Download presentation
Presentation is loading. Please wait.

1
ANKYLOSING SONDYLITIS
Ankylosing spondylitis (AS) is characterised by a chronic inflammatory arthritis predominantly affecting the sacroiliac joints and spine, which can progress to bony fusion of the spine.
 is characterised by a chronic inflammatory arthritis predominantly affecting the sacroiliac joints and spine, which can progress to bony fusion of the spine.")
2
It has a peak onset in the second and third decades, with a male:female ratio of about 3:1.
In Europe, more than 90% of those affected are HLA-B27- positive

3
AS is thought to result from exposure to a common environmental pathogen in genetically susceptible individuals, although no specific trigger has been identified. Chronic prostatitis is more common than expected but appears to be non-infective in origin.

4
Increased faecal carriage of Klebsiella aerogenes occurs in patients with established AS and may relate to exacerbation of both joint and eye disease.

5
Clinical features The onset is usually insidious, with recurring episodes of low back pain and marked stiffness

6
. Radiation of pain to the buttocks or posterior thighs may be misdiagnosed as sciatica.
Unlike mechanical back pain, symptoms extend over many segments and are axial and symmetrical in distribution

7
Symptoms are most marked in the early morning and after inactivity, and are relieved by movement.
Although the lumbosacral area is usually the first and worst affected region, some patients present with mainly thoracic or neck symptoms

8
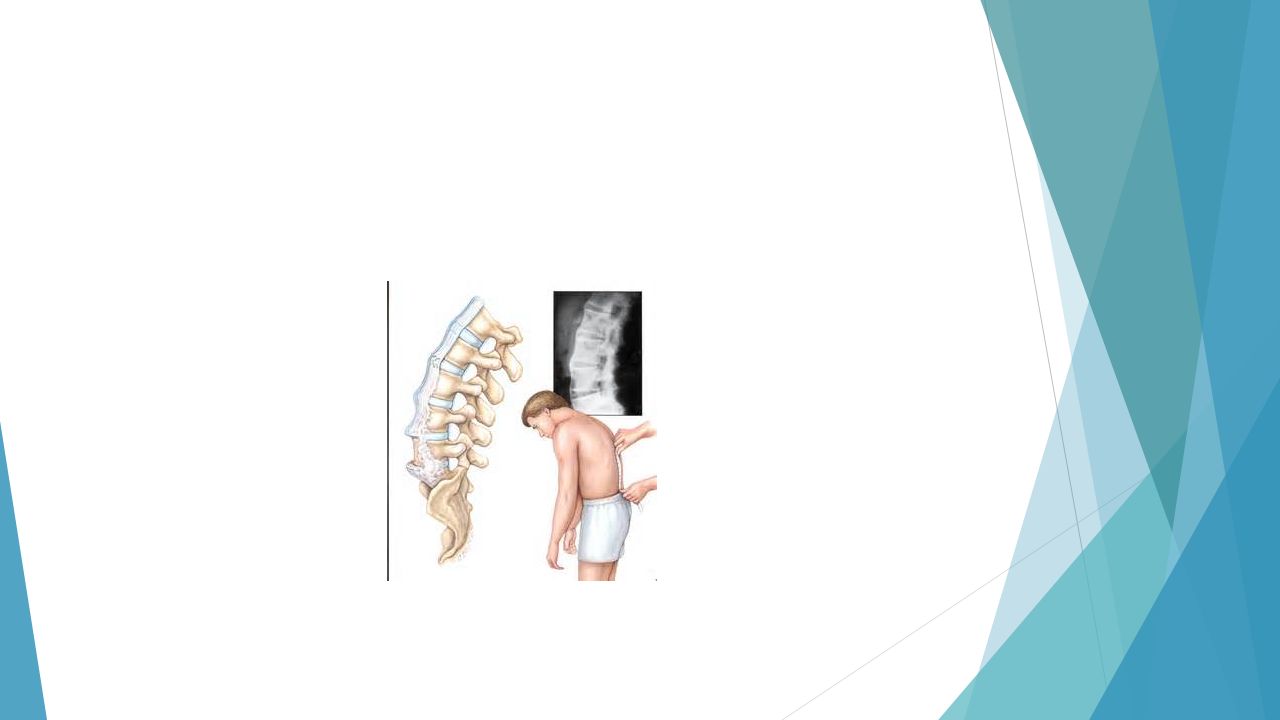
Early physical signs include failure to obliterate the lumbar lordosis on forward flexion, restriction of movements of the lumbar spine in all directions, and possible pain on sacroiliac stressing.

9
As the disease progresses, stiffness increases throughout the spine, and chest expansion frequently becomes restricted. Spinal fusion varies in its extent and in most cases does not cause a gross flexion deformity

10
Pleuritic chest pain aggravated by breathing is common and results from costovertebral joint involvement.

11
Plantar fasciitis, Achilles tendinitis and tenderness over bony prominences such as the iliac crest and greater trochanter are common, reflecting inflammation at the sites of tendon insertions

12
Peripheral arthritis Up to 40% of patients have peripheral arthritis. This is usually asymmetrical at first, mainly affecting hips, knees, ankles or shoulders. Involvement of a peripheral joint, most commonly ankle, knee or elbow, may precede the development of spinal symptoms in around 10% of cases.

13
In a further 10%, symptoms begin in childhood as one variety of pauciarticular juvenile idiopathic arthritis

14
Extra-articular features of ankylosing spondylitis
Anterior uveitis (25%) and conjunctivitis (20%) Prostatitis (80% men): usually asymptomatic Cardiovascular disease Aortic incompetence Mitral incompetence Cardiac conduction defects Pericarditis Amyloidosis Atypical upper lobe pulmonary fibrosis Extra-articular features of ankylosing spondylitis
 and conjunctivitis (20%) Prostatitis (80% men): usually asymptomatic. Cardiovascular disease. Aortic incompetence. Mitral incompetence. Cardiac conduction defects. Pericarditis. Amyloidosis. Atypical upper lobe pulmonary fibrosis. Extra-articular features of ankylosing spondylitis.")
16
Investigations X-ray changes are characteristic but may take years to develop. Sacroiliitis is often the first abnormality, beginning in the lower synovial parts of the joints with irregularity and loss of cortical margins, widening of the joint space and subsequently sclerosis, narrowing and fusion. MRI is more sensitive for detection of early sacroiliitis, but is seldom required.

17
Lateral thoracolumbar spine X- rays may show anterior 'squaring' of vertebrae due to erosion and sclerosis of the anterior corners and periostitis of the waist

18
The ESR and CRP are usually raised in active disease
The ESR and CRP are usually raised in active disease. RF and other autoantibodies are usually negative. Testing for HLA-B27 can be a helpful investigation for pauciarticular juvenile idiopathic arthritis but is unhelpful in adults with spinal symptoms

26
MANAGEMENT The aims are to relieve pain and stiffness, maintain a maximal range of skeletal mobility and avoid the development of deformities. Education and appropriate physical activity are the cornerstones of management.

27
Early in the disease, patients should be taught to perform daily back extension exercises, including a morning 'warm-up' routine, and to punctuate prolonged periods of inactivity with regular breaks. Swimming is ideal exercise. Poor posture must be avoided.

28
NSAIDs and analgesics are often effective in relieving symptoms but do not alter the course of the disease. A long-acting NSAID at night is helpful for marked morning stiffness

29
. Peripheral arthritis can be treated with methotrexate or sulfasalazine, but these drugs have no effect on axial disease

30
Anti-TNF therapy should be considered for disease inadequately controlled by these measures since it often has a significant impact on axial symptoms

31
Local corticosteroid injections can be useful for persistent plantar fasciitis, other enthesopathies and peripheral arthritis.

32
Oral corticosteroids may be required for acute uveitis but do not help spinal disease.
Total hip arthroplasty has largely removed the need for difficult spinal surgery in those with advanced deformity.

33
Severe hip, knee or shoulder restriction may require surgery.

Similar presentations

















 and most often affects.>")



 is the name for a family of inflammatory rheumatic diseases that cause.>")




