provider ◦ Single-pill combination pharmacotherapy Lisinopril-HCTZ; could be used as initial therapy JAMA. 2013;310(7):699-705
:")
23
Continued success 2011 control rate of 87.1%

24
Multispecialty group practice focusing on primary care 75 thousand patients

25
Clinical Microsystems ◦ Front-line units comprised of a small group of people that provide health care Places where patients, families, and care teams meet Including support staff Where recurring patterns of information, behavior, and results take place ◦ Linked processes ◦ Produces performance outcomes ◦ Embedded in larger organizations

26
Team Approach ◦ “Pod” system at InterMed “Working from the ground up” ◦ Structured approach to organizational improvement ◦ “laboratory” for finding and refining successful practices that can be adopted across the organization

27
Practice-wide training in correct BP technique ◦ Aneroid sphygmomanometers Performance Metric ◦ Terminal digit bias Prescription refill protocol ◦ Reducing delays in BP medication refills ◦ Improving staff efficiency 24 hour blood pressure monitor Home BP monitoring

28
Practice-Wide Registry Adopting and modifying an algorithm/practice guidelines NP/PA hypertension experts to see patients in follow up for medication titration Hypertension Specialty Practice ◦ For resistant hypertension and challenging cases

29
Hypertension is prevalent, expensive and a major contributor to cardiovascular mortality There are several practice guidelines and algorithms Population management is the key ◦ Evidence supports organized, comprehensive system of regular population review and intervention to improve the goal of lowering BP We are making strides in this direction at InterMed

Similar presentations














 Minor Research:>")








