Download presentation
Presentation is loading. Please wait.

1
Thyroid Autoimmune Diseases

2
Mechanisms of development of Autoimmune endocrine disease:
Two factors could be involved in development of human autoimmune disorders: Expression of Class II MHC (HLA: human leukocyte antigens) on the surface of the target endocrine cells. The antigen Cross-reactivity
 on the surface of the target endocrine cells. The antigen Cross-reactivity.")
3
Expression of Class II HLA on The Target Cells
Infectious agent (or self-antigen) Inflammatory cells chemotaxis & production of INFγ Expression of HLA genes (MHC class II) Presentation of own cellular proteins Reactive T and B cell response.
 Inflammatory cells chemotaxis & production of INFγ. Expression of HLA genes (MHC class II) Presentation of own cellular proteins. Reactive T and B cell response.")
4
The antigen cross-reactivity:
Infectious agents or external organic material epitopes show antigenic cross- reactivity with self tissues. formation of auto-reactive antibodies. Humoral immune response against self tissues Tissue destruction.

5
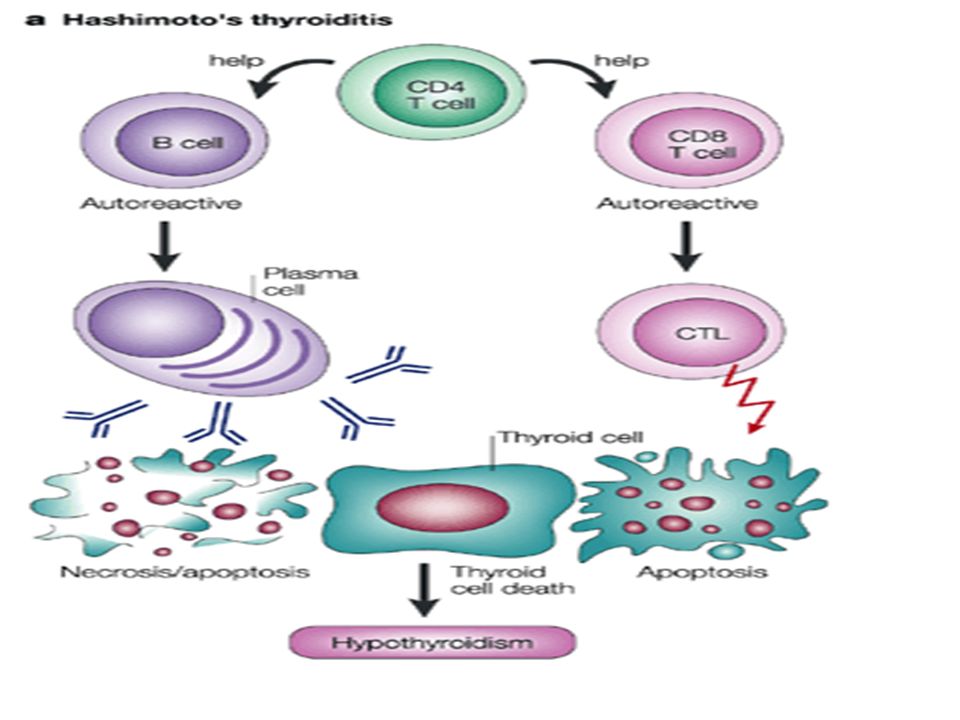
Chronic Lymphocytic Thyroiditis: (Hashimoto’s Thyroiditis):
:")
6
The first disease recognized as autoimmune disease by the Japanese specialist (Hakaru Hashimoto) in Germany in 1912. The thyroid gland is attacked by cell- and antibody-mediated immune processes. Hypothyroidism, large and lobulated thyroid gland due to lymphocytic infiltration and fibrosis.

7
General considerations:
Family history of thyroid disease. HLA gene polymorphism (DR3,DR4, DR5). CTLA-4 *gene polymorphism (cytotoxic T- lymphocyte associated protein) result in reduced negative regulation of T-cells. Most common in middle-aged, starts in adulthood. Woman to men ratio is 5-10: 1. Associated with other autoimmune diseases such as: SLE, dermatitis, and scleroderma. *CTLA-4 is a receptor that transmits an inhibitory signal to T cells.
. CTLA-4 *gene polymorphism (cytotoxic T- lymphocyte associated protein) result in reduced negative regulation of T-cells. Most common in middle-aged, starts in adulthood. Woman to men ratio is 5-10: 1. Associated with other autoimmune diseases such as: SLE, dermatitis, and scleroderma. *CTLA-4 is a receptor that transmits an inhibitory signal to T cells.")
8
Chromosomal disorders: Turner, Klinefelter’s and Down’s Syndrome.
Other risk factors: Chromosomal disorders: Turner, Klinefelter’s and Down’s Syndrome. Tobacco smoking. Immunological features: Lymphocytic infiltration of the thyroid gland Presence of antibodies against thyroid antigens. Cellular sensitization to thyroid antigens. n

9
Pathogenesis of chronic thyroiditis:
Expression of MHC class II-self epitope complex on the thyroid cell surface. Thyroid cell-CD4+ Lymphocyte interaction. Chemotaxis of CTL and macrophages. Loss of T lymphocyte suppressor function due to CTLA gene A mutation: CTL-thyroid cell interaction and killing of target cells by apoptosis. n

10
Engulfment of cellular peptides by macrophages; antigen presentation.
Activation of B lymphocytes and production of anti- thyroid peroxidase and anti-thyroglobulin antibodies ADCC of cuboidal cells lining the thyroid follicles by CD8 and N.K cells.

12
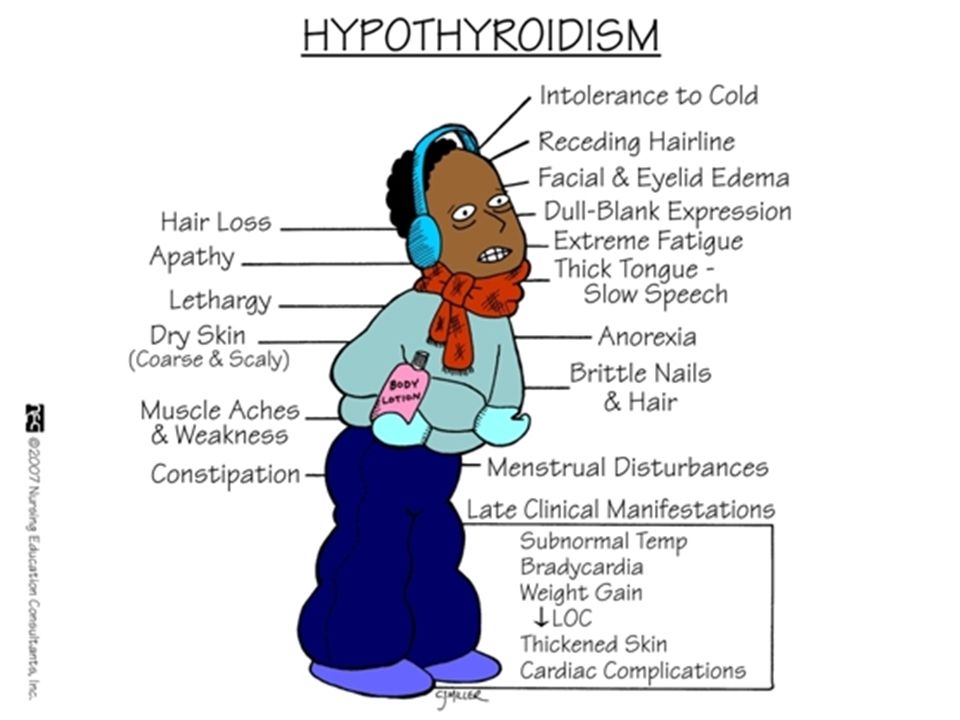
Stages & Clinical Features of Chronic Thyroiditis:
Primary stage: Transient hyperthyroidism due to inflammatory breakdown of thyroid follicles (silent painless inflammation). Release of thyroid hormones. Late stage: Hypothyroidism due to progressive destruction of thyroid tissue and cellular malfunction. The last outcome of Hashimoto’s disease is hypothyroidism.
. Release of thyroid hormones. Late stage: Hypothyroidism due to progressive destruction of thyroid tissue and cellular malfunction. The last outcome of Hashimoto’s disease is hypothyroidism.")
13
A consistent physical sign in Hashimoto’s disease is enlarged thyroid gland (Goiter).
Enlarged surrounding lymph nodes. Weight gain, muscle weakness, cold intolerance, depression, fatigue, constipation, periorbital edema , hoarse voice and dry skin. Rarely, symptoms of urticaria and nephritis can be seen due to presence of circulating immune complexes.

16
Diagnosis of Chronic Thyroiditis:
The disease is diagnosed by the presence of autoantibodies: Anti-thyroglobulin* antibodies. Anti-thyroid peroxidase antibodies. These antibodies can be detected by: Immunofluorescence assay , ELISA or agglutination assay. In seronegative patients, autoantibodies are localized intrathyroidal. Histopathology *Thyroglobulin (Tg) a protein produced by the thyroid and is used to produce the thyroid hormones thyroxine (T4) and triiodothyronine (T3). *Thyroid peroxidase oxidizes iodide to iodine for addition onto tyrosine residues on thyroglobulin for the production of thyroxine (T4) or triiodothyronine (T3),
 a protein produced by the thyroid and is used to produce the thyroid hormones thyroxine (T4) and triiodothyronine (T3). *Thyroid peroxidase oxidizes iodide to iodine for addition onto tyrosine residues on thyroglobulin for the production of thyroxine (T4) or triiodothyronine (T3),")
17
N Immunohistochemistry for P63. Positive in Germinal center (not found in normal glands). Germinal center formation within thyroid tissues: reactive lymphocyte infiltrate. Pink: dying thyroid cell

18
Before After

19
Graves’ Disease:

20
It is an autoimmune disease where the thyroid is activated by anti-TSH receptor autoantibodies to produce excessive amount of thyroid hormones. The most common cause of hyperthyroidism (60-90%), affects up to 2% of the female. 5-10 more common in females than in males. It has a powerful hereditary component
, affects up to 2% of the female more common in females than in males. It has a powerful hereditary component.")
21
General Considerations:
Hyperthyroidism and thyrotoxicosis with a diffuse goiter. About 30-50% of people with Graves' disease will also suffer from Graves' ophthalmopathy caused by inflammation of the eye muscles by attacking autoantibodies. Exophthalmos: upper eyelid retraction, edema, erythema, and conjunctivitis. The volume of the extraocular muscles and retroorbital connective and adipose tissue is increased, due to inflammation . Autoantibodies to various components of retroorbital tissues, particularly components of extraocular muscle cells, have been detected in the serum of patients with Graves' ophthalmopathy.

22
Graves’ Goiter and Exophthalmos

23
Family History: increased risk if other family members are affected.
Specific cross-reactivity between some microbes (viruses; Coxsackieviruses, and bacteria; Yersinia enterocolitica) and TSH- receptors on thyroid follicular cells. Strong association with DR3, DQα , and DQβ genotype of MHC II haplotypes Family History: increased risk if other family members are affected. Associated with different types of autoimmune diseases; such as Hashimoto’s disease and antibodies to gastric intrinsic factors.* * Graves’ disease can lead to Hashimoto’s thyroiditis and vice versa.
 and TSH- receptors on thyroid follicular cells. Strong association with DR3, DQα , and DQβ genotype of MHC II haplotypes. Family History: increased risk if other family members are affected. Associated with different types of autoimmune diseases; such as Hashimoto’s disease and antibodies to gastric intrinsic factors.* * Graves’ disease can lead to Hashimoto’s thyroiditis and vice versa.")
24
Clinical presentation:
Goiter, exophthalmos (30-50%), muscle weakness, weight loss, diarrhea and frequent defecation, hyperactivity, tachycardia, hair loss, and oligomenorrhea. Immunologic features of Graves’ disease: Antibodies against TSH receptor; that stimulate thyroid cell function. Class II HLA expression on the surface of thyroid cells. Associated autoimmune ophthalmopathy. N
, muscle weakness, weight loss, diarrhea and frequent defecation, hyperactivity, tachycardia, hair loss, and oligomenorrhea. Immunologic features of Graves’ disease: Antibodies against TSH receptor; that stimulate thyroid cell function. Class II HLA expression on the surface of thyroid cells. Associated autoimmune ophthalmopathy. N.")
25
Autoantibodies present against TSH- receptor:
Thyroid-stimulating immunoglobulins (TSI): Activate TSH-receptor; increase thyroid hormones levels. Thyroid growth immunoglobulins (TGI): Growth of thyroid follicles. Thyrotrophin binding-inhibiting immunoglobulins (TBII): Inhibits TSH binding. Thyrotrophin = TSH
: Activate TSH-receptor; increase thyroid hormones levels. Thyroid growth immunoglobulins (TGI): Growth of thyroid follicles. Thyrotrophin binding-inhibiting immunoglobulins (TBII): Inhibits TSH binding. Thyrotrophin = TSH.")
26
Colloid suspension show lymphocytic infiltration: CD4, CD8, and B lymphocytes.
No cellular immune response; Histology shows no destruction of thyroid tissues.

27
Pathogenesis mechanism of Graves’ disease:

28
N n

29
Diagnosis of Graves’ disease:
Clinically: Signs and symptoms. Radiologically: Increased uptake of radioactive iodine. Serology: Elevated total and free T4, and T3. Identification of anti-thyroid antibodies in patient’s sera: Thyroid stimulating Immunoglobulin (TSI). Thyroid growth stimulating immunoglobulins Thyroid binding-inhibiting immunoglobulins
. Thyroid growth stimulating immunoglobulins. Thyroid binding-inhibiting immunoglobulins.")
30
Anti-thyroid antibodies can be detected by: ELISA Test:
Microtiter plate wells should be coated by recombinant human TSH-receptors. Tissue culture(Fisher Rat thyroid cell line) measure the presence and activity of anti- thyroid antibodies (IgG) in patient's sera. Serum specimens are incubated with rat thyroid cell line culture; then the incorporation of radioactive thymidine (pyrimidine) are measured. (action of TGI) N
 measure the presence and activity of anti- thyroid antibodies (IgG) in patient s sera. Serum specimens are incubated with rat thyroid cell line culture; then the incorporation of radioactive thymidine (pyrimidine) are measured. (action of TGI) N.")
32
THANKS

Similar presentations

 Hypersensitivity. (cytotoxic hypersensitivity )>")










BB>")



. Inflammation and destruction.>")


: (IDDM-type 1)>")
