Download presentation
Presentation is loading. Please wait.

1
The course and conduct of normal labor and delivery Song Weiwei OB&GY Department of Shengjing Hospital

2
Definition of labor Labor is strictly defined as regular uterine contractions with resultant change of cervical effacement and dilatation and extrusion of the products conception.

3
Types of delivery Postterm delivery:>42w
Premature delivery:28w~36w+6 Term delivery:37~41w+6 Postterm delivery:>42w

4
Why and when the labor initiated?
Mechanical theory Endocrine regulating theory Neurohumone theory No exact course has been found that can initiate the onset of labor.

5
Four factors that determine a normal labor
expulsive force birth canal fetal factors psychological factors (3 Ps: powers, passage and passenger)
")
6
Expulsive force Characteristics of uterine contraction rhythmicity
symmetry polarity retraction

7
rhythmicity symmetry polarity retraction

8
Birth canal (passage) bone canal
pelvis: size \shape\ inclination of pelvis soft canal vagina、cervix、low segment of uterine cervical effacement :2~3cm before labor cervical dilatation: closed to 10cm open

9
Fetus Lie- relationship between the long axis of the fetus and that of the mother (longitudinal, transverse or oblique). Presentation- the fetal part that lies closest to the pelvic inlet (cephalic - vertex, face; breech; shoulder). Position- relationship of the fetal parts to maternal parts.
. Position- relationship of the fetal parts to maternal parts.")
10
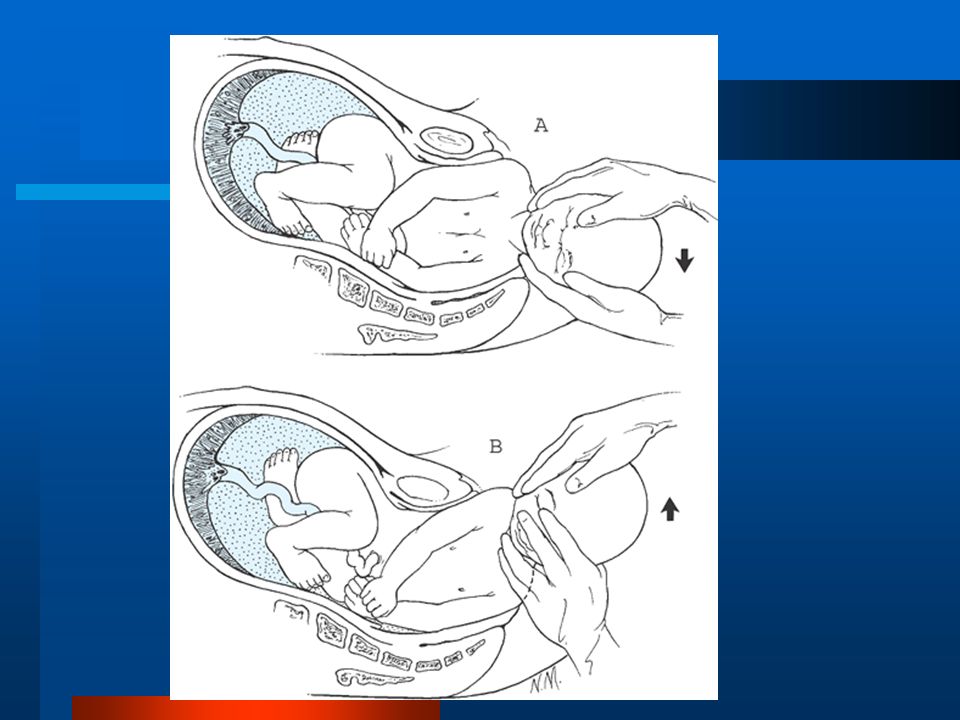
incomplete breech presentation frank breech presentation complete breech presentation

14
Fetus Body weight of fetus Diameters of fetal skull BPD:9.3cm
Occipito frontal diameter: 11.3cm Occipito bregmatic diameter:9.5cm Occipito mental diameter:12.5cm Fetal position Fetal anomality: hydrocephalus, conjoined twins.

15
What signs might the patient report to herald the onset of true labor?
Bloody show: the release from the cervix of the protective mucous plug intermixed with a small amount of blood as a result of cervical effacement. Regular contractions: contractions occurring at regular intervals (such as every five minute) suggest true labor. The contractions are felt in the lower abdomen and back, and are noted to increase in intensity over time. Rupture of membranes (ROM) : a gush of clear fluid (break your water) is felt coming from the vagina. The fluid may otherwise leak slowly but steadily out of the vagina.
 suggest true labor. The contractions are felt in the lower abdomen and back, and are noted to increase in intensity over time. Rupture of membranes (ROM) : a gush of clear fluid (break your water) is felt coming from the vagina. The fluid may otherwise leak slowly but steadily out of the vagina.")
16
What is a Bishop score? -----evaluate the condition of cervix
This system is used to grade the cervix in terms of readiness for delivery. Each factor is given a score of 0 to 3. the factors graded are dilation, effacement, station, consistency and position. Station refers to the level of descent of the presenting part (usually the head) of the fetus. The preferred method is in relationship to the ischial spines. Above the spines one uses -5 to -1 cm (-5 being most superior). Zero station is at the level of the ischial spines. Similarly, +1 to +5 cm describes the presenting part below the level of the ischial spines (+5 being at the introitus). A cervix that is ready (ripe) for delivery is considered favorable. A score of 5 or greater strongly suggests an advancing cervix.
 of the fetus. The preferred method is in relationship to the ischial spines. Above the spines one uses -5 to -1 cm (-5 being most superior). Zero station is at the level of the ischial spines. Similarly, +1 to +5 cm describes the presenting part below the level of the ischial spines (+5 being at the introitus). A cervix that is ready (ripe) for delivery is considered favorable. A score of 5 or greater strongly suggests an advancing cervix.")
17
What are the stages of labor?
Stage 1: onset of labor ~ full dilation of the cervix. latent phase: in which early cervical effacement and dilation occur:0~3cm. active phase: cervical dilation becomes more rapid (approximately 3 to 4 cm to full dilation of 10cm). Stage 2 : complete cervical dilation~ delivery of the infant. Stage 3: after delivery of the infant ~ delivery of the placenta.
. Stage 2 : complete cervical dilation~ delivery of the infant. Stage 3: after delivery of the infant ~ delivery of the placenta.")
18
Duration of the labor

19
Mechanisms of labor The special labor mechanisms is due to asymmetry of the shape of both the fetal head and maternal pelvis. Changes in the position of the fetal head are required for the average size fetus to accomplish passage through the birth canal. The rotations are accomplished by the propulsive force of uterine activity.

20
Cardinal movements of labor
movements of the head engagement descent 1. flexion 2. internal rotation 3. extension 4. external rotation expulsion

21
Engagement It is the descent of the largest transverse diameter of fetal head (BPD) to a level below the plane of the pelvic inlet. Then the head is engaged.

22
Flexion (I movement of the head) - placement of the fetal chin on the thorax (fetus takes a chin-to-chest posture) Internal rotation (II movement) - the occiput rotates toward the mother’s pubic symphysis.
 - the occiput rotates toward the mother’s pubic symphysis.")
23
Extension - III movement
Begins at the level of maternal vulva The fetal head is delivered by extension from the flexed to the extended position rotating around the symphysis pubis ( the occiput arches toward the fetal back).
.")
25
External rotation - IV movement
After delivery of the head the forces exerted on the head by the maternal pelvic musculature are relived and the fetus resumes its normal face-forward position. Its face begins to „look” at one of mother’s leg.

27
Expulsion Delivery of the shoulders - first the anterior one (under the symphysis pubis) and then the posterior one. The rest of the body is usually quickly delivered.

30
How are uterine contractions monitored?
Uterine contractions may be monitored by an internal or external pressure monitor (tocometer). Internal monitoring with an intrauterine pressure catheter (IUPC) confirms the adequacy of contractions. The unit of measure for the IUCP is called the Montevideo unit. Uterine contraction can also be evaluated by the palpation of abdomen.
. Internal monitoring with an intrauterine pressure catheter (IUPC) confirms the adequacy of contractions. The unit of measure for the IUCP is called the Montevideo unit. Uterine contraction can also be evaluated by the palpation of abdomen.")
31
How is fetal heart rate monitored?
Intermittent Doppler ultrasound or (rarely) fetal stethoscope Continuous electronic monitoring via an external monitor or internally via a fetal scalp electrode
 fetal stethoscope. Continuous electronic monitoring via an external monitor or internally via a fetal scalp electrode.")
32
What are the types of episiotomy and their indication?
Sometimes episiotomy is considered necessary to facilitate delivery of the fetus or to avoid a spontaneous tear or tears during a forceps delivery. It is an incision in either the midline or in the mediolateral position of the perineum.

33
Episiotomy A lateral incision of perineum before delivery of the head
Why? to enlarge the area of the outlet easier delivery of the head prevention of intraventricular hemorrhage prevention of lacerations prevention of late complications - relaxation of pelvic muscles and urine incontinence

34
Episiotomy Prophylactic - nulliparas, some multiparas Mandatory
in instrumental delivery, like forceps or vacuum extractor in abnormal presentations, like breech in preterm deliveries

35
Median episiotomy

37
How is pain controlled? The most common form of pain control by far is the epidural. This allows a woman to receive analgesia while maintaining enough sensation to push during the delivery. Alternatively, narcotic analgesics are sometimes used. Spinal anesthetics are sometimes used, delivered into the same area as an epidural but in a single dose. Local blocks, such as a pudendal block, may be given for perineal anesthesia. A local is also given before repair of a tear or episiotomy.

38
What is VBAC? VBAC stands for vaginal birth after cesarean. This is a trial of labor for a patient who has previously undergone a C-section with a low transverse uterine incision. The patient should have had no more than two prior sections, an adequate pelvis, and no history of other uterine incision or rupture. VBAC is contraindicated in patients who have had a prior classical cesarean section due to the increased risk of uterine rupture.

Similar presentations




















. Labor Labor is the energy and effort used to push the baby out of the womb. Dilation is when the cervix.>")





