Download presentation
Presentation is loading. Please wait.

1
Dr. Chris Cobourn Medical Director and Surgeon Surgical Weight Loss Centre Staff Surgeon Trillium Health Centre Mississauga, Ontario

2
Consultant – Allergan Canada

3
There are an overwhelming number of patients with Type II DM No single operation has been proven to be the best for all patients or we would be doing it “My operation versus your operation” is not an effective means of winning the support of endocrinologists All of these operations were designed as bariatric procedures to treat obesity Caution is indicated if we are going to extend the indications and propose treatment for T2DM

4
Guidelines regarding the role of bariatric surgery for diabetes NONE

5
ADA Guidelines 2009: Bariatric Surgery ● Bariatric surgery should be considered for adults with BMI > 35 kg/m2 and type 2 diabetes, especially if the diabetes is difficult to control with lifestyle and pharmacologic therapy. (B) Although small trials have shown glycemic benefit of bariatric surgery in patients with type 2 diabetes and BMI of 30– 35kg/m2, there is currently insufficient evidence to generally recommend surgery in patients with BMI < 35 kg/m2 outside of a research protocol. (E) ● The long-term benefits, cost effectiveness, and risks of bariatric surgery in individuals with type 2 diabetes should be studied in well-designed randomized controlled trials with optimal medical and lifestyle therapy as the comparator. (E) DIABETES CARE, VOLUME 32, SUPPLEMENT 1, JANUARY 2009
 Although small trials have shown glycemic benefit of bariatric surgery in patients with type 2 diabetes and BMI of 30– 35kg/m2, there is currently insufficient evidence to generally recommend surgery in patients with BMI < 35 kg/m2 outside of a research protocol. (E) ● The long-term benefits, cost effectiveness, and risks of bariatric surgery in individuals with type 2 diabetes should be studied in well-designed randomized controlled trials with optimal medical and lifestyle therapy as the comparator. (E) DIABETES CARE, VOLUME 32, SUPPLEMENT 1, JANUARY")
6
L APAROSCOPIC A DJUSTABLE G ASTRIC B AND S URGERY (LAP-BAND) Most common bariatric procedure in Europe, Australia, Canada, Safest Bariatric Procedure - Mortality 1:5000 No functional or structural alteration of the GI tract Adjustable Reversible Purely restrictive (satiety inducing), no malabsorption
 Most common bariatric procedure in Europe, Australia, Canada, Safest Bariatric Procedure - Mortality 1:5000 No functional or structural alteration of the GI tract Adjustable Reversible Purely restrictive (satiety inducing), no malabsorption")
7
B AND A DJUSTMENTS

8
8 Source: O’Brien et al. Obesity is a Surgical Disease: Overview of Obesity and Bariatric Surgery, ANZ J Surg, 2004; 74: 200-204.

11
Weight loss is more gradual than other bariatric procedures Safest bariatric procedure Sustained weight loss Adjustable Commitment and Long Term Follow Up are critical to success Patient and Physician both must be committed Studies from low volume centres with short follow up are not relevant

14
50 patients, Avg BMI 48 1 year EWL 38% Results: HbA1c, Fasting plasma glucose, Fasting insulin, hypoglycemic medications or insulin Remission 64% (32 pts) Improved 26% (13 pts) Unchanged 10% (5 pts) 3 (6%) has HbA1c > 7% Dixon et al. Diabetes Care. 2002;25:358-363.

15
Diabetic pts wt loss is not as significant as non diabetic cohort Improvements in hypertension, NASH, dyslipidemias, sleep disturbances, QOL Weight loss did not alter need for insulin Improvement in B cell function was not predictable and may correlate with duration of T2DM Dixon et al. Diabetes Care. 2002;25:358-363.

17
4-year case-controlled study LAGB vs Conventional Treatment Group A – Impaired Glucose Tolerance – Prevention 56 LAGB, 29 Diet Progression to T2DM: 0% vs 17.2% Group B - Type II DM - Remission 17 LAGB, 20 pts conventional treatment of T2DM Remission T2DM: 45% vs 4 %

18
Dixon, O’Brien et al, JAMA 2008

19
Study Design: 60 eligible participants (BMI> 30 and 40<kg/m 2 ) with recently diagnosed (<2yrs) type 2 diabetes Prospective Randomized Controlled Trial 55 (92%) completed the program. Treatment: Surgical – LAGB and routine post op care Conventional – “best available medical practice for the treatment, education and follow up of patients with Type II DM”. Lifestyle modification included nutritional counseling, physical activity. Medical treatment including pharmaceutical for DM, weight loss, VLCD determined by physician Main Outcome measure: Remission of type 2 diabetes (fasting glucose <7mmol/L and HbA1c<6.2% while taking no glycemic therapy) Secondary measures included weight and components of the metabolic syndrome.
 Secondary measures included weight and components of the metabolic syndrome..")
20
Table 1:Baseline characteristics of participants Surgery (n = 30) Conventional Therapy (n = 30) Age, mean (SD) 46.6 (7.4) 47.1 (8.7) Men, No. (%) 15 (50) 13 (43) Hypertension, No. (%) 28 (93) 27 (90) Metabolic syndrome, No. (%) 29 (97) 29 (97) Coronary artery disease, No. (%) 0 1 (3) BMI, mean (SD) 37.0 (2.7) 37.2 (2.5) Weight, mean (SD), kg 105.6 (13.8) 105.9 (14.2) Waist circumference, mean (SD), cm 114.1 (10.2) 116.0 (10.0) Waist to hip ratio, mean (SD) 0.96 (0.09) 0.96 (0.10) Neck circumference, mean (SD), cm 41.8 (4.0) 42.4 (4.5) Blood pressure, mean (SD), mm Hg Systolic 136.4 (15.6) 135.3 (14.4) Diastolic 86.6 (9.4) 84.5 (9.8) HbA1c, mean (SD), % 7.8 (1.2) 7.6 (1.4) Plasma glucose, mean (SD), mg/dL 156.7 (38.5) 158.0 (48.7) Plasma insulin, median (IQR), μIU/mL 19.7 (16.5-27.5) 18.7 (13.7-30.7) Lipids, mean (SD), mg/dL Total cholesterol 201.8 (32.7) 198.2 (56.7) Triglycerides 190.6 (106.6) 188.7 (111.8) HDL-C 47.1 (10.1) 48.1 (11.1) Total cholesterol to HDL-C ratio 4.41 (0.87) 4.23 (1.11 )
 15 (50) 13 (43) Hypertension, No. (%) 28 (93) 27 (90) Metabolic syndrome, No. (%) 29 (97) 29 (97) Coronary artery disease, No. (%) 0 1 (3) BMI, mean (SD) 37.0 (2.7) 37.2 (2.5) Weight, mean (SD), kg (13.8) (14.2) Waist circumference, mean (SD), cm (10.2) (10.0) Waist to hip ratio, mean (SD) 0.96 (0.09) 0.96 (0.10) Neck circumference, mean (SD), cm 41.8 (4.0) 42.4 (4.5) Blood pressure, mean (SD), mm Hg Systolic (15.6) (14.4) Diastolic 86.6 (9.4) 84.5 (9.8) HbA1c, mean (SD), % 7.8 (1.2) 7.6 (1.4) Plasma glucose, mean (SD), mg/dL (38.5) (48.7) Plasma insulin, median (IQR), μIU/mL 19.7 ( ) 18.7 ( ) Lipids, mean (SD), mg/dL Total cholesterol (32.7) (56.7) Triglycerides (106.6) (111.8) HDL-C 47.1 (10.1) 48.1 (11.1) Total cholesterol to HDL-C ratio 4.41 (0.87) 4.23 (1.11 ).")
24
Surgical (N=29) Baseline Surgical (N=29) 2 years Conventional Baseline Conventional 2 years No Therapy 22648 Metformin 2832618 Other Oral 8187 Insulin 1003 Not known 0104 Use of Diabetes Medications Other- Surgical Baseline: Glimepride 3, Glicazide 5, Surgical 2-years; Glicazide 1 Conventional Baseline: Glimepride 2, Glicazide 4, Glibenclimide 1, Rosiglitazone 1 Conventional 2-years: Glimepiride 3, Glicazide 3, Glibenclimide 1
 Baseline Surgical (N=29) 2 years Conventional Baseline Conventional 2 years No Therapy Metformin Other Oral 8187 Insulin 1003 Not known 0104 Use of Diabetes Medications Other- Surgical Baseline: Glimepride 3, Glicazide 5, Surgical 2-years; Glicazide 1 Conventional Baseline: Glimepride 2, Glicazide 4, Glibenclimide 1, Rosiglitazone 1 Conventional 2-years: Glimepiride 3, Glicazide 3, Glibenclimide 1")
25
VariableSurgical (N=29) Conventiona l (N=26) 95% CI of between group differences P-value HbA1c (%)6.007.21(1.39) Change (%)-1.81 (1.24)-0.38 (1.26)-2.1, -0.80<0.001 Plasma Glucose (mg/dl) 105.6 (30.3)139.6 (38.1) Change (mg/dl) -51.2 (37.6)-18.4 (41.2)-53.1 -12.30.002 Plasma Insulin (uIU/ml) 9.8 (4.7)24.1 (13.6) Change (uIU/ml)-12.4 (8.4)+1.0 (14.8)-19.6, -7.3<0.001 Glycemic control – 2 Years Mean HbA1c and fasting plasma glucose levels were significantly lower in the surgical group at two years.
 Conventiona l (N=26) 95% CI of between group differences P-value HbA1c (%) (1.39) Change (%)-1.81 (1.24)-0.38 (1.26)-2.1, -0.80<0.001 Plasma Glucose (mg/dl) (30.3)139.6 (38.1) Change (mg/dl) (37.6)-18.4 (41.2) Plasma Insulin (uIU/ml) 9.8 (4.7)24.1 (13.6) Change (uIU/ml)-12.4 (8.4)+1.0 (14.8)-19.6, -7.3<0.001 Glycemic control – 2 Years Mean HbA1c and fasting plasma glucose levels were significantly lower in the surgical group at two years.")
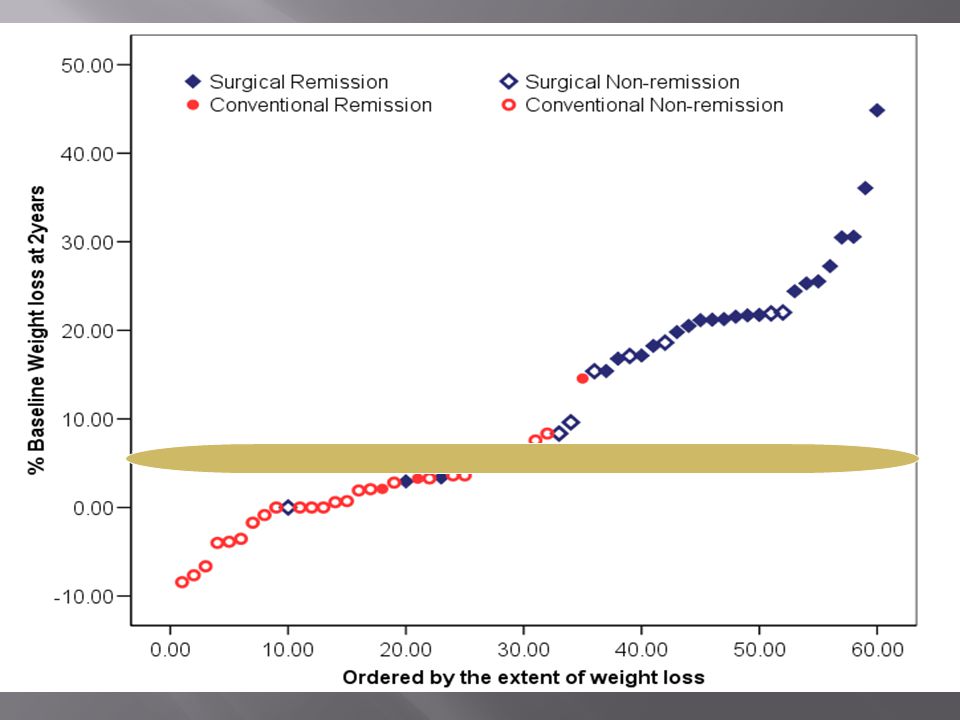
26
Weight loss – 2 Years This study showed that few achieved remission with a body weight loss of less than 10%, a level expected to produce important health benefits. VariableSurgical (N=29) Conventiona l (N=26) 95% CI of between group differences P-value Weight (kg)84.6 (15.8)104.8 (15.3) Change-21.1(10.5)-1.5 (5.4)-23.8, -15.2<0.001 Waist circum95.8 (10.3)112.7 (10.3) Change-17.9(10.8)-4.0 (9.1)-19.0, -8.7<0.001 Waist to Hip ratio 0.90 (0.06)0.95 (0.08) Change-0.06 (0.06)-0.01 (0.06)-0.07, -0.0070/018
 Conventiona l (N=26) 95% CI of between group differences P-value Weight (kg)84.6 (15.8)104.8 (15.3) Change-21.1(10.5)-1.5 (5.4)-23.8, -15.2<0.001 Waist circum95.8 (10.3)112.7 (10.3) Change-17.9(10.8)-4.0 (9.1)-19.0, -8.7<0.001 Waist to Hip ratio 0.90 (0.06)0.95 (0.08) Change-0.06 (0.06)-0.01 (0.06)-0.07, /018.")
27
SurgicalConventionalP value Remission 73%13%<0.001 A1c 6.007.21 Change A1c -1.81-0.38<0.001 % Weight Loss 20.71.7<0.001 % EWL 62.54.3<0.001

28
LAGB assisted weight loss results in diabetes remission in the majority of subjects diagnosed for < 2-years A percentage weight loss of greater than 10-15% provides a high likelihood of remission Lifestyle measures are unlikely to achieve this weight loss This is strong evidence to support the early consideration of surgically induced loss of weight in the management of obese patients with type 2 diabetes.

30
LAGB is the safest bariatric procedure with the lowest morbidity and mortality Only Level 1 evidence to show efficacy in remission of Type II DM is with LAGB Weight loss is more gradual than with other bariatric procedures Remission of T2DM is more gradual Weight loss is sustained if LAGB delivered in the context of a multi-disciplinary long term follow up program

31
LAGB is critically dependant on commitment and follow up on the part of both the patient and the clinic Older studies with previous techniques and older technology are not relevant Studies with low volume and poor follow up are not relevant Obesity and Diabetes are chronic conditions and require sustained weight loss to be successful – short term outcomes are not relevant

32
There seems to be an early effect with duodenal exclusion procedures that we will hear about However, the sustained resolution of diabetes is associated with sustained weight loss Diabetes is a chronic condition so there is rarely a need or benefit to rapid resolution If we are going to offer bariatric surgery for diabetes, we must offer safe and effective options in order to get buy in from endocrinologists We are extending the limits of bariatric surgery so we should do it carefully and with good evidence

33
Dr. Chris Cobourn Surgical Weight Loss Centre Trillium Health Centre Mississauga, Ontario

Similar presentations













 describes relative weight for height: weight (kg)/height (m 2 ) Overweight = 25–29.9 BMI Obesity = >30 BMI.>")













