Download presentation
Presentation is loading. Please wait.

1
ZARIA THORACIC CLUB MEETING AHMADU BELLO UNIVERSITY TEACHING HOSPITAL,ZARIA,NIGERIA TERATOMA BY DR SANNI,R.O REGISTRAR

3
Introduction Epidemiology Classification Aetiopathogenesis Clinical presentation Investigation treatment conclusion

4
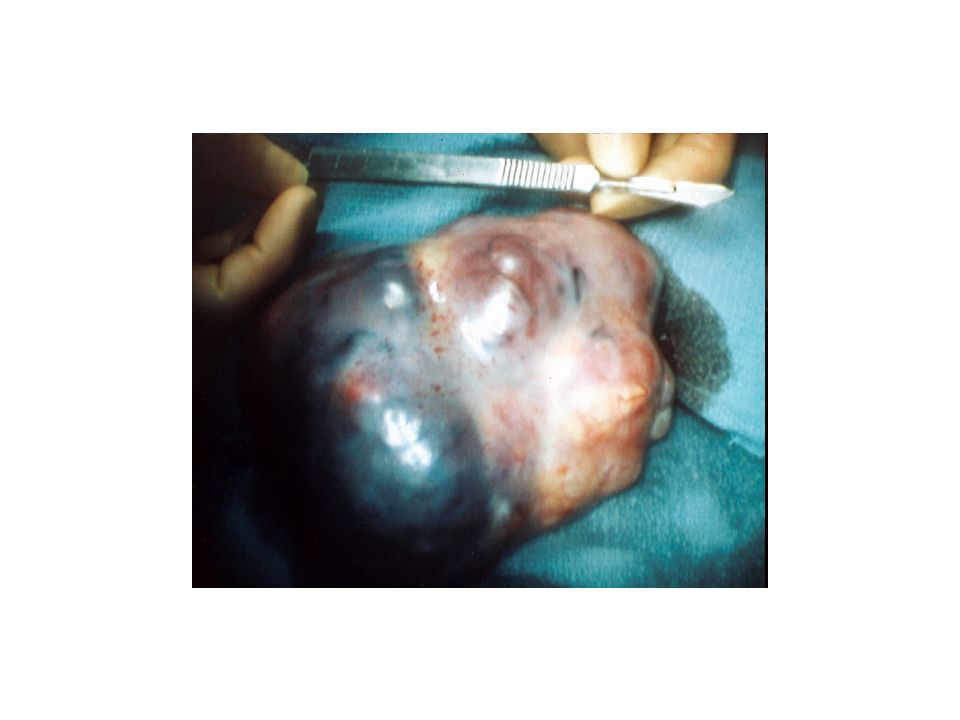
Introduction Terato (Greek : monster, oma : swelling) Teratomas - embronic neaplasm from totipotent stem cells. Component derived from all 3 germ layer. Tissues foreign to the location found. Relatively common solid Neoplasm in children. Gonadal and extragonadal location. Tumor marker

5
Epidermiology SCT most common teratoma. Germ cell tumor-11% childhood tumor,3% malignant. 25% mediastinal tumor malignant. Teratoma Commoner in females. -F:M 4:1 SCT. Affect all age group Increased frequency in the last decade. No significant geographic predilection.

6
Aetiology Gene related Familial tendency Polyunsaturated fat (ovarian) Pyloric stenosis Turner syndrome Klinefelter syndrome
 Pyloric stenosis Turner syndrome Klinefelter syndrome")
7
Aetiopathogenesis Pathology-solid -cystic -mixed -Benign -Malignant

8
Pathogenesis Several theories about its origin. Abnormal differentiation of fetal germ cell that arise from fetal yolk sac Normal migration of cell- gonadal tumor Abnormal to extra gonadal tumor. Typically found in the midline or gonads.

9
Frequency of common sites. Sacroccocygeus40% Ovary25% Testes12% Brain5% Others(neck, mediastinum)18%
18%.")
10
GRADE GradeDescription 00-mature tumor 1immature element in 1 low power field/slide 2<4 field /slide. 3>4 field/slide

11
Correlation between Degree of immaturity and foci of microscopic malignant cell. Charoenkwan et al-over expression of P53 in immature teratoma.

12
Mutter –genetic imprint factor. Osterhuis et al-suggest tumor group based on chromosomal abnormality’. MAGE gene family of tumor rejection antigen involved. Hara et al

13
Mediastinal Teratoma CLINICAL FEATURES Chest pain,retrosternal pain. Cough Dyspnoea Fever Weight loss Fatigue Venous congestion Compressive syptoms Hoarseness, dysphagia, Horners syndrome

14
Clinical presentation Depend on location of tumor. Prenatal diagnosis-SCT,mass, pressure effect. Ovarian mass-abdominal pain,mass distension. Testicular tumor –scrotal mass, pain.

15
Physical examination Chest Cardiovascular Abdominal Rectal examination Identify associated anomalies

16
Investigations Diagnostic Imaging studies- –CXR –CT scan –Ultra sonography – abdomino-pelvic, testicular.

17
Chest X-ray:mediastenal teratoma

18
CT-scan:mediastenal teratoma

19
Tissue Biopsy Mediastinoscopy. Video assisted thoracoscopy, biopsy. Broncoscopy.

20
Serum- AFP -Beta-Hcg Genetic screening.

21
FBC, diff. U E Cr. LFT Pulmonary function test. Others as necessitated by presentation.

22
Treatment Goals –Removal, where possible –Relief of symptoms –Prolongation of life –Improve quality of life. Depends on site, extent of Dx. –Surgical excision. –Chemotherapy

23
Recurrence Risk of recurrence related to degree of maturity. <10% in completely resected mature Teratoma. 33% immature Teratoma. Depends on site and completeness of resection. Decreased by chemotherapy-9.5%(German ). SCT more likely to re occure.
. SCT more likely to re occure..")
24
Follow up Monitor-Examination -AFP -Beta hCG -CXR

25
Prognosis Depend on the organ of origin and extent of the dx.

26
Conclusion The incidence of teratoma is gradually increasing,therefore High index of suspicion is needed for early diagnosis and prompt intervention.

Similar presentations

1 CHILDHOOD LEUKAEMIA. TA OGUNLESI (FWACP)2 LEUKAEMIA Heterogenous group of malignant disorders Characterised by uncontrolled clonal.>")

>")







; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")







