Download presentation
Presentation is loading. Please wait.

1
Applying the Surviving Sepsis Campaign Guidelines to Clinical Practice
Ruth M. Kleinpell PhD RN FCCM Rush University Medical Center Chicago, Illinois USA; President, World Federation of Critical Care Nurses

2
Conflict of Interest “I believe there is value in the use of clinical practice guidelines, but at the same time acknowledge their limitations”

3
Clinical Practice Guidelines: Origins
The Georg Ebers Papyrus. Found in Egypt in the 1870’s, outlines more than 700 remedies, including this one for an acute asthma attack Hieroglyphics outlining treatments for more than 700 remedies, circa 1552 BC

4
Clinical practice guidelines are recommendations for clinicians about the care of patients with specific conditions. They should be based on the best available evidence and practice experience.

5
Using Guidelines in Clinical Practice
On average, what percent of healthcare clinicians apply guidelines in clinical practice? 12% 20% 50% 75%

6
30 studies, representing 11,611 clinician responses
Guidelines were helpful sources of advice (75%) Good educational tools (71%) Intended to improve quality (70%) Too rigid to apply to individual patients (30%) Reduced clinician autonomy (34%) Oversimplified medicine (34%) Medical Journal of Australia; ; 2002;177:;
 Good educational tools (71%) Intended to improve quality (70%) Too rigid to apply to individual patients (30%) Reduced clinician autonomy (34%) Oversimplified medicine (34%) Medical Journal of Australia; ; 2002;177:;")
7
Fact: The Interpretation of Medical Guidelines
is Somewhat Subjective

8
Fact: Not all Guidelines are Clear In Their Interpretation

9
2011

10
Kung J et al JAMA Internal Medicine 2012;172:1628-1633

11
Kung J et al JAMA Internal Medicine 2012;172:1628-1633

12
How Does This Apply to Sepsis?

13
Critical Care Medicine 2013;41:580-637

15
Evidence-based recommendations
Outline the management of severe sepsis and septic shock Identify key recommendations for treatment The GRADE system Grade 1 – Strong Grade 2 – Weak Quality of Evidence: Grade A – High Grade B – Moderate Grade C – Low Grade D – Very Low Grading of Recommendations Assessment, Development and Evaluation Dellinger RP et al. Critical Care Medicine 2013;41:

17
Despite limitations, the guidelines represent an important advance
in the management of patients with severe sepsis. Although a number of recommendations were based on low-quality evidence, strong agreement existed among international experts regarding many level 1 recommendations as the best care for patients with sepsis.

18
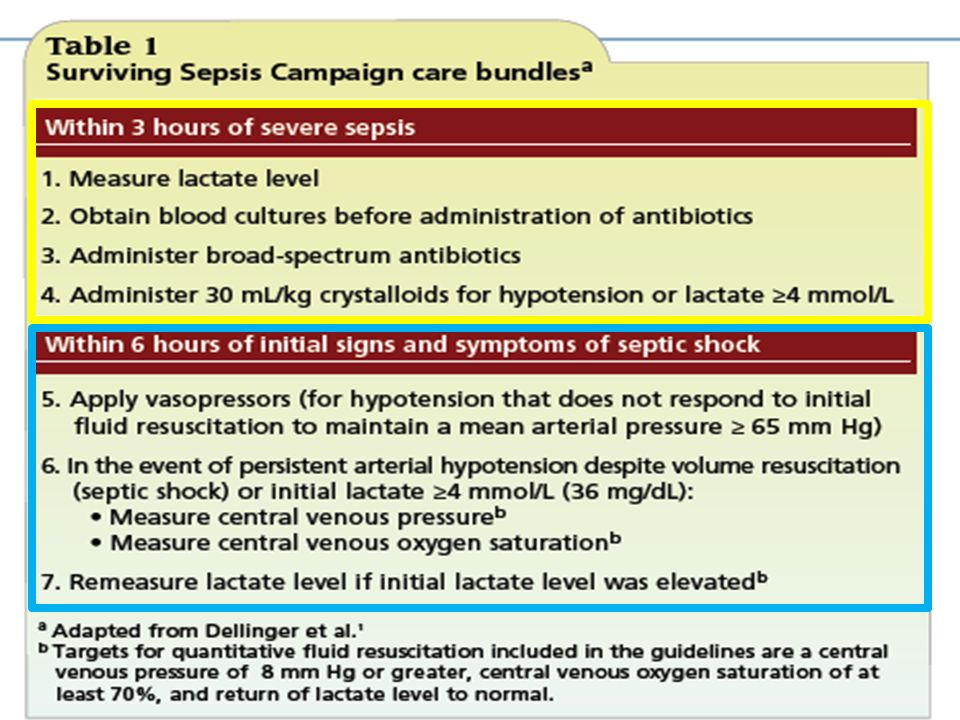
Basic care tasks [microbiological sampling and antibiotic delivery
within 1 hour, fluid resuscitation, and risk stratification using serum lactate] are likely to benefit patients most, yet are unreliability performed. Barriers include lack of awareness, lack of supporting controlled trials and complex diagnostic criteria leading to recognition delays.

19
620 bed University Medical Center, Chicago Illinois
22 bed Surgical ICU 21 bed Medical ICU 25 bed NeuroSurgical ICU 25 bed CCU/CSU Total ICU admissions/year = 8,349

20
Clinical Example Rush University Medical Center
Sepsis Initiative ■Started as educational initiative to promote awareness of new sepsis protocol. ■ Evolved to QI project to assess the impact of an educational initiative and focused follow up on protocol implementation.

21
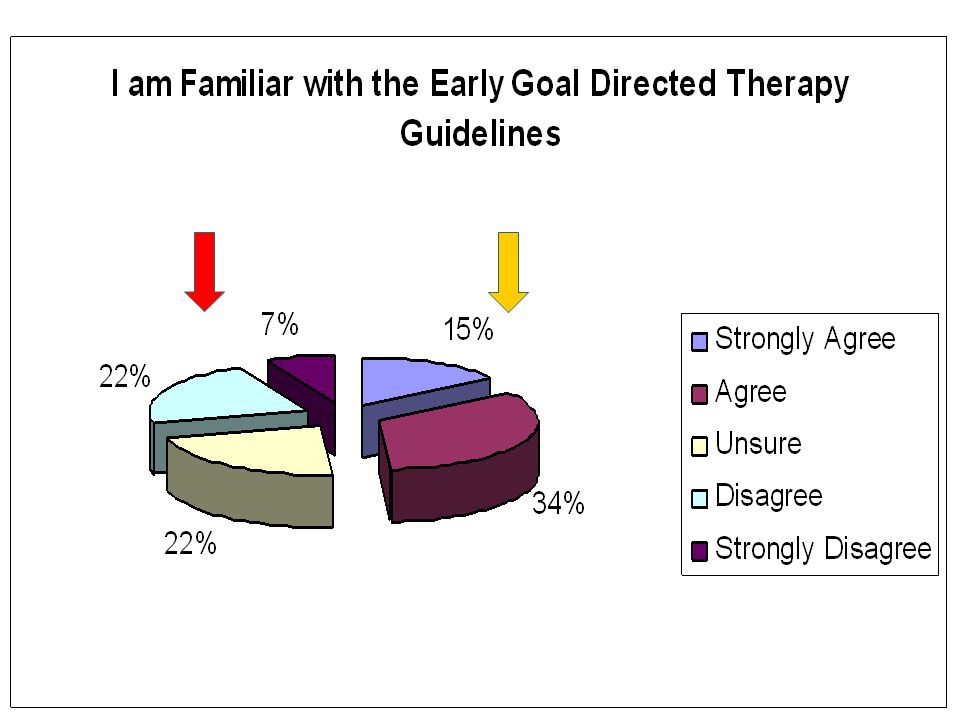
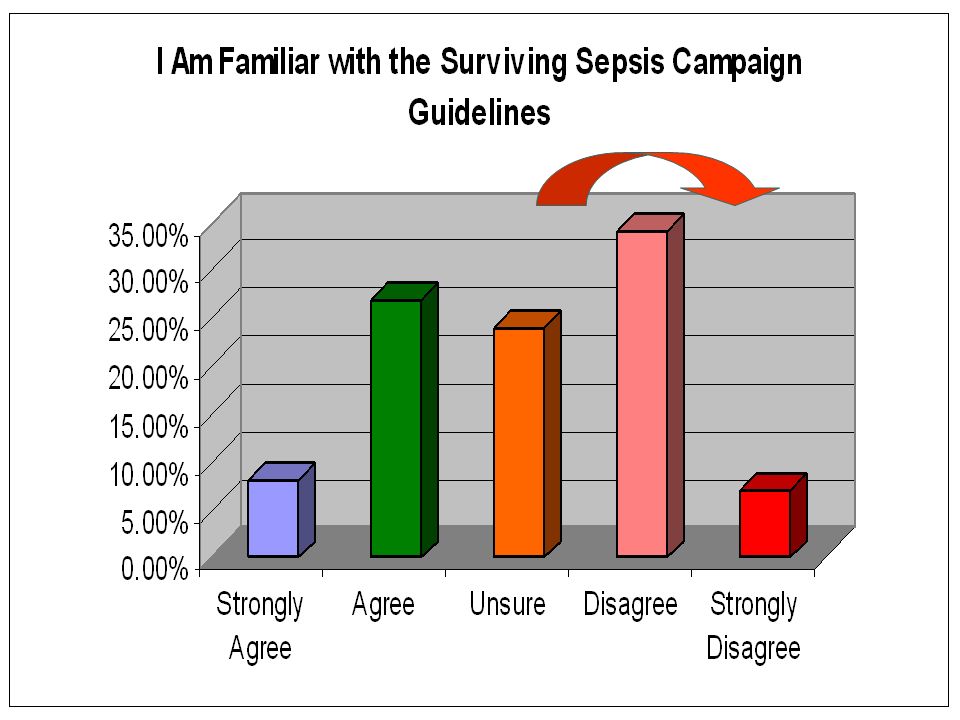
Clinical Example: Sepsis Protocol Implementation
Surveys conducted prior to protocol implementation N=240 respondents (MDs, RNs, PharmD, Therapists)
")
26
New Focus Area Screening for Sepsis & Performance Improvement
We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early identification of sepsis and allow implementation of early sepsis therapy (grade 1C). Performance improvement efforts in severe sepsis should be used to improve patient outcomes (UG). Dellinger RP et al. Critical Care Medicine 2013;41:
. Performance improvement efforts in severe sepsis should be used to improve patient outcomes (UG). Dellinger RP et al. Critical Care Medicine 2013;41:")
27
Using Performance Improvement to Target Sepsis

28
Strategies for Implementing Sepsis Performance Improvement
Identify gaps in care and specific areas for improvement Time to blood cultures Time to antibiotics Time to lactate levels Time to fluid bolus goals Targeting Sepsis as a Performance Improvement Metric: AACN Clinical Issues, In Press

29
Initial Resuscitation
We recommend the protocolized resuscitation of a patient with sepsis-induced shock, defined as tissue hypoperfusion (hypotension persisting after initial fluid challenge or blood lactate concentration 4 mmol/L). During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol: Central venous pressure (CVP): 8–12mm Hg Mean arterial pressure (MAP) ≥ 65mm Hg Urine output ≥ 0.5mL.kg–1.hr –1 Central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively (Grade 1C) Lactate:2C Dellinger RP et al. Critical Care Medicine 2013;41:
. During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol: Central venous pressure (CVP): 8–12mm Hg. Mean arterial pressure (MAP) ≥ 65mm Hg. Urine output ≥ 0.5mL.kg–1.hr –1. Central venous (superior vena cava) or mixed venous oxygen saturation ≥ 70% or ≥ 65%, respectively. (Grade 1C) Lactate:2C. Dellinger RP et al. Critical Care Medicine 2013;41:")
30
Fluid therapy We recommend crystalloids be used in the initial fluid resuscitation in patients (Grade 1B). We recommend that initial fluid challenge in patients with sepsis-induced tissue hypoperfusion with suspicion of hypovolemia to achieve a minimum of 30ml/kg. (Grade 1C). Dellinger RP et al. Critical Care Medicine 2013;41:
. Dellinger RP et al. Critical Care Medicine 2013;41:")
32
Strategies for Implementing Sepsis Performance Improvement
Identify gaps in care and specific areas for improvement Compliance to elements of the 3 hour bundle Compliance to elements of the 6 hour bundle Targeting Sepsis as a Performance Improvement Metric: AACN Clinical Issues, In Press

33
Diagnosis We recommend obtaining appropriate cultures before antimicrobial therapy is initiated if such cultures do not cause significant delay (>45 minutes) in antimicrobial administration. To optimize identification of causative organisms, we recommend at least two blood cultures be obtained before antimicrobial therapy with at least one drawn percutaneously and one drawn through each vascular access device, unless the device was recently (<48 hr.) inserted (1C) Dellinger RP et al. Critical Care Medicine 2013;41:
 in antimicrobial administration. To optimize identification of causative organisms, we recommend at least two blood cultures be obtained before antimicrobial therapy with at least one drawn percutaneously and one drawn through each vascular access device, unless the device was recently (<48 hr.) inserted (1C) Dellinger RP et al. Critical Care Medicine 2013;41:")
34
Antibiotic therapy We recommend that intravenous antimicrobial therapy be started as early as possible and within the first hour of recognition of septic shock (1B) and severe sepsis without septic shock (grade1C). We recommend that initial empiric anti-infective therapy include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) (grade 1B).
 and severe sepsis without septic shock (grade1C). We recommend that initial empiric anti-infective therapy include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) (grade 1B).")
35
Vasopressors We recommend that vasopressor therapy initially target a mean arterial pressure (MAP) of 65 mm Hg (grade 1C). We recommend norepinephrine as the first choice vasopressor (Grade 1 B). Dellinger RP et al. Critical Care Medicine 2013;41:
. Dellinger RP et al. Critical Care Medicine 2013;41:")
36
Strategies for Implementing Sepsis Performance Improvement
Identify gaps in care and specific areas for improvement Glucose value levels < 180 mg/dL Sedation targeted to specific endpoints Nutritional support Targeting Sepsis as a Performance Improvement Metric: AACN Clinical Issues, In Press

37
2008 Surviving Sepsis Campaign Guidelines
Consideration for limitation of support (1D) Discuss end-of-life care for critically ill patients Promote family communication to discuss use of life-sustaining therapies 1D = Very Low Quality of Evidence Dellinger RP et al Crit Care Med 2008; 36:
 Discuss end-of-life care for critically ill patients. Promote family communication to discuss use of life-sustaining therapies. 1D = Very Low Quality of Evidence. Dellinger RP et al Crit Care Med 2008; 36:")
38
Consideration for Limitation of Support
Setting Goals of Care Recommendation 1: We recommend that identification of goals of care, prognosis for achieving those goals and the level of certainty for the prognosis be discussed with patients and families. (1B) Recommendation 2: We recommend that these communications should be incorporated into treatment plans with integration of palliative care principles, and as appropriate, end-of-life care planning. (1B) Recommendation 3: It is suggested that goals of care be addressed as early as feasible but no later than within 72 hours. (Grade 2C) Dellinger RP et al. Critical Care Medicine 2013;41:
 Recommendation 2: We recommend that these communications should be incorporated into treatment plans with integration of palliative care principles, and as appropriate, end-of-life care planning. (1B) Recommendation 3: It is suggested that goals of care be addressed as early as feasible but no later than within 72 hours. (Grade 2C) Dellinger RP et al. Critical Care Medicine 2013;41:")
39
Strategies for Implementing Sepsis Performance Improvement
Identify gaps in care and specific areas for improvement Patients receiving family care conference to address goals of care within 72 hours of ICU admission Targeting Sepsis as a Performance Improvement Metric: AACN Clinical Issues, In Press

43
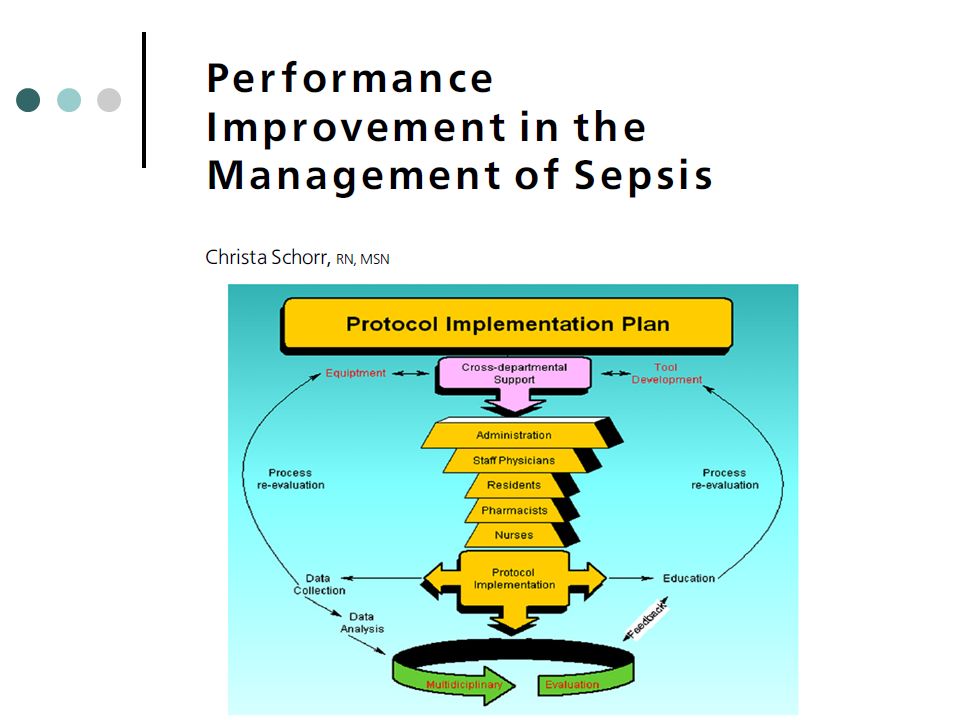
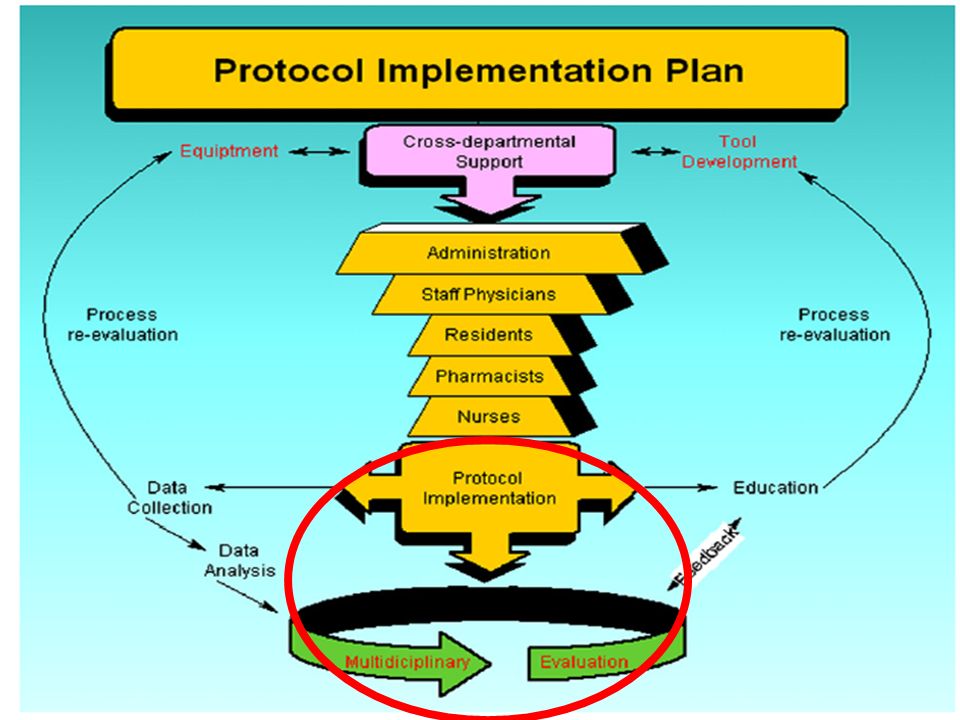
Performance Improvement
The focus on the new Surviving Sepsis Campaign is not only on the early identification and treatment of patients, but on the recognition that nurses are critical to performance improvement and data collection

44
Available full text open access
45
Reliable timely delivery of more complex life-saving tasks demands
greater awareness, faster recognition and initiation of basic care, and more effective collaboration between clinicians and nurses on the front line.

46
Summary: Optimizing Outcomes in Sepsis
Role of Astute Clinical Assessment EARLY: Recognition Treatment Judicious application of guideline recommendations

47
Congratulations!

49
Dank Je

Similar presentations
























, Society of Critical Care Medicine (SCCM), and the International Sepsis Forum (ISF) developed.>")