Download presentation
Presentation is loading. Please wait.

1
MISS Journal Club 2012 Metabolic Surgery & Emerging Technologies Goal: To review 5 important and clinically relevant papers from 2011, on Metabolic Surgery and Emerging Technologies

2
Disclosure

3
10/2/2015 Ann of Surg, 248, 5, Nov 08 3 JAMA. 2012 Jan 4;307(1):56-65. Article #1
: Article #1")
4
Objective To study the association between bariatric surgery, weight loss, and cardiovascular events F/U data from The Swedish Obese Subjects (SOS) Study – an ongoing, non-randomized, prospective, controlled study
 Study – an ongoing, non-randomized, prospective, controlled study")
5
Methods 25 public surgical departments & 480 primary health care centers in Sweden Patient recruitment between 9/1/1987 - 1/31/2001 Median follow-up of 14.7 years (range, 0-20 years). Inclusion criteria – Age 37 to 60 years – BMI of 34 or greater in men – BMI of 38 or greater in women.

6
Methods: cont. N=4047 obese individuals – 2 study arms 1.Obese pts undergoing Bariatric Surgery (n=2010) 2.Obese pts receiving non-operative care (n=2037) Surgery pts (n=2010) underwent: – Gastric bypass (13.2%) – Gastric banding (18.7%), or – Vertical banded gastroplasty (68.1%) Controls (n=2037): – Received usual care in the Swedish primary health care system
 2.Obese pts receiving non-operative care (n=2037) Surgery pts (n=2010) underwent: – Gastric bypass (13.2%) – Gastric banding (18.7%), or – Vertical banded gastroplasty (68.1%) Controls (n=2037): – Received usual care in the Swedish primary health care system.")
8
Methods: cont. Primary Outcome Measure: – Total mortality (Primary end point of the SOS study) – Previously reported in 2007 Secondary Outcome Measure: – MI and stroke were predefined secondary end points – Considered separately and combined
 – Previously reported in 2007 Secondary Outcome Measure: – MI and stroke were predefined secondary end points – Considered separately and combined.")
9
Methods: cont. Data collection, via physical examinations and questionnaires, completed at: – Matching – Baseline – After 0.5. 1, 2, 3, 4, 6, 8, 10, 15 and 20 yrs

10
Findings

11
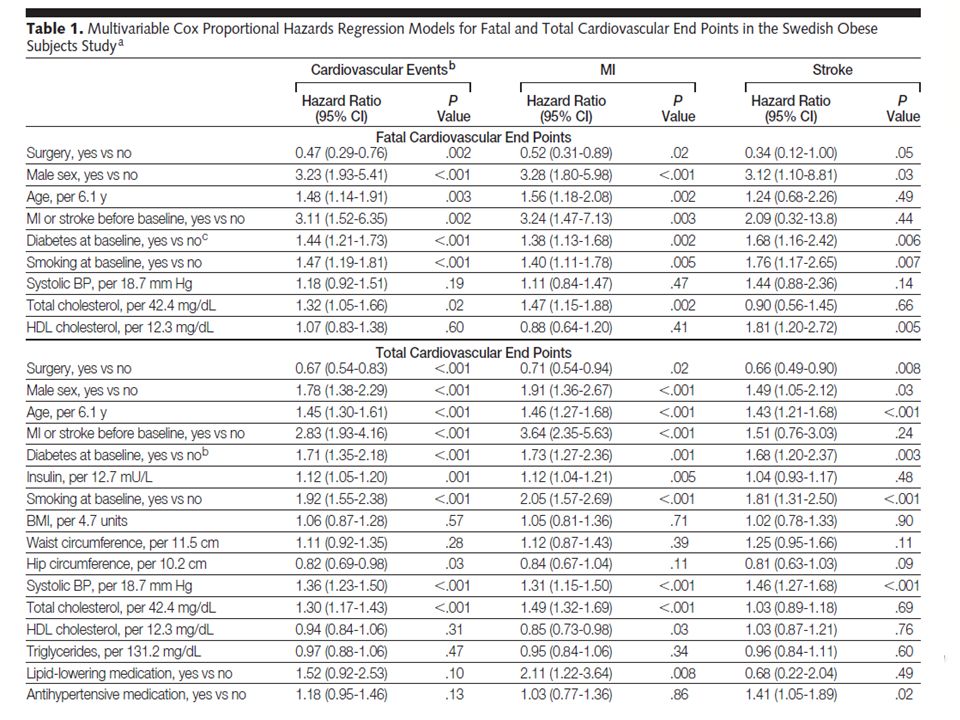
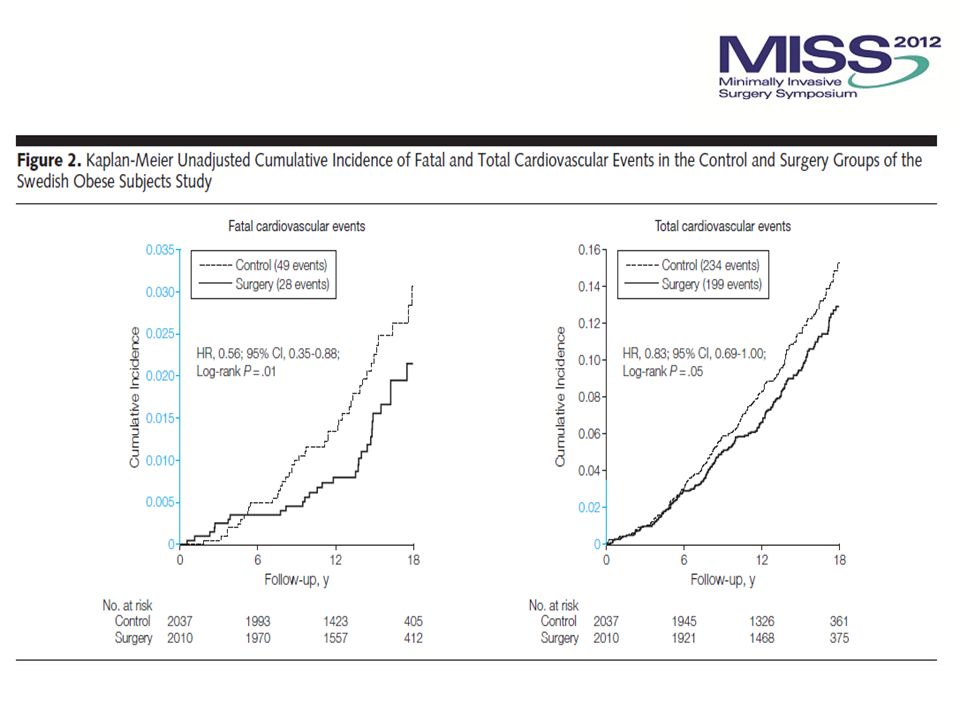
Primary Outcome Measure Bariatric surgery was associated with a reduced number of cardiovascular deaths – 28 events / 2010 pts in the surgery group vs. – 49 events / 2037 pts in the control group – Adjusted hazard ratio [HR] 0.47; 95% CI 0.29-0.76; p=0.002

13
Findings Secondary Outcome Measure Total # of first time cardiovascular events (fatal or nonfatal / MI or stroke) was lower in the surgery group than in the control group – 199 events / 2010 surgery patients vs. – 234 events / 2037 control patients – Adjusted HR 0.67; 95% CI 0.54-0.83; p=0.001

15
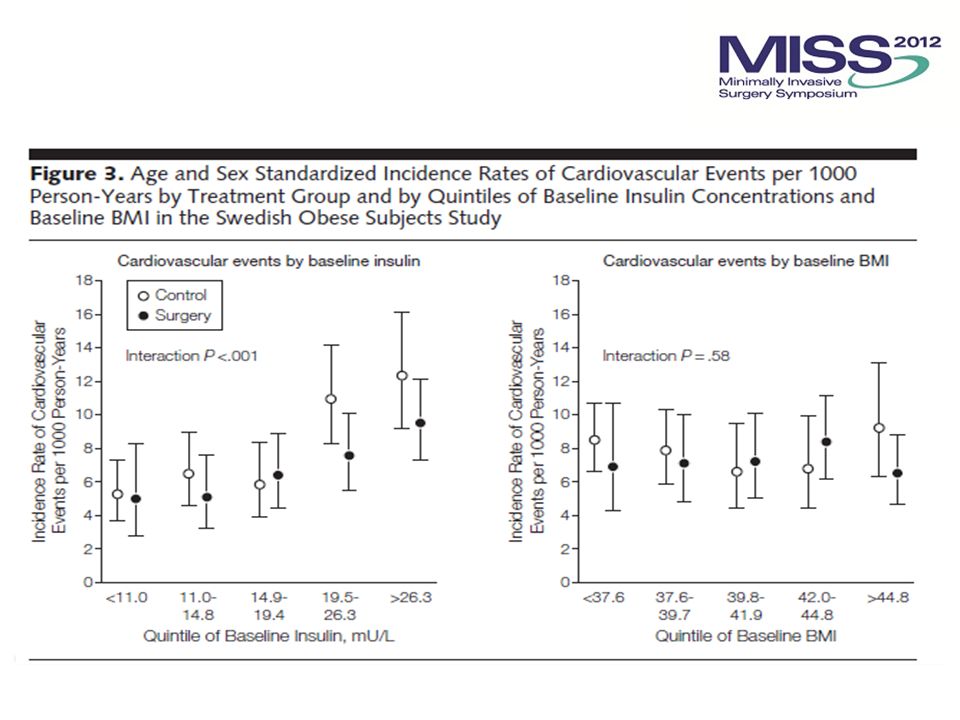
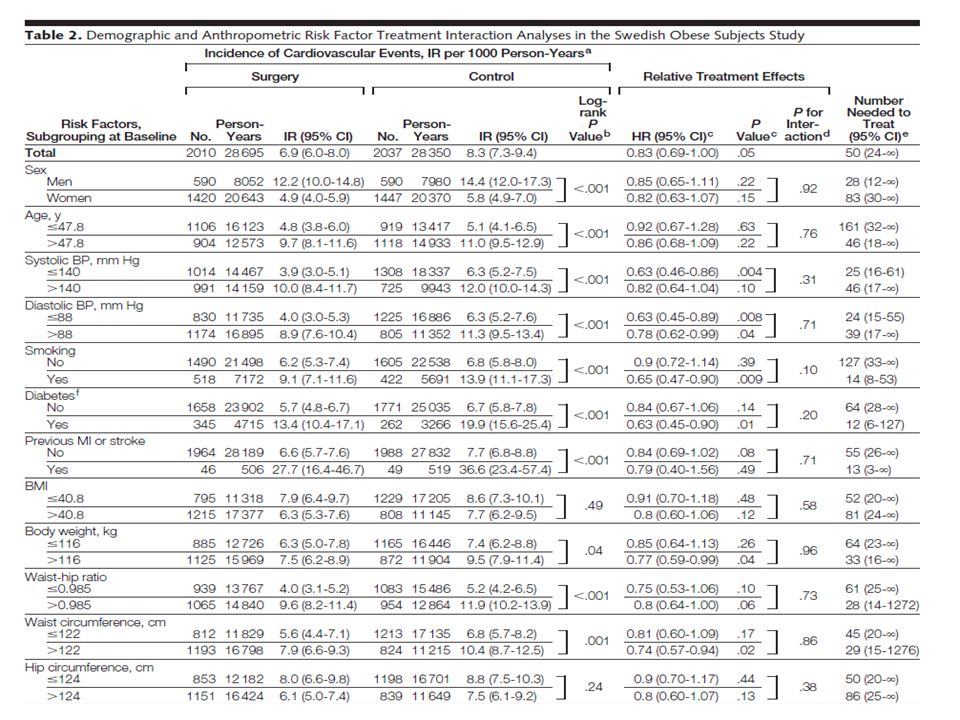
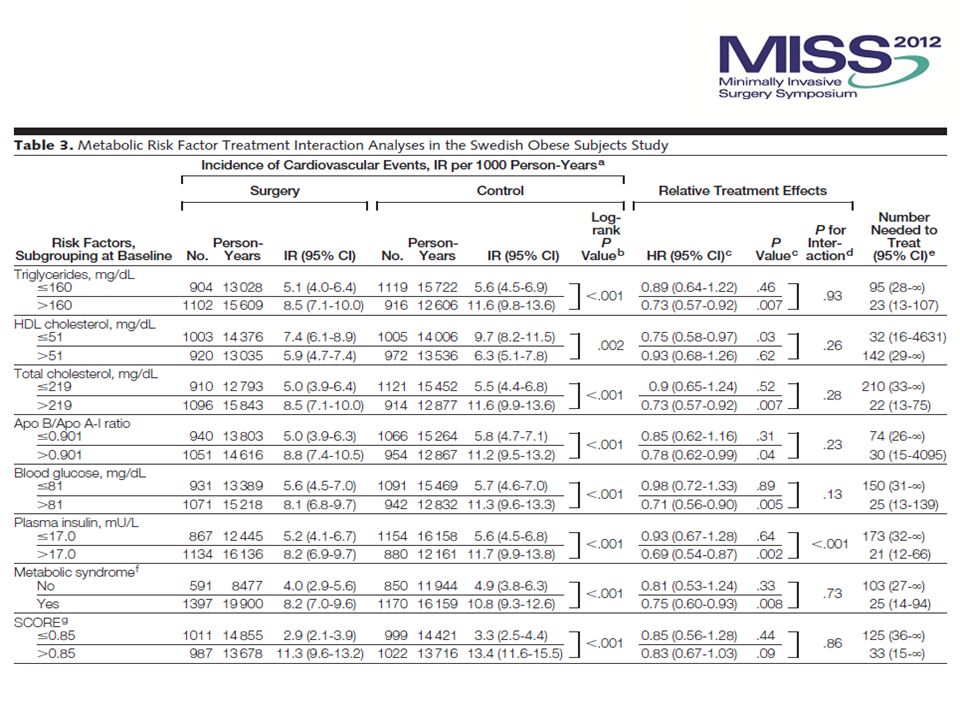
Findings Secondary Subgroup Analysis Post-hoc analysis – Higher baseline insulin concentration was significantly associated with a more favorable outcome of bariatric surgery on cardiovascular events (P for interaction <0.001)
")
18
Discussion

19
Article #2 Br J Surg 2012;99(1):100-3
:100-3")
20
Background Previously, the accepted definition of remission of type II diabetes was: – being off diabetes medication, with normal fasting blood glucose level or HbA1c <6%

21
Background 2009 - American Diabetes Association defined remission of type II diabetes as: “a return to normal measures of glucose metabolism (HbA1c < 6 %, fasting glucose < 5·6 mmol/l) at least 1 year after bariatric surgery without hypoglycaemic medication”
 at least 1 year after bariatric surgery without hypoglycaemic medication")
22
Objective To study the proportion of patients achieving complete remission of type II diabetes following bariatric surgery, according to 2009 ADA consensus definitions

23
Methods Retrospective review of data collected prospectively in three bariatric centres on patients undergoing gastric bypass, sleeve gastrectomy and gastric banding 2 centers in the UK and 1 in Norway

24
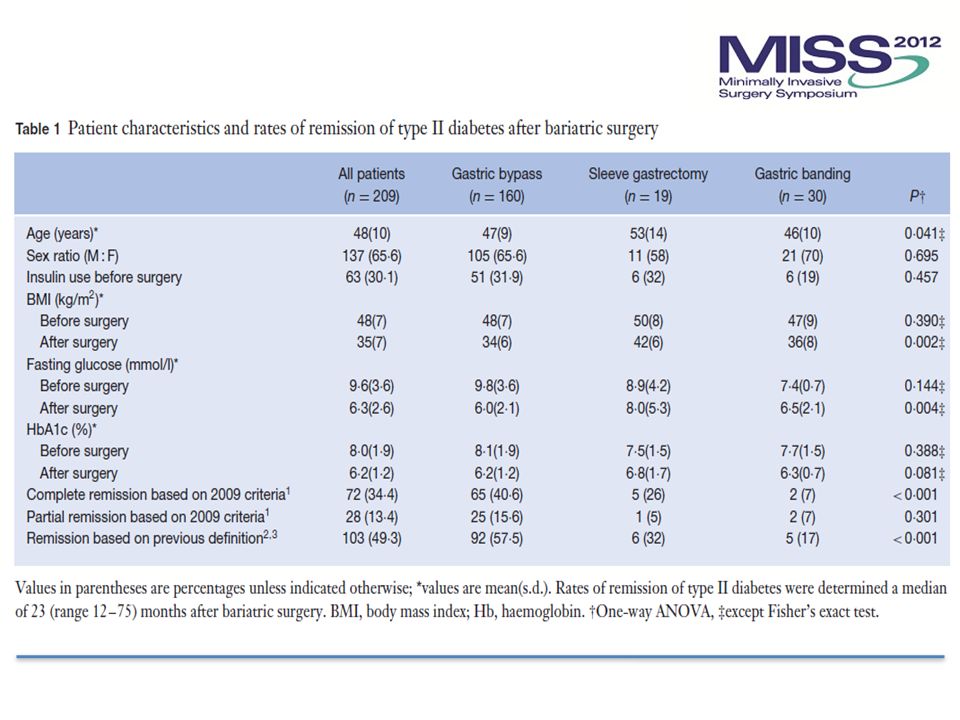
Findings 1006 patients underwent bariatric surgery 209 had type II diabetes Median follow-up: 23 months (range 12–75) HbA1c was reduced after operation in all three surgical groups (p < 0·001) – Gastric bypass – Sleeve Gastrectomy – Gastric Banding
 HbA1c was reduced after operation in all three surgical groups (p < 0·001) – Gastric bypass – Sleeve Gastrectomy – Gastric Banding")
25
Findings 72 of 209 (34·4 %) pts had complete remission of diabetes, according to the new definition Remission rates by procedure were: – 40·6 % (65 of 160) after gastric bypass – 26 % (5 of 19) after sleeve gastrectomy – 7 % (2 of 30) after gastric banding P < 0·001 between groups
 pts had complete remission of diabetes, according to the new definition Remission rates by procedure were: – 40·6 % (65 of 160) after gastric bypass – 26 % (5 of 19) after sleeve gastrectomy – 7 % (2 of 30) after gastric banding P < 0·001 between groups")
27
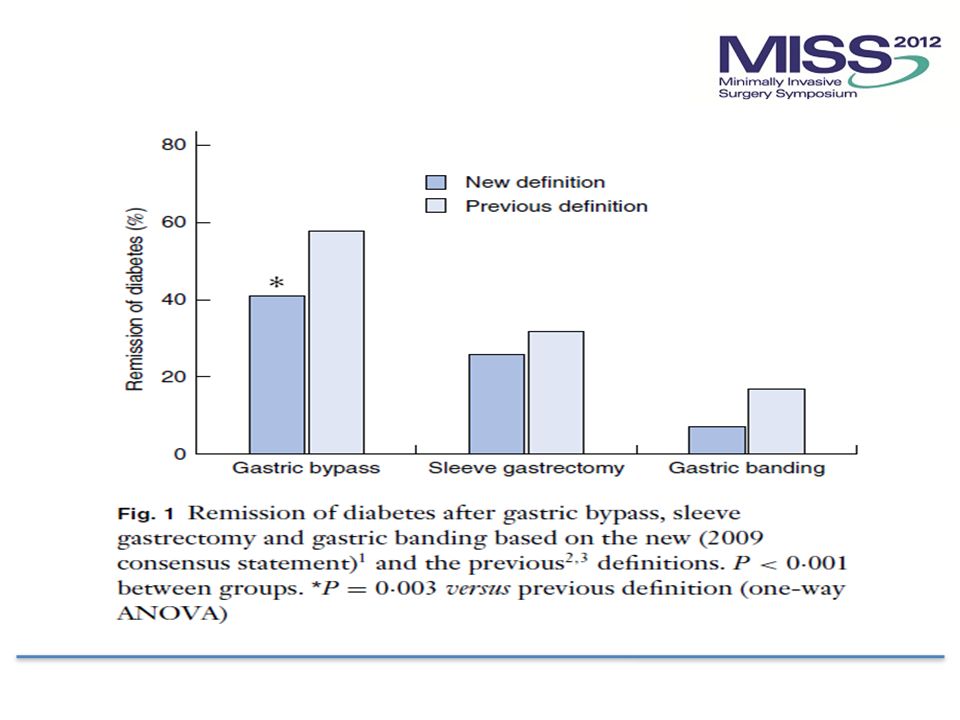
Findings Analysis by procedure showed no significant difference between remission rates based on new and previous definitions for either sleeve gastrectomy or gastric banding

28
Findings Remission rate for gastric bypass was significantly lower with the new definition – 40·6% vs. 57·5 %, p=0·003 Remission rates by procedure were: – 40·6 % (65 of 160) after gastric bypass – 26 % (5 of 19) after sleeve gastrectomy – 7 % (2 of 30) after gastric banding P < 0·001 between groups
 after gastric bypass – 26 % (5 of 19) after sleeve gastrectomy – 7 % (2 of 30) after gastric banding P < 0·001 between groups.")
30
Discussion

31
10/2/2015 Ann of Surg, 248, 5, Nov 08 31 Article #3 Am J Cardiol. 2011;108(10):1499-507
:")
32
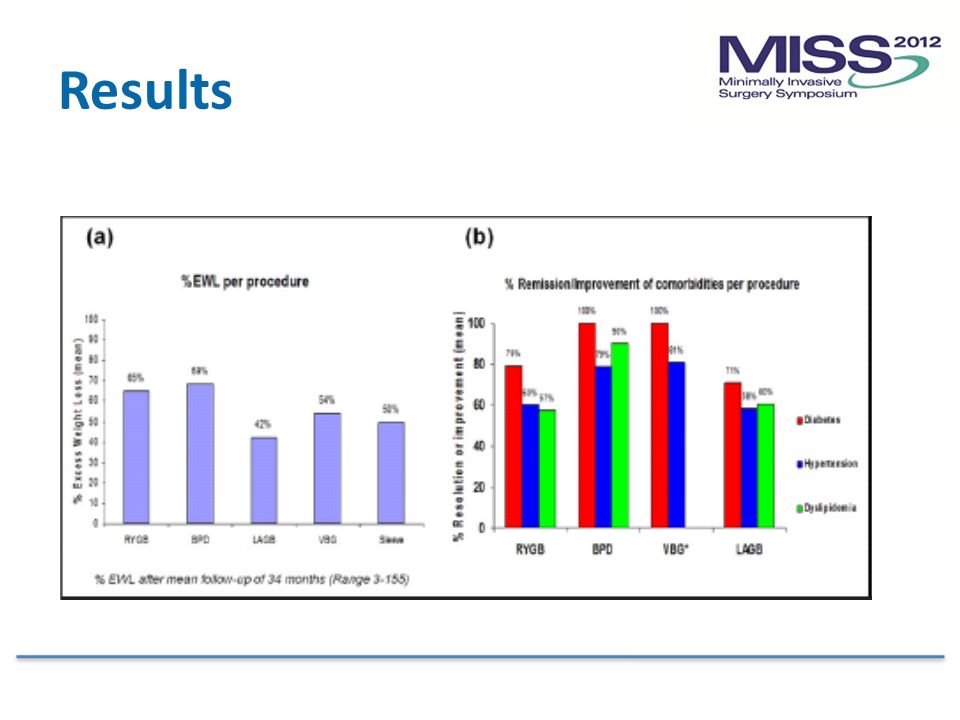
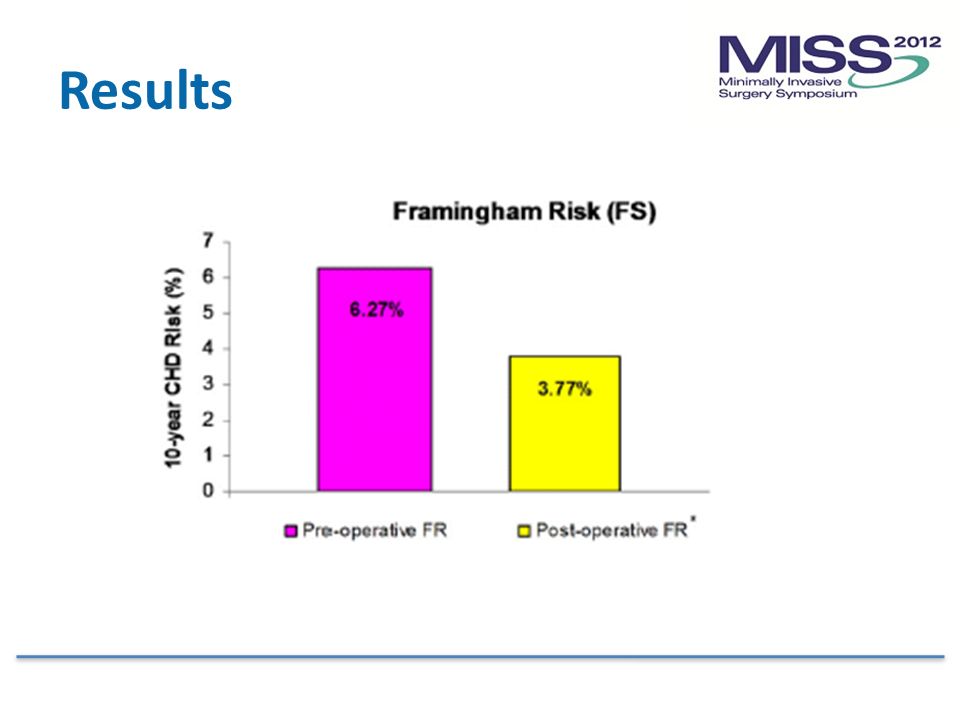
Objective Significant weight loss following bariatric surgery is associated with dramatic benefits including reduced cardiovascular (CV) mortality CV mortality reduction is related to the remarkable consequences on individual co-morbid conditions including diabetes, hypertension and dyslipidemia The purpose of this study was to evaluate the current evidence regarding CV disease risk reduction
 mortality CV mortality reduction is related to the remarkable consequences on individual co-morbid conditions including diabetes, hypertension and dyslipidemia The purpose of this study was to evaluate the current evidence regarding CV disease risk reduction")
33
Methods

34
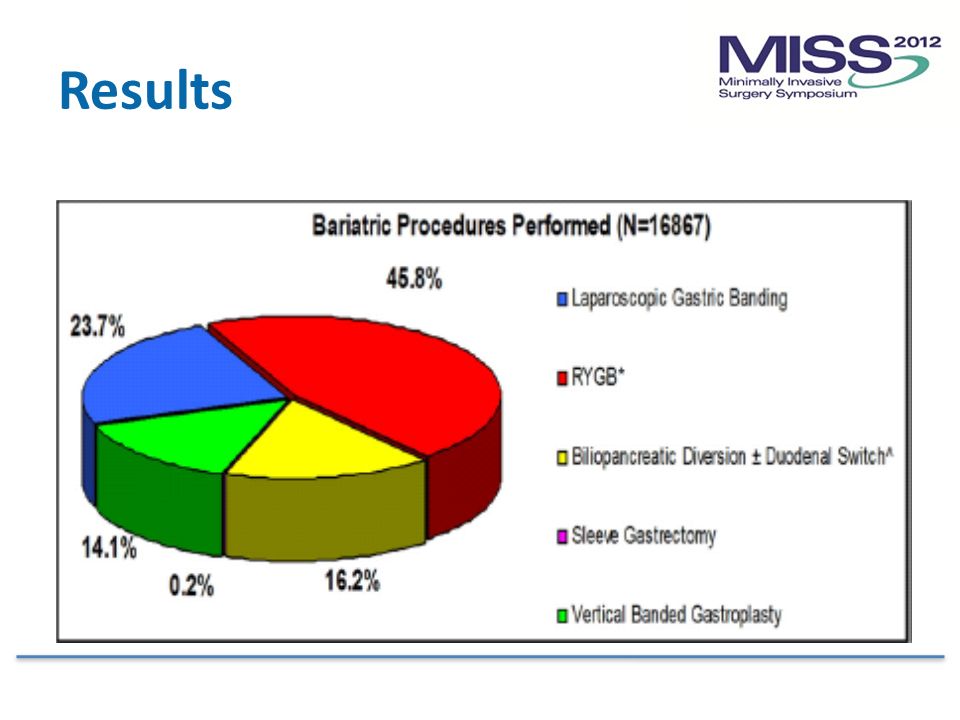
Results

38
Discussion

39
10/2/2015 Ann of Surg, 248, 5, Nov 08 39 Article #4

40
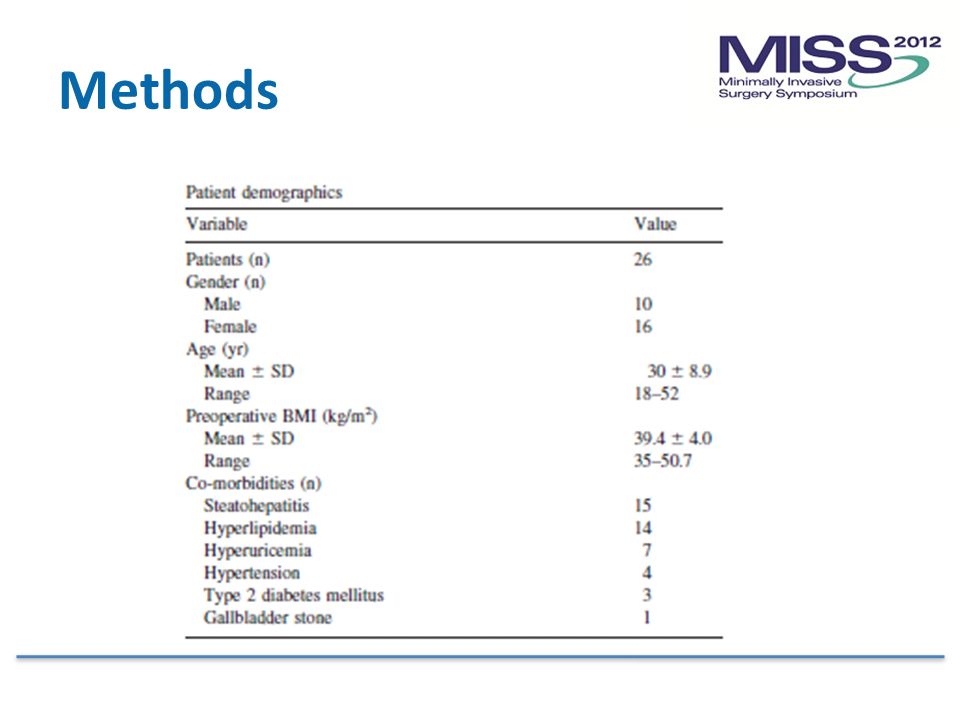
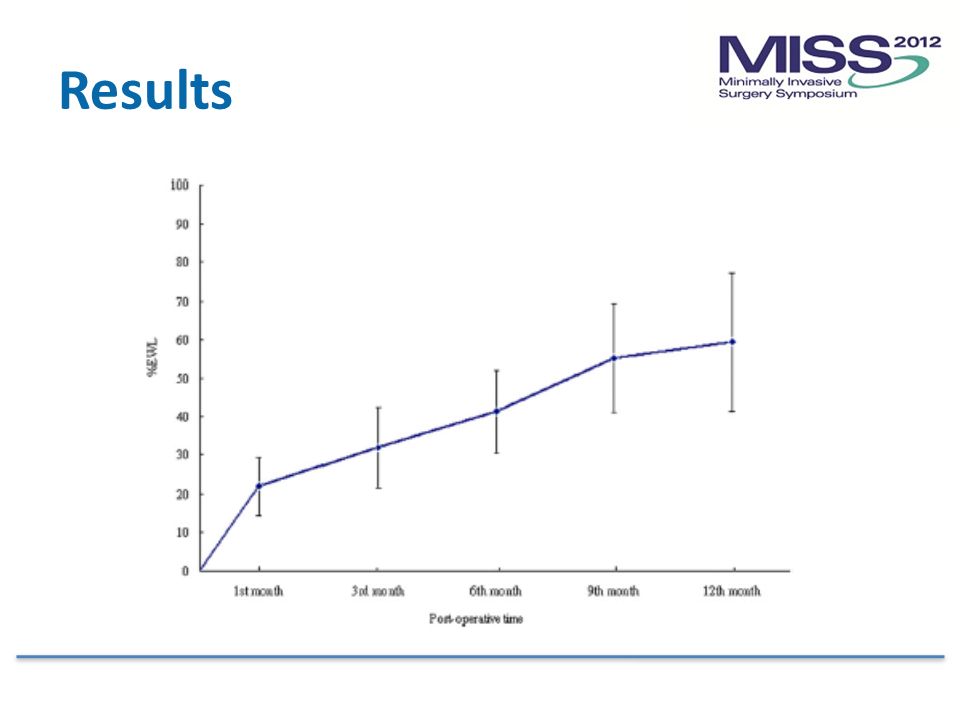
Objective LAGB is considered the safest bariatric procedure Variations in outcomes and complications related to port adjustment The purpose of this study is to report the safety, feasibility and results of LAGB Plication

41
Methods 26 morbidly obese patients Swedish band, pars flaccida technique, 2 anterior gastro-gastric sutures, plication over a 36F bougie F/U @ 1 week, 1,3,6,9,12,18,24 months Gastrograffin study @ 3 months

42
Methods

44
Results

46
Discussion

47
Article #5 World J Surg 2011;35:637-642

48
Objective The daVinci Robot has been implemented in several laparoscopic procedures including Roux-en-Y gastric bypass (RYGBP) with reported advantages including ergonomics Routine use in bariatric surgery has not been adopted due to increases in costs, operating time, and lack of any clear outcomes benefit Objective: Compare intraoperative and postoperative outcomes of 135 consecutive RYGBP operations performed by a single surgeon – 45 laparoscopic RYGB – 90 robotic RYGB
 with reported advantages including ergonomics Routine use in bariatric surgery has not been adopted due to increases in costs, operating time, and lack of any clear outcomes benefit Objective: Compare intraoperative and postoperative outcomes of 135 consecutive RYGBP operations performed by a single surgeon – 45 laparoscopic RYGB – 90 robotic RYGB")
49
Methods Retrospective review of prospectively collected data on N=135 obese individuals All operations performed by a single surgeon Laparoscopic RYGBP (L-RYGBP) cohort, N=35 – underwent standard L-RYGBP with creation of a linear gastrojejunostomy and two layer (vicryl & silk) closure Robotic RYGBP (R-RYGBP) cohort, N=90 – underwent robotic creation of linear gastrojejunostomy with two layer (PDS & PDS) closure
 cohort, N=35 – underwent standard L-RYGBP with creation of a linear gastrojejunostomy and two layer (vicryl & silk) closure Robotic RYGBP (R-RYGBP) cohort, N=90 – underwent robotic creation of linear gastrojejunostomy with two layer (PDS & PDS) closure")
50
Methods: cont. Data collected on demographics, operative time, morbidity, mortality, and 1 year weight loss Operative time calculated as follows – L-RYGBP: time between pneumoperitoneum and closure of skin incisions – R-RYGBP: time recorded in 3 phases 1.Laparoscopic phase (pneumoperitoneum to jejunojejunostomy) 2.Set up phase (docking of the robot and attaching of the arms) 3.Robotic phase (gastrojejunostomy to skin closure)
 2.Set up phase (docking of the robot and attaching of the arms) 3.Robotic phase (gastrojejunostomy to skin closure).")
51
Findings

52
Statistically younger patient cohort in R-RYGBP group – 38 ± 9 years vs. 43 ± 8 years; p = 0.001 Shorter mean operative time in R-RYGBP group – 207 ± 31 min vs. 227 ± 31 min; p = 0.0006 – R-RYGBP gastrojejunostomy time of 57 ± 16 minutes and mean robot set-up time of 31 ± 4 minutes – First 45 R-RYGBP cases were shorter (205 ± 31 minutes; p = 0.0011)
.")
53
Findings No mortalities in either group Early morbidity of 1 patient in each group – Leak from excluded stomach in L-RYGBP group – Pulmonary embolism in one patient from R-RYGBP group Late morbidity higher in L-RYGBP group (4 vs. 1; p = 0.04)
.")
54
Discussion

Similar presentations

>")

















