Download presentation
Presentation is loading. Please wait.

1
Prof. Amgad Fouad Gastroenterology center Mansoura University

2
Achalasia of the esophagus, different line for therapy

3
Achalasia –Greek word –Failure to relax –Willis (1672)
")
4
Zenker & Vonziemssen (1877): Diminished contractile power of the esophageal musculature. Meltzer & Miklicz (1888): Spasmodic contraction of the cardiac sphincter. Einhorn (1888): Failure of relaxation of the cardia on swallowing. Horst (1929): Established the term achalasia (failure to relax).
: Spasmodic contraction of the cardiac sphincter. Einhorn (1888): Failure of relaxation of the cardia on swallowing. Horst (1929): Established the term achalasia (failure to relax)..")
5
Achalasia : –The most recognised motor disorder of the esophagus. –Cardinal features: Poorly relaxing LES Prolonged esophageal transit Defective esophageal body peristalsis.

6
1-2 / 200.000 ♂ = ♀. Any age. Onset 3 rd – 5 th decade. Duration of symptoms at presentation 2 years average. (Mayberry & Atkinson, 1985)
.")
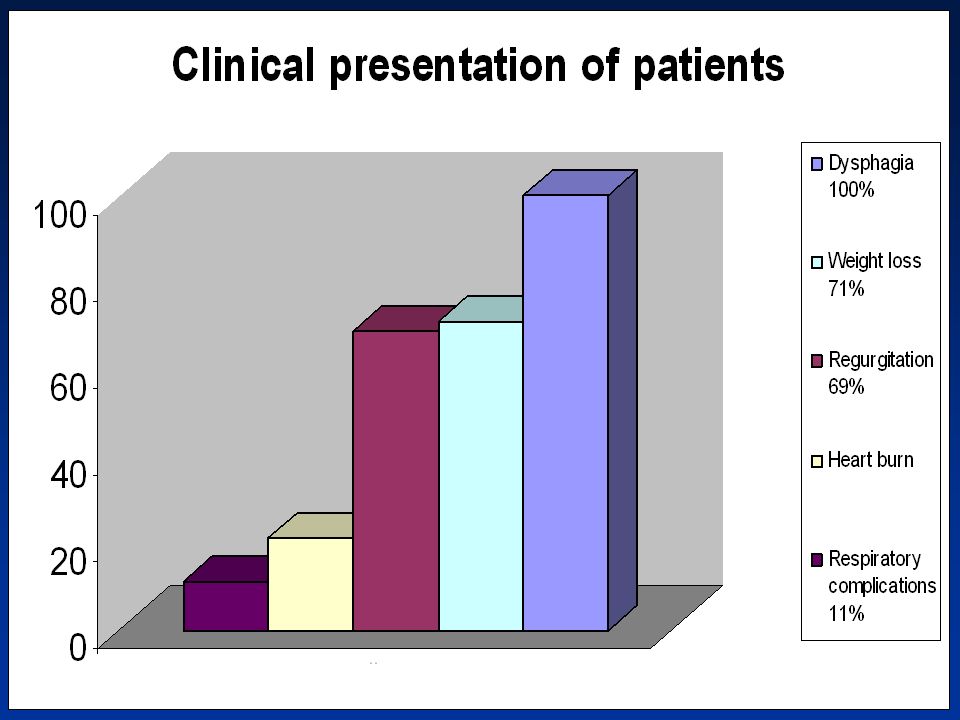
7
Presentation Dysphagia (almost 100%) Regurgitation (60-90%) Chest pain (30 – 50%) Wt loss (Advanced disease). Pulmonary symptoms. –Bronchopneumonia –Lung abscess –Ht burn (rare presentation )
.")
8
Diagnosis –Compatible clinical history. –Radiography. –Endoscopy. –Manometry.

9
Radiographic studies Plain X ray : Widened mediastinum. Air fluid level Absence of gastric air bubble Evidence of pulmonary complications

10
(continue) Radiographic studies (continue) Barium swallow Screening test Esophageal body dilated Lower end esophagus → tapered point. (birds Beak ) Nitrite test → Diagnostic.
 Nitrite test → Diagnostic..")
11
Radiographic staging Stage I : Slight dilatation of the body not >3.5cm. Stage II : Moderate dilatation 3.5-6cm. Stage III : Marked dilatation >6cm. Stage IV : Marked dilatation elongation and tortiousity of the esophagus (sigmoid esophagus).
..")
12
Endoscopy Important diagnostic tool Rule out several diseases that mimic achalasia. Evaluate esophageal mucasa before therapeutic manipulation. Typical finding Dilated esophgeal body Puckered closed LES No organic stricture

13
Mamometry Confirms & establishes the diagnosis Features: Essential features Absence of esophgeal body peristalsis (1ry peristaltic waves) ↑ intraesophageal resting pressure. Abnormal LES relaxation. Supportive Features Hypertensive LES pressure Low amplitude esophageal contractions (Castell, 1996)
.")
14
☺Treatment of Achalasia

15
Medical Treatment Nitrates. Ca ++ channel blockers Anticholinergic drugs All have been shown to reduce the force of contraction of esophageal body smooth muscles. May be of value in reducing chest pain & improving dysphagia (Gelfond et al., 1982)
.")
16
Botulinum toxin Neurotoxin produced by clostridium botulinum. Only serotype A+B have been approved for clinical use. Two preparations of BTX (A) available: Dysport (UK) Botox (USA)
 available: Dysport (UK) Botox (USA).")
17
Efficacy of BTX in achalasia Response 6 mo (%) Response 1 mo (%)Dose No. of patients Study designYearAuthor Adults 609080 U10OL1994 Pasricha 669080 U31DBPC1995 Pasricha 53100100 U8DBPC1996 Annese 418080U42OL1999 Prakash 3688200 U40MCRT2000 Annese 6584100 U37OL2002 D'Onofrio Children 438380-100U23OL2000 Hurwitz 3310030U7OL2000 IP

18
Pneumatic dilatation The most effective non-surgical treatment option. Forceful dilatation using air or water pressure can be applied to the lower esophageal segment and controlled to secure further stretching to the point of rupture of the circular ms fibers.

19
Recommended technique for pneumatic balloon dilatation (Voizi et al, 1994) Fasting for at least 12 h before procedure. 1 Esophageal lavage with a large-bore tube (if needed). 2 Sedation and endoscopy in Rt lateral position. 3 Guidewire positioned in stomach and balloon passed over the guidewire. 4 Initial dilatation with 3-cm diameter balloon; subsequent progression to 3.5-cm and 4- cm balloons may be required at separate sessions. 5 Accurate placement of balloon across gastroesophageal junction fluoroscopically. 6 Balloon distention to obliterate the waist, which usually requires 7-10 psi (this is the key to a successful dilatation) 7 Gastrograffin study followed by barium swallow to exclude esophageal perforation. 8 Observation for 4 h for chest pain and fever. 9 Discharge with follow-up in 1 mo. 10 * Before proceeding with pneumatic dilatation, it is important to ensure that a cardiothoracic surgeon is available in case of an esophageal perforation.
. 2 Sedation and endoscopy in Rt lateral position. 3 Guidewire positioned in stomach and balloon passed over the guidewire. 4 Initial dilatation with 3-cm diameter balloon; subsequent progression to 3.5-cm and 4- cm balloons may be required at separate sessions. 5 Accurate placement of balloon across gastroesophageal junction fluoroscopically. 6 Balloon distention to obliterate the waist, which usually requires 7-10 psi (this is the key to a successful dilatation) 7 Gastrograffin study followed by barium swallow to exclude esophageal perforation. 8 Observation for 4 h for chest pain and fever. 9 Discharge with follow-up in 1 mo. 10 * Before proceeding with pneumatic dilatation, it is important to ensure that a cardiothoracic surgeon is available in case of an esophageal perforation..")
20
Cumulative effectiveness of pneumatic dilatation in Achalasia Perforation (%) Follow- up (yr) Mean (Range) % Sx Improvement Objective Assessments Dilator (Size/cm) Study Design Number of Patients Reference Excellent/Goo d %LES Pressure 00.8(0.5-1)863Prospective7Cox 070,9360,683.4Prospective24Gelfand 01.3(0.1-3.4)903.5Prospective50Barkin 00.5743.5Prospective10Stark 5.90.550,75,753, 3.5, 4Retrospective17Makela 085,883, 3.5Retrospective62Levine 04(0.3-6)62,79,93673, 3.5, 4Prospective29Kadakia 0.375393, 3.5Prospective14Kim 73, 3.5, 4Prospective28Lee
 Follow- up (yr) Mean (Range) % Sx Improvement Objective Assessments Dilator (Size/cm) Study Design Number of Patients Reference Excellent/Goo d %LES Pressure 00.8(0.5-1)863Prospective7Cox 070,9360,683.4Prospective24Gelfand 01.3( )903.5Prospective50Barkin Prospective10Stark ,75,753, 3.5, 4Retrospective17Makela 085,883, 3.5Retrospective62Levine 04(0.3-6)62,79,93673, 3.5, 4Prospective29Kadakia , 3.5Prospective14Kim 73, 3.5, 4Prospective28Lee")
21
Perforation (%) Follow-up (yr) Mean (Range) % Sx Improvement Objective Assessments Dilator (Size/cm) Study Design Number of PatientsReference Excellent/Good %LES Pressure 085,883, 3.5Retrospective62Levine 04(0.3-6)62,79,93673, 3.5, 4Prospective29Kadakia 0.375393, 3.5Prospective14Kim 73, 3.5, 4Prospective28Lee 6.62.3(1-4)88,893.5, 4Retrospective36Abid 2.5 89423, 3.5Retrospective40Wehrmann 01.8(0.1-4.8)673Retrospective27Lambroza 01.2(0.3-3)73,933, 3.5Prospective15Bhatnagar 7/345=2%1.6(0.1-6)yr125/168=74%size 3359Total 184/214=86%Size 3.5 90/100=90%size 4 Continue
 Follow-up (yr) Mean (Range) % Sx Improvement Objective Assessments Dilator (Size/cm) Study Design Number of PatientsReference Excellent/Good %LES Pressure 085,883, 3.5Retrospective62Levine 04(0.3-6)62,79,93673, 3.5, 4Prospective29Kadakia , 3.5Prospective14Kim 73, 3.5, 4Prospective28Lee (1-4)88,893.5, 4Retrospective36Abid , 3.5Retrospective40Wehrmann 01.8( )673Retrospective27Lambroza 01.2(0.3-3)73,933, 3.5Prospective15Bhatnagar 7/345=2%1.6(0.1-6)yr125/168=74%size 3359Total 184/214=86%Size /100=90%size 4 Continue")
22
Surgical management of Achalasia Rationale of surgery is to weaken the lower esophageal sphincteric pressure but in controlled Faison avoiding subsequent reflux (Earlam, 1976)
")
23
Heller (1913) First performed extra mucosal cardiorytomy. Two 8cm incisions one ant & one post. Incisions extending 2cm into the dilated part cranially & into the fundus of the stomach caudally.

24
Modified Heller’s myotomy (Zaaijer, 1985) Most widely used technique. Single anterior myotomy. Transabdominal. However Two problems →poor results 1.Incomplete myotomy 2.Reflux esophagitis.

25
Anti – Reflux

26
Laparoscopic Heller’s Most preferred by gastrointestinal laparoscopic surgeon. Easy access. Good result Anti – reflux +

27
Results of Heller Esoph Perf Morb (%) Mort (%)F/U % Reg % Dys % SATNo.ProcedureAuthor (Year) Laparotomy NA 04 y4 y192566108Heller/PostBlack et al (1976) 02.3062 mo28219542Heller/DCsendes et al (1989) 08.305.4 yr449248Heller/PostParicio et al (1990) NA 06 mo-15 yr NR 95722Heller/PostPinotti et al (1991) 01.9064.5 mo9494206Heller/DBonavina et al (1992) Thoracotomy 05.608 yr6780102HellerMenzies-Gow et al (1978) NA 085 mo4811INR145HellerJara et al (1979) 1%1%NA0.26.5 yr3385468Heller/B or A Okike et al (1979) 02.303 mo-19 yr IN R 9344Heller/DFYong-xian (1982) 09.606.75 yr4591103HellerEllis et al (1984) NA 1.84.8 yr968857Heller/BLittle et al (1988)
 Mort (%)F/U % Reg % Dys % SATNo.ProcedureAuthor (Year) Laparotomy NA 04 y4 y Heller/PostBlack et al (1976) mo Heller/DCsendes et al (1989) yr449248Heller/PostParicio et al (1990) NA 06 mo-15 yr NR 95722Heller/PostPinotti et al (1991) mo Heller/DBonavina et al (1992) Thoracotomy yr HellerMenzies-Gow et al (1978) NA 085 mo4811INR145HellerJara et al (1979) 1%1%NA yr Heller/B or A Okike et al (1979) mo-19 yr IN R 9344Heller/DFYong-xian (1982) yr HellerEllis et al (1984) NA yr968857Heller/BLittle et al (1988)")
28
Laparoscopy 0007 mo069417Heller/DAncona et al (1995) 04012 moINR49625Heller/DRosati et al (1995) 8%1.603 moINR16INR12Heller/DDelgado et al (1996) 00016 mo1789212Heller or Heller/T Swanstrom and Pennings (1994) 07.5012.5 mo510INR40Heller/D or THunter et al (1997) Thoracoscopy 01802 yrINR128822HellerPelligrini et al (1993)
 moINR49625Heller/DRosati et al (1995) 8%1.603 moINR16INR12Heller/DDelgado et al (1996) mo Heller or Heller/T Swanstrom and Pennings (1994) mo510INR40Heller/D or THunter et al (1997) Thoracoscopy yrINR128822HellerPelligrini et al (1993)")
29
Aim of work The aim of this work was to evaluate Heller’s myotomy and preumatic balloon dilatation as two alternative lines of therapy for patients with achalasia of the esophagus.

30
Patients and Methods

31
o Our study is a retrospective non- randomised study conducted at GEC during the period between October 1979- November 2002. o The study included 310 cases with achalasia. o 169 ♂ & 141 ♀ o According to the line of management the study included two groups: Group A: 150 patients treated with myotomy + fundoplication. Group B: 160 patient treated by pneumatic balloon dilatation.

32
Preoperative work up Thorough history and clinical examination. Patients were divided into 4 groups according to Demeester's grading for dysphagia. (Cuschieri et al., 2002) No dysphasia Mild : occasional episodes. Moderate: requires fluids to clear. Severe : episodes of solid food impaction & require medical treatment.
 No dysphasia Mild : occasional episodes. Moderate: requires fluids to clear. Severe : episodes of solid food impaction & require medical treatment..")
33
(continue ) Preoperative work up (continue ) Radiological examination According to Olsen scoring system, patients were divided into 4 groups (Olsen et al., 1983) Endoscopic evaluation Manometric study
 Preoperative work up (continue ) Radiological examination According to Olsen scoring system, patients were divided into 4 groups (Olsen et al., 1983) Endoscopic evaluation Manometric study")
34
Method of management Group (A): Modified Heller myotomy 35 patient (56.8%). Myotomy + Dor fundoplication 45 patient (30%). Myotomy + Nissen fundoplication 9 patient (6%). Myotomy + Taupet fundoplication 4patient (2.6%). Laparoscopic mytomy 3 patients (2%). Laparoscopic mytomy + Dor fundoplication 4patints (2.6%).
. Myotomy + Nissen fundoplication 9 patient (6%). Myotomy + Taupet fundoplication 4patient (2.6%). Laparoscopic mytomy 3 patients (2%). Laparoscopic mytomy + Dor fundoplication 4patints (2.6%)..")
35
Group (B): Pneumatic balloon dilatation (1.8+ 1 set) One session in 79 patients (60.5%). Two sessions in 48 patients (30%). Three or more sessions in only 15 patients (9.5%). Method of management Continue
. Three or more sessions in only 15 patients (9.5%). Method of management Continue.")
38
Results

39
75 patients (24%)MildDysphagia according to Demeester’s grading for dysphagia 186 patients (60%) Moderate 49 patients (16%)Sever 213 patients (69%) Regurgitation 65 patients (21%)Heart burn 220 patients (71%) Weight loss 43 patients (11%)Respiratory complications
MildDysphagia according to Demeester’s grading for dysphagia 186 patients (60%) Moderate 49 patients (16%)Sever 213 patients (69%) Regurgitation 65 patients (21%)Heart burn 220 patients (71%) Weight loss 43 patients (11%)Respiratory complications")
42
Radiological characters of achalasia patients before management. 283 patients (91%)First and second degree. according to Olsen et al 1953 scoring system 27 patients (8.8%)Third and fourth degree. according to Olsen et al 1953 scoring system 279 patients (90%)Delayed evacuation. 9 patients (2.8%)Normal esophagus.
First and second degree. according to Olsen et al 1953 scoring system 27 patients (8.8%)Third and fourth degree. according to Olsen et al 1953 scoring system 279 patients (90%)Delayed evacuation. 9 patients (2.8%)Normal esophagus..")
43
Endoscopic findings in patients with achalasia before management. 273 patients (88%)Dilated esophagus. 36 patients (12%)Marked spastic cardia. 25 patients(8%)Esophagitis. 50 patients (16%)Gastritis and or duodenitis.
Dilated esophagus. 36 patients (12%)Marked spastic cardia. 25 patients(8%)Esophagitis. 50 patients (16%)Gastritis and or duodenitis..")
44
Manometric features for achalasia paients before management

45
Symptomatic evaluation of patients after cardiomyotomy. 105 patients (70%) Complete resolution Dysphagia according to Demeester’s grading for dysphagia 25 patients (16%)Improvement 20 patients (14%)Persistant 37 patients (25%)Heart burn and regurgitation 89 patients (60%)Weight gain
 Complete resolution Dysphagia according to Demeester’s grading for dysphagia 25 patients (16%)Improvement 20 patients (14%)Persistant 37 patients (25%)Heart burn and regurgitation 89 patients (60%)Weight gain.")
46
Symptomatic evaluation of patients after pneumatic ballon dilatation. 96 patients (60%)Complete resolutionDysphagia according to Demeester’s grading for dysphagia 30 patients (19%)Improvement 34 patients (21%)Persistant 24 patients (15%)Heart burn and regurgitation
Complete resolutionDysphagia according to Demeester’s grading for dysphagia 30 patients (19%)Improvement 34 patients (21%)Persistant 24 patients (15%)Heart burn and regurgitation.")
48
AfterBefore Average ValueAverageValue 5 to 19 mmHg 12.9 + 3 mmHg 11 to 95 mmHg 34.5 ±4 mmHg LESP LES 69 to 99 % 80+8 %20to 99%58.5+10 % %RELAXATION 10 to 54 mmHg 24+ 3 mmHg 11to 72% mmHg 24.1+3.5 mmHg PROXAMPLITUDE BODY 10 to 68 mmHg 27+4 mmHg 11to 80% mmHg 23+2 mmHg MID 11 to 65 mmHg 34+2 mmHg 9to 80 mmHg 22.5 1.9± mmHg DISTAL 0.9 to 5.4 sec 3+0.5 Sec 1.5to 10 sec 4.1 ± 2.1 sec PROXDURATION 1.1 to 6.7 sec 3.2+0.3 Sec 1.7 to 10.1 sec 4.1 ± 1sec MID 1 to 6 sec 3.1+1.8 Sec 1.6to 9.8 sec 3.7 ± 1.8 sec DISTAL 9 to 100 % 41+13.2 % 6 to 100 % 55 ± 13.2 % SIMULTANEUSVELOCITY 9 to 100 % 25.1+9 % 6 to 100 % 32.9+9% NON TRANSMITTED Manometric study before and after cardiomyotomy

49
Manometric features before and after pneumatic dilatation.

51
Summary and conclusion

52
We agree that life long palliation of dysphagia is not guaranteed but It is obvious that Heller cardiomyotomy in our study gives good to excellent results as regard the improvement of dysphagia. As in the largest series puplished about the management of achalasia. Pneumatic ballon dilatation is also a good method of management of patients with achalasia, but it doesn’t give the same longterm response as surgical cardiomyotomy besides that some cases may have early recurrence or persistant dysphagia after dilatation.

Similar presentations








 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")






, FACS, FCCP Consultant & Asst. Professor of Cardiothoracic Surgery Consultant.>")








, FRACP. SHAKESPEARE SPECIALIST GROUP MILFORD, AUCKLAND.>")
