Download presentation
Presentation is loading. Please wait.

1
WWW.EINSTEIN.BRWWW.SLACIP.COM.BR Trinidad, Buenos Aires, Argentina: 7 a 9 de junio

3
We need to have two primary goals in mind: (1) to ease the work of breathing in the critically ill neonate (2) to reduce the incidence of neonatal lung injury, or bronchopulmonary dysplasia (BPD) Eichenwald & Stark, NEJM 2008
 to ease the work of breathing in the critically ill neonate (2) to reduce the incidence of neonatal lung injury, or bronchopulmonary dysplasia (BPD) Eichenwald & Stark, NEJM 2008")
4
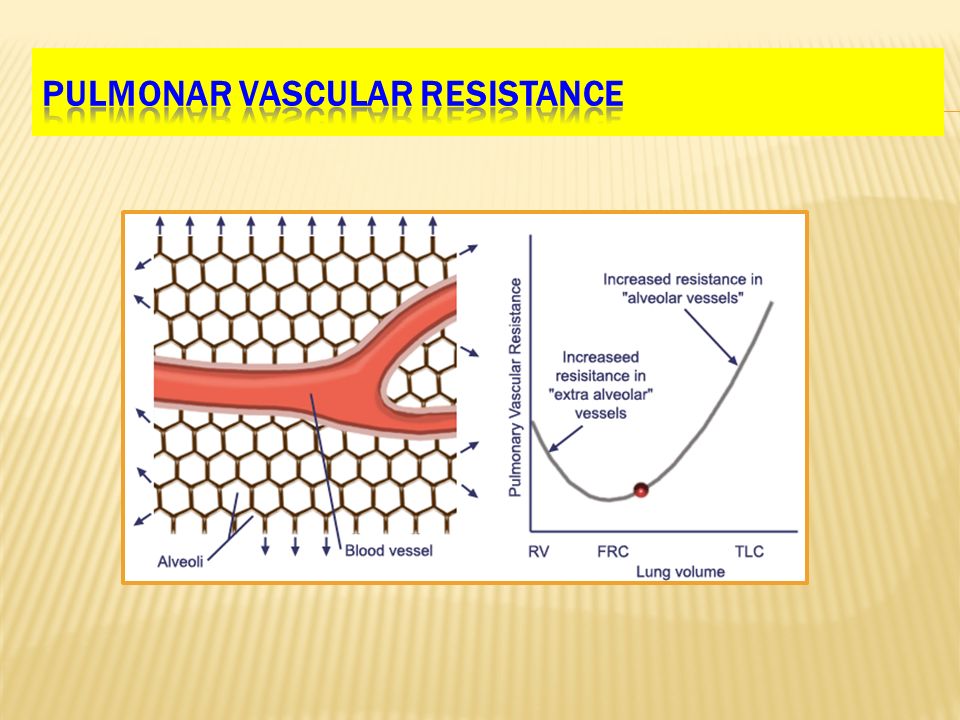
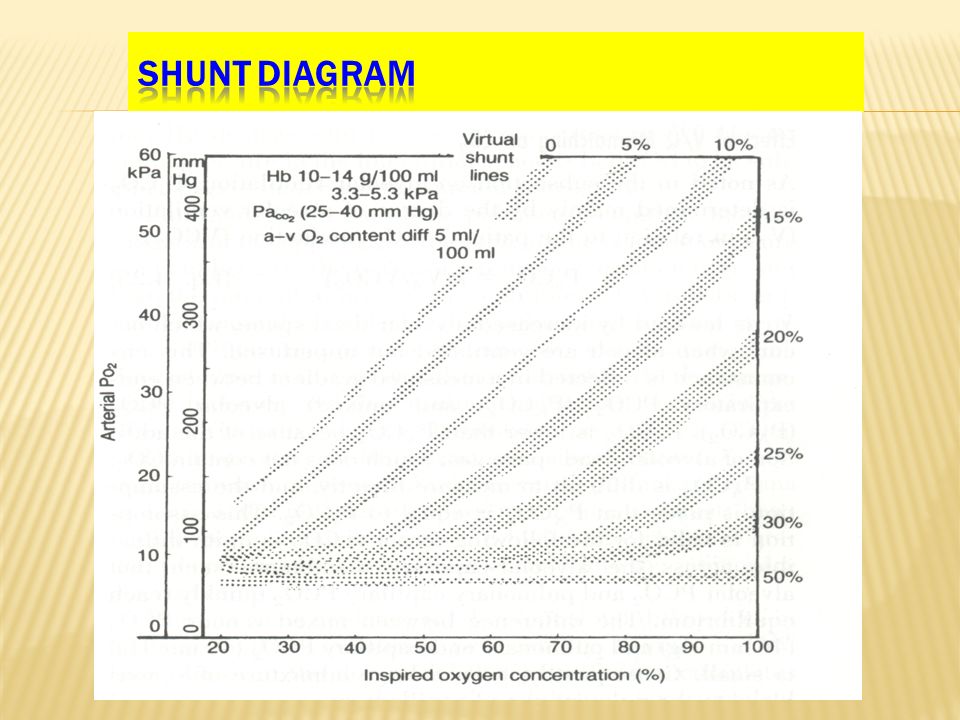
- Positive Pressure Ventilation - Lung Volume and Capacities - Compliance - Airway Resistance - Time Constant - Regional Differences in Perfusion - Pulmonar Vascular Resistance - Shunt Diagram

5
Knowledge of the unique physiology and pathophysiology of the respiratory system of newborn forms the foundation of individualized care that optimizes pulmonary and neurodevelopmental outcomes in our vulnerable patients.

6
Spontaneous Respiration

7
Positive Pressure Ventilation

10
The elastic and resistive forces of the chest, lungs abdomen, airways and ventilator circuit oppose the forces exerted by the respiratory muscles and /or ventilator.

11
Compliance is a measure of the change in volume resulting from a given change in pressure: C L (Lung Compliance) = ▲Volume / ▲Pressure
 = ▲Volume / ▲Pressure")
12
Static Compliance: When measured under static conditions, compliance reflects only the properties of the lung. Static Compliance is measured by determining the transpulmonary pressure change after inflating the lungs with a known volume of gas.

13
Transpulmonary Pressure = Alveolar Pressure – Pleural Pressure It is approximated by measuring pressure at the airway opening and in the esophagus.

14
In the newborn, the chest wall is very compliant; thus large volume changes are achieved with small pressure changes.

15
Plateau Pressure Inspiratory Pressure fluxo Volume Corrente Expiratory Pressure C dyn = Tidal Volume Pinsp-PEEP C st = Tidal Volume Pplateau-PEEP

16
If one measures compliance during continous breathing, the result is called dynamic compliance.

17
Dynamic compliance reflects not only the elastic properties of the lungs but, to some extent, also the resistive component.

18
If one measures compliance during continous breathing, the result is called dynamic compliance. Dynamic compliance reflects not only the elastic properties of the lungs but, to some extent, also the resistive component. It measures the change in pressure from the end of exhalation to the end of inspiration for a given volume and is based on the assumption that at zero flow the pressure difference reflects compliance

19
The steeper the slope of the curve connecting the points of zero flow, the greater the compliance. Dynamic compliance is the compliance that is generally measured in the clinical setting, but its interpretation can be problematic, due to: a) At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent.
 At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent..")
20
The steeper the slope of the curve connecting the points of zero flow, the greater the compliance. Dynamic compliance is the compliance that is generally measured in the clinical setting, but its interpretation can be problematic, due to: a) At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent. b) In premature infants, REM sleep is associated with paradoxical chest wall motion, so pressure changes recorded from the esophagus may correlate poorly with intrathoracic or pleural pressure changes.
 At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent. b) In premature infants, REM sleep is associated with paradoxical chest wall motion, so pressure changes recorded from the esophagus may correlate poorly with intrathoracic or pleural pressure changes..")
21
The steeper the slope of the curve connecting the points of zero flow, the greater the compliance. Dynamic compliance is the compliance that is generally measured in the clinical setting, but its interpretation can be problematic, due to: a) At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent. b) In premature infants, REM sleep is associated with paradoxical chest wall motion, so pressure changes recorded from the esophagus may correlate poorly with intrathoracic or pleural pressure changes. c) Chest wall distortion generally results in underestimation of esophageal pressure changes.
 At the fairly rapid RR common in infants, the instant zero flow may not coincide with the point of lowest pressure. This is because Cd is rate dependent. b) In premature infants, REM sleep is associated with paradoxical chest wall motion, so pressure changes recorded from the esophagus may correlate poorly with intrathoracic or pleural pressure changes. c) Chest wall distortion generally results in underestimation of esophageal pressure changes..")
23
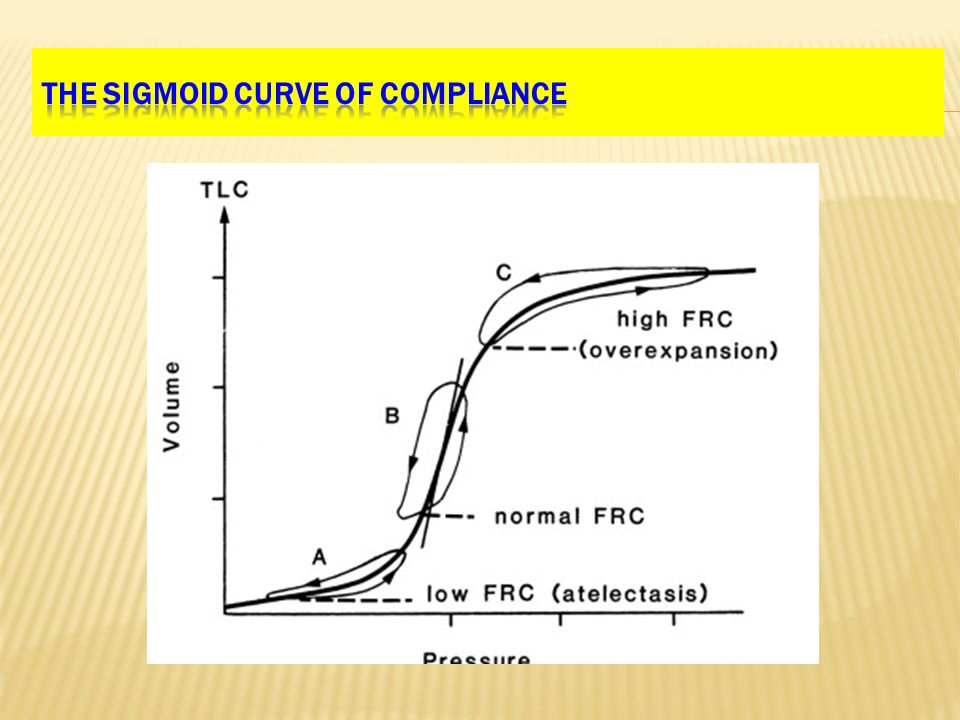
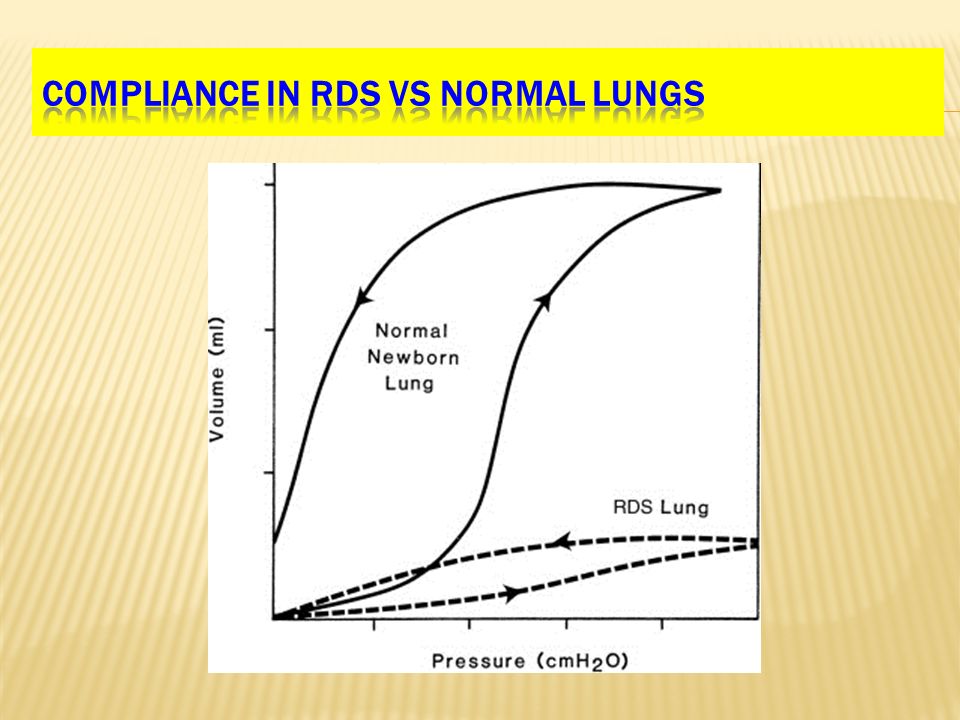
The overall compliance curve is sigmoidal: a) At the lower end of the curve (at low volume) the compliance is low, that is, there is a small change in volume for a large change in pressure. This correlates with underinflation. Pressure is required to open up terminal airways and atelectatic terminal air spaces before gas can move into the lung. The lung volume is starting below critical opening pressure.

24
The overall compliance curve is sigmoidal: b) At the center of curve, the compliance is high; there is a large change in volume for a small change in pressure. This is where normal tidal breathing should occur. This is the position of maximum efficiency in a mechanical sense, the best ventilation/perfusion matching and lowest pulmonary vascular resistance. The best PEEP

25
The overall compliance curve is sigmoidal: c) At the upper end of the curve ( at high volume), the compliance is low; again, there is a small change in volume for a large change in pressure. This correlates with a lung that already is overinflated. Applying additional pressure yields little in terms of additional volume but may contribute significantly to airway injury and compromises venous return because if increased transmission of pressure to the pleural space.

26
It is important to understand that compliance is reduced at both high and low volumes. Low lung volumes are seen in surfactant deficiency states( RDS), whereas high volumes are seen in obstructive lung diseases, such as BPD.
, whereas high volumes are seen in obstructive lung diseases, such as BPD..")
28
The rapid RR of premature infants with surfactant deficiency can compensate for chest wall instability to a certain extent, because the short expiratory time results in gas trapping that tends to normalize their FRC.

29
PEEP: THE HEROPPI: THE KILLER Mechanical ventilation without PEEP leads to surfactatnt inactivation resulting in worsening lung compliance, and repeated cycling of the terminal airways from below critical opening pressure leads to cellular injury and inflammation ( atelectotrauma). This results in alveolar collapse, atelectasis, interstitial edema, and elaboration of inflammatory mediators.

30
AVOID ATELECTASIS OPEN THE LUNG AND KEEP IT OPEN Once atelectasis occurs: - lung compliance deteriorates, - surfactant turnover is increased, - ventilation/perfusion mismatch with increased intrapulmonary right to left shunting develops

31
AVOID ATELECTASIS A higher distending pressure and higher concentrations of FiO2 will be required to maintain lung volume and adequate gas exchange, resulting in further injury

32
THE EARLY THE BETTERBETTER SAFE THAN SORRY Early establishment of an appropriate FRC, administration of surfactant, use of CPAP or PEEP to avoid the repeated collapse and reopening of small airways( atelectotrauma), avoidance of overinflation caused by using supraphysiologic tidal volumes ( volutrauma) and avoidance of use more O2 than is required ( oxidative injury) all are important in achieving the best possible outcome and long-term health of patients.
, avoidance of overinflation caused by using supraphysiologic tidal volumes ( volutrauma) and avoidance of use more O2 than is required ( oxidative injury) all are important in achieving the best possible outcome and long-term health of patients.")
33
THE BEST OR OPTIMUM PEEPBETTER SAFE THAN SORRY The level of PEEP at which static lung compliance is maximized has been termed best or optimum PEEP. This is the level of PEEP at which O2 transport ( Cardiac output and O2 content) is greatest.
 is greatest..")
34
SOMETIMES MORE IS LESS “ as veces menos es más ” If the level of PEEP is raised above the optimal level, dynamic compliance decreases rather than increases. Additionally, venous return and cardiac output are compromised by excessive PEEP

35
If IPP is not reduced as compliance improves, cardiovascular compromise may develop. Also, the distending pressure may become excessive and lead to alveolar overexpansion and ultimately air leak.

36
T he use of volume targeted ventilation would be ideal in the circunstances that the dynamic compliance improves, because in this mode the ventilator will decrease the IPP as lung compliance improves to maintain a set tidal volume.

37
Don’t forget the compliance of the chest wall ! Usually is very compliant in the premature, but in certain clinical scenarios, it may be dificculty to ventilated.

38
The increased intraabdominal presssure with upward pressure on the diaphragm, as may be seen in infants with necrotizing enterocolitis, or after surgical reduction of viscera that had developed outside the abdominal cavity, that is, large omphalocele, gastroschisis or CDH

41
Resistance to flow is defined as a difference in pressure needed to maintain certain flow trough the system R = P / Fluxo

42
A certain pressure is required to deliver the gas through the airways to the alveoli. The flow can be classified as laminar or turbulent. Lei de Pouiselle no fluxo laminar Fluxo = P. π. R 4 / 8. η. L

43
The wider, large airways offer less resistance. The longer is the tube the greater is the resistance R = ΔP/Δ Fluxo = P. π. R 4 / 8. η. L R = 8. η.L / π. R 4

44
Factors determining Airway Resistance: -Properties of the airway and types of flow - Lung volume -Bronchial muscle tone The airway are smaller Resistance of the Airways Newborn – 30 a 50 cmH2O/l/seg (intubated 100 a 150 cmH2O/l/seg) Adult- 1,5 cmH2O/l/seg (intubated - 4,5 a 6 mH2O/l/seg)
 Adult- 1,5 cmH2O/l/seg (intubated - 4,5 a 6 mH2O/l/seg)")
45
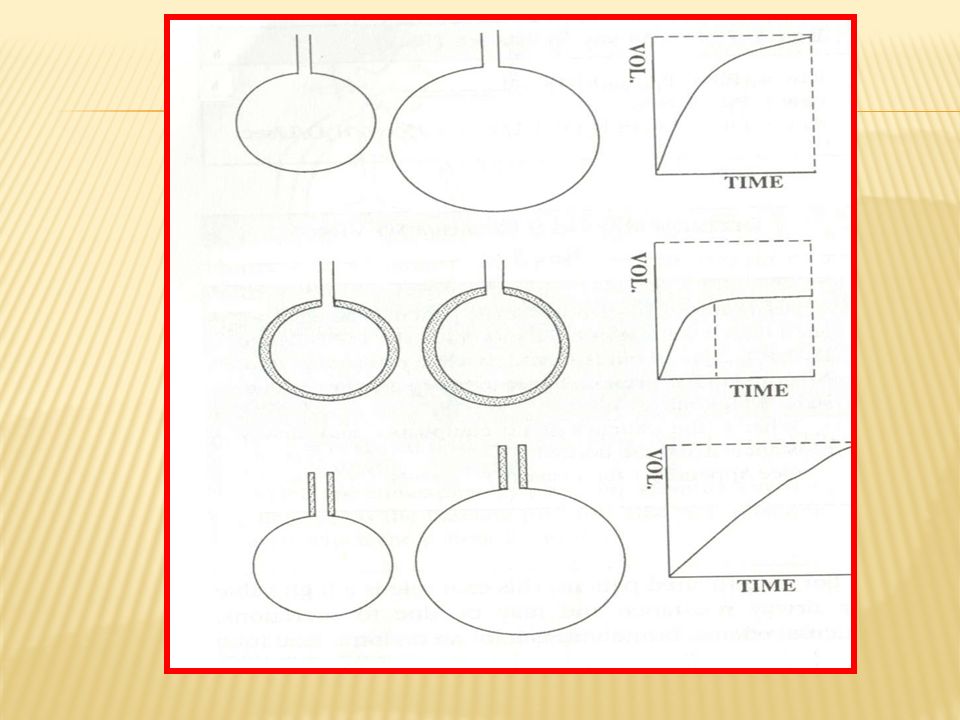
Resistance X Compliance Normal Newborn (1 TC = 0,15 seg) Resistance = 30-50 cmH2O/l/seg Compliance= 0.003 a 0.005 l/cmH2O 100 80 60 40 20 1 2 3 4 5 Time Constant %Pressure change
 Resistance = cmH2O/l/seg Compliance= a l/cmH2O Time Constant %Pressure change")
50
PRESSURE = FLOW X RESISTANCE + VOLUME/COMPLIANCE Pressure Flow Volume Compliance = Δ volume Δ pressure Resistance = Δ pressure Δ flow

51
VOLUME PRESETPRESSURE PRESET Volume Preset ventilators: deliver the same tidal volume of gas each breath, regardless of the inflating pressure that is needed. Pressure-preset ventilators,: in contrast, are designed to deliver a volume of gas with each breath until a preset limiting pressure designated by the physician is reached.

52
http://www.einstein.br/ensino/eventos-cientificos

53
WWW.EINSTEIN.BRWWW.SLACIP.COM.BR Trinidad, Buenos Aires, Argentina: 7 a 9 de junio

Similar presentations
















 2. Airways resistance work30% 3. Moving tissues 5% Normally >")



