Download presentation
Presentation is loading. Please wait.

1
Treatment of caries: choice of method depending on a clinical case. Remineralizing therapy. Stages of surgical treatment. Features of treatment of deep caries. General and local treatment of plural caries. Medicinal facilities and physical methods in complex therapy of dental caries. Therapeutic dentistry department

2
Types of lesions and choice of treatment ( high caries risk ) Smooth surface incipient caries; Sticky pits and fissures Sticky pits and fissures with incipient caries Small and moderate lesions Deep lesions Root caries
 Smooth surface incipient caries; Sticky pits and fissures Sticky pits and fissures with incipient caries Small and moderate lesions Deep lesions Root caries")
4
Types of lesions and choice of treatment ( high caries risk ) Smooth surface incipient caries: Reminerlize with clinical topical fluoride applications and home application of fluoride by various means ; toothpaste, rinses, brush-on gels, custom tray-applied gels, ect. Reminerlize with clinical topical fluoride applications and home application of fluoride by various means ; toothpaste, rinses, brush-on gels, custom tray-applied gels, ect. Sticky pits and fissures: Pit and fissure sealants Pit and fissure sealants

5
Types of lesions and choice of treatment ( high caries risk ) Sticky pits and fissures with incipient caries Preventive resin/sealants (Remove caries, place composite in the cavity and cover all with sealant) Preventive resin/sealants (Remove caries, place composite in the cavity and cover all with sealant) Definitive amalgam restorations Definitive amalgam restorations Small and moderate lesions Definitive amalgam, composite or glass ionomer restorations Definitive amalgam, composite or glass ionomer restorations
 Sticky pits and fissures with incipient caries Preventive resin/sealants (Remove caries, place composite in the cavity and cover all with sealant) Preventive resin/sealants (Remove caries, place composite in the cavity and cover all with sealant) Definitive amalgam restorations Definitive amalgam restorations Small and moderate lesions Definitive amalgam, composite or glass ionomer restorations Definitive amalgam, composite or glass ionomer restorations")
6
Types of lesions and choice of treatment ( high caries risk ) Deep lesion: Caries control restorations with ZnO- eugenol, glass ionomer or amalgam, and the definitive resotrations after caries activity has decreased Caries control restorations with ZnO- eugenol, glass ionomer or amalgam, and the definitive resotrations after caries activity has decreased Root caries: Fluoride applications Fluoride applications Glass ionomer restoration Glass ionomer restoration
 Deep lesion: Caries control restorations with ZnO- eugenol, glass ionomer or amalgam, and the definitive resotrations after caries activity has decreased Caries control restorations with ZnO- eugenol, glass ionomer or amalgam, and the definitive resotrations after caries activity has decreased Root caries: Fluoride applications Fluoride applications Glass ionomer restoration Glass ionomer restoration")
7
Patients (especially the elderly) with root caries. Patients that report a history of a physical condition, medical treatment (especially radiation therapy), medication and dietary changes that would influence saliva or oral flora History of continued high quantity intake of carbonated beverages
, medication and dietary changes that would influence saliva or oral flora History of continued high quantity intake of carbonated beverages.")
8
Patients with active caries-lesions that are unpigmented, of a soft consistency, moist, sensitive to Sweets, cold or excarvation, and with depth greater than width.

9
DXACTIVEINACTIVE COLORLIGHTDARK CONSISTENCYMUSHYFIRM MOISTUREWETDRY SYMPTOMSENSITIVENONE SHAPEDEPTH>WIDTHWIDTH>DEPTH

10
Caries Control Restoration Indirect pulp capping is often done in conjunction with caries control restorations. Pulp must show radiographic and clinical signs and symptoms of vitality. Pulp must show radiographic and clinical signs and symptoms of vitality. All caries is removed at the periphery, establishing a sound DEJ. All caries is removed at the periphery, establishing a sound DEJ.

11
Caries Control Restoration

12
Indirect pulp capping is often done in conjunction with caries control restorations. After 6-8 weeks the entire restoration is removed, any remaining caries is removed and a definitive restoration is planned. After 6-8 weeks the entire restoration is removed, any remaining caries is removed and a definitive restoration is planned.

13
Pit & Fissure Sealing Techniques

14
Glass ionomer sealants Chemical bond to enamel. Fluoride release. New GIC material- Fuji 7 high fluoride release (6 x more) than other restorative GICs. has good flow properties and flow well into pits/fissures. moisture tolerant. has a strong fused layer which is acid resistant & continues to offer protection to occlusal surface even when it appears “visually” lost due to wear. Restorative GICs tend not to be suited as fissure sealants as are thicker and do not flow well into narrow/deep pits & fissures
 than other restorative GICs. has good flow properties and flow well into pits/fissures. moisture tolerant. has a strong fused layer which is acid resistant & continues to offer protection to occlusal surface even when it appears visually lost due to wear. Restorative GICs tend not to be suited as fissure sealants as are thicker and do not flow well into narrow/deep pits & fissures.")
15
Glass ionomer sealants

16
Diagnosis of pit/fissure caries Diagnosis of pit/fissure caries - can be very difficult! 3 Possibilities: 1. No caries 2. Definite caries 3. Questionable caries

17
Is there caries or is this only stain?

18
Management of Questionable pit/fissure early caries Monitor tooth surface over period of time in conjunction with other caries preventive measures. Mechanically open up fissures with a bur/air abrasion and check if carious (invasive?) Fissure seal with fissure sealant.
 Fissure seal with fissure sealant..")
19
Fissure exploration Bur tip should be as fine as possible. L 10L 20

20
Fissure exploration Place bur in central fossa of occlusal fissure.

21
Depth is determined by: depth of staining present what is required to alter the anatomy of the fissure so that the sealant can flow to its full depth (approx 0.5mm). Avoid cuspal inclines. Note that the depth may therefore vary. Upright bur so that it is in the long axis of the tooth; however, bur can be leant towards the ‘direction of travel’ movement, away from the tip.

22
Demonstrates initial investigation to distal part of occlusal fissure system

23
Initial investigation into complete fissure system

24
Completed fissure investigation 1. Wash (5 seconds) 2. Dry with mild air (10 seconds)
 2. Dry with mild air (10 seconds)")
25
Completed fissure investigation (cont.) Visually check the prepared fissure system: Any staining? Is it clean? (Note that the depth may vary.)
.")
26
Fissure sealant materials Select appropriate material to complete the fissure sealant. You can use: resin system Glass Ionomer Cement Resin Modified Glass Ionomer Cement (RMGIC

27
Application of etchant Apply etchant to fissure system for 15 seconds.

28
Wash thoroughly for minimum 20 seconds to remove etchant.

29
Note that natural tooth should have a frosty appearance. Dry thoroughly.

30
Applying sealant Step 1 Spread sealant evenly. One can use applicator or micro-brush, or sealant can be applied directly to surface. Avoid porosity (bubbles). (DO NOT blow air to spread the sealant.)
. (DO NOT blow air to spread the sealant.).")
31
Applying sealant Step 2 Note that the occlusal fissure system is completely covered with resin material but does not extend up to the cusps.

32
Light cure resin material for 20 seconds.

33
Checking the sealant Using explorer: ensure material is completely cured check margins ensure material is bonded to enamel.

34
Composite resin finishing point STEPS IN FINISHING A COMPOSITE RESINS 1.Reduction of the material is completed by the use of a white stone or a finishing diamond. 2.Fine finishing is done with carbide finishing burs, then with diamond burs. 3.Polishing the resin begins with the medium discs and finishing with the superfine discs. 4.Finishing strips assist in the polishing of the interproximal surfaces. 5.Polishing paste applied to a rubber cup completes the step.

35
Treatment of dental caries by: AMALGAM. Properties, indications, inserting, carving, polishing.

36
Composition The composition of the alloy powder particles varies from one product to another. Composition of CONVENTIONAL AMALGAM ALLOY:

37
Effects on properties of an amalgam restoration imparted by ingredients. PROPERTYINGREDIENT SilverTinCopperZinc StrengthIncreases DurabilityIncreases Hardness Increases ExpansionIncreasesDecreasesIncreases FlowDecreasesIncreasesDecreases ColorImparts Setting timeDecreasesIncreasesDecreases Workability Increases Cleanliness Increases

38
TRITURATION The advantages of mechanical trituration are as follows: 1. A uniform and reproducible mix is produced. 2. A shorter trituration time can be used. 3. A greater alloy/mercury ratio can be used. Amalgamator

39
3. CONDENSATION There should be a minimal time delay between trituration and condensation. If condensation is commended too late, the amalgam will have achieved a certain degree of set and adaptation, and final mechanical properties are all affected. There is a good correlation between the quality of an AM restoration and the energy expended by the operator who condenses it. It needs to use a high condensating force. Lower forces are required to condense spherical particle amalgams than lathe-cut materials.

40
Condensing instruments Amalgam carriers and condensers are used for this purpose.

41
4. CARVING Soon after condensing the AM, the surface layer, which is rich in mercury, is carved away with a sharp instrument. If carving is delayed too long the material may become too hard to carve and there is a danger of chipping at the margins.

42
4. CARVING Amalgam carvers

43
5. POLISHING Polishing is carried out in order to achieve a lustrous surface having a more acceptable appearance and better corrosion resistance. The fillings should not be polished untill the material has achieved a certain level of mechanical strength, otherwisw there is a danger of fracture, particularly at the margins. Many products require a delay of 24 hours between placing and polishing.

44
5. POLISHING Polishing kits

45
Polishers Black Dark purple Green

46
Amalgam indications In primary and permanent dentition In stress bearing areas of the mouth In stress bearing areas of the mouth When moisture control is a problem When moisture control is a problem When oral hygiene is bad When oral hygiene is bad As a foundation to crowns As a foundation to crowns When cost is a concern Small to moderate – sized cavities in the posterior teeth Small to moderate – sized cavities in the posterior teeth

47
Amalgam contraindications When esthetics is important When patient has a history of allergic reactions to the alloy When cost is not a concern

48
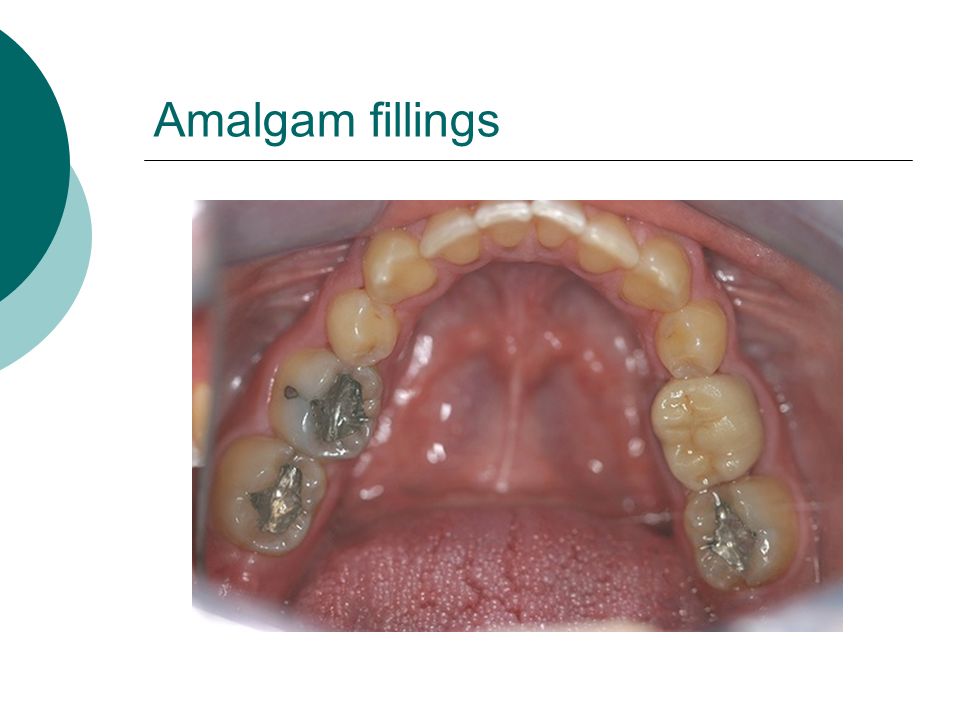
Amalgam fillings

50
Thank you for attention!

Similar presentations

















. All rights reserved. No part of this product may be reproduced or transmitted in any.>")


