Download presentation
Presentation is loading. Please wait.

1
DEEP VENOUS THROMBOSIS
DR.SHERAZ AHMED

2
Definition Deep vein thrombosis is the formation of a blood clot in one of the deep veins of the body, usually in the leg

3
ETIOLOGY DVT ususally originates in the lower extremity venous level ,starting at the calf vein level and progressing proximally to involve popliteal ,femoral ,or iliac system % pulmonary emboli originates here .

4
Virchow tried More than 100 years ago, Virchow described a triad of factors of venous stasis, endothelial damage, and hypercoagulable state

5
Venous stasis prolonged bed rest (4 days or more) A cast on the leg
Limb paralysis from stroke or spinal cord injury extended travel in a vehicle

6
Hypercoagulability Surgery and trauma responsible for up to 40% of all thromboembolic disease Malignancy Increased estrogen (due to a fall in protein ‘S) Increased estrogen occurs during all stages of pregnancy— the first three months postpartum, after elective abortion, and during treatment with oral contraceptive pills
 Increased estrogen occurs during. all stages of pregnancy— the first three months postpartum, after elective abortion, and. during treatment with oral contraceptive pills.")
7
Inherited disorders of coagulation
deficiencies of protein ‘S, ’ protein ‘C,’ and antithrombin III.

8
Acquired disorders of coagulation
nephrotic syndrome results in urinary loss of antithrombin III, this diagnosis should be considered in children presenting with thromboembolic disease Antiphospholipid antibodies accelerate coagulation and include the lupus anticoagulant and anticardiolipin antibodies.

9
Inflammatory processes, such as systemic lupus erythematosus (SLE),
sickle cell disease, and inflammatory bowel disease (IBD), also predispose to thrombosis, presumably due to hypercoagulability
, also predispose to thrombosis, presumably due to hypercoagulability.")
10
Endothelial Injury Trauma, surgery, and
invasive procedure may disrupt venous integrity Iatrogenic causes of venous thrombosis are increasing due to the widespread use of central venous catheters, particularly subclavian and internal jugular lines. These lines are an important cause of upper extremity DVT, particularly in children.

11
Clinical Pathophysiology
The nidus for a clot is often an intimal defect When a clot forms on an intimal defect, the coagulation cascade promotes clot growth proximally. Thrombus can extend from the superficial veins into the deep system from which it can embolize to the lungs.

12
Opposing the coagulation cascade is the endogenous fibrinolytic system
Opposing the coagulation cascade is the endogenous fibrinolytic system. After the clot organizes or dissolves, most veins will recanalize in several weeks. Residual clots retract as fibroblasts and capillary development lead to intimal thickening. Venous hypertension and residual clot may destroy valves, leading to the postphlebitic syndrome, which develops within 5-10 years

13
Edema, sclerosis, and ulceration characterize this syndrome, which develops in 40-80% of patients with DVT. patients also can suffer exacerbations of swelling and pain, probably as a result of venous dilatation and hypertension Pulmonary embolism (PE) is a serious complication of DVT. Many episodes of pulmonary embolism go unrecognized, and at least 40% of patients with DVT have clinically silent PE on VQ scanning
 is a serious complication of DVT. Many episodes of pulmonary embolism go unrecognized, and at least 40% of patients with DVT have clinically silent PE on VQ scanning.")
14
Presentation and Physical Examination
Calf pain or tenderness, or both Swelling with pitting oedema Swelling below knee in distal deep vein thrombosis and up to groin in proximal deep vein thrombosis Increased skin temperature Superficial venous dilatation Cyanosis can occur with severe obstruction

15
Palpate distal pulses and evaluate capillary refill to assess limb perfusion.
Move and palpate all joints to detect acute arthritis or other joint pathology. Neurologic evaluation may detect nerve root irritation; sensory, motor, and reflex deficits should be noted Homans'’ sign: pain in the posterior calf or knee with forced dorsiflexion of the foot

16
Search for stigmata of PE such as tachycardia (common), tachypnea or chest findings (rare), and
exam for signs suggestive of underlying predisposing factors.

18
Wells Clinical Prediction Guide
The Wells clinical prediction guide incorporates risk factors, clinical signs, and the presence or absence of alternative diagnoses . Wells Clinical Prediction Guide for DVTClinical ParameterScore Active cancer (treatment ongoing, or within 6 months or palliative)1 Paralysis or recent plaster immobilization 1 Recently bedridden for >3 days or major surgery <4 weeks1
1. Paralysis or recent plaster immobilization 1. Recently bedridden for >3 days or major surgery <4 weeks1.")
19
Localized tenderness along the distribution of the deep venous system1
Entire leg swelling1 Calf swelling >3 cm compared to the asymptomatic leg 1 Pitting edema (greater in the symptomatic leg)1 Collateral superficial veins (nonvaricose)1 Alternative diagnosis (as likely or > that of DVT)
1. Collateral superficial veins (nonvaricose)1. Alternative diagnosis (as likely or > that of DVT)")
20
Total of Above Score High probability: Score ³3 Moderate probability: Score = 1 or 2 Low probability: Score £0 Adapted from Anand SS, et al. JAMA. 1998; 279 [14];1094

21
Diagnostic Studies Clinical examination alone is able to confirm only 20-30% of cases of DVT Blood Tests the D-dimer INR. Current D-dimer assays have predictive value for DVT, and the INR is useful for guiding the management of patients with known DVT who are on warfarin (Coumadin)
")
22
D-dimer D-dimer is a specific degradation product of cross-linked fibrin. Because concurrent production and breakdown of clot characterize thrombosis, patients with thromboembolic disease have elevated levels of D-dimer three major approaches for measuring D-dimer ELISA latex agglutination blood agglutination test (SimpliRED

23
False-positive D-dimers occur in patients with
recent (within 10 days) surgery or trauma, recent myocardial infarction or stroke, acute infection, disseminated intravascular coagulation, pregnancy or recent delivery, active collagen vascular disease, or metastatic cancer
 surgery or trauma, recent myocardial infarction or stroke, acute infection, disseminated intravascular coagulation, pregnancy or recent delivery, active collagen vascular disease, or metastatic cancer.")
24
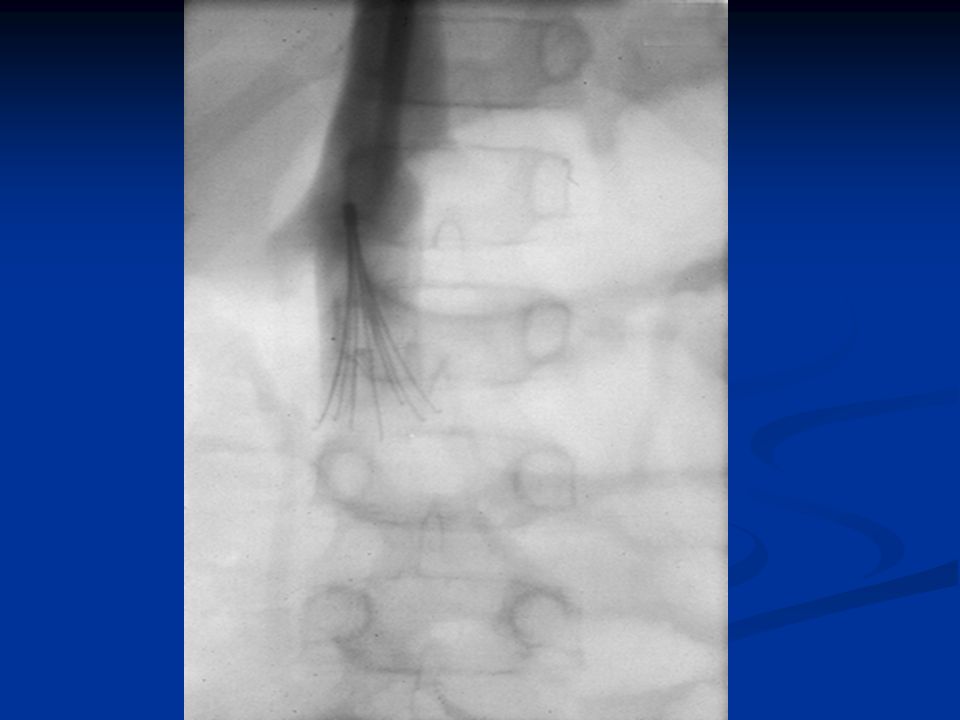
Imaging Studies Invasive venography, radiolabeled fibrinogen and.
noninvasive ultrasound, plethysmography, MRI techniques

25
venography gold standard” modality for the diagnosis of DVT Advantages
Venography is also useful if the patient has a high clinical probability of thrombosis and a negative ultrasound, it is also valuable in symptomatic patients with a history of prior thrombosis in whom the ultrasound is non-diagnostic.

26
side effects phlebitis anaphylaxis

28
Nuclear Medicine Studies
Because the radioactive isotope incorporates into a growing thrombus, this test can distinguish new clot from an old clot

29
Plethysmography Plethysmography measures change in lower extremity volume in response to certain stimuli.

30
Ultrasonography color-flow Duplex scanning is the imaging test of choice for patients with suspected DVT inexpensive, noninvasive, widely available Ultrasound can also distinguish other causes of leg swelling, such as tumor, popliteal cyst, abscess, aneurysm, or hematoma.

31
clinical limitations expensive reader dependent
Duplex scans are less likely to detect non-occluding thrombi. During the second half of pregnancy, ultrasound becomes less specific, because the gravid uterus compresses the inferior vena cava, thereby changing Doppler flow in the lower extremities

32
Magnetic Resonance Imaging
It detects leg, pelvis, and pulmonary thrombi and is 97% sensitive and 95% specific for DVT. It distinguishes a mature from an immature clot. MRI is safe in all stages of pregnancy.

33
DIFFERENTIAL DIAGNOSIS
Cellulitis Thrombophlebitis Arthritis Asymmetric peripheral edema secondary to CHF, liver disease, renal failure, or nephrotic syndrome lymphangitis Extrinsic compression of iliac vein secondary to tumor, hematoma, or abscess Hematoma Lymphedema

34
Muscle or soft tissue injury Neurogenic pain Postphlebitic syndrome Prolonged immobilization or limb paralysis Ruptured Baker cyst Stress fractures or other bony lesions Superficial thrombophlebitis Varicose veins

35
Management Using the pretest probability score calculated from the Wells Clinical Prediction rule, patients are stratified into 3 risk groups—high, moderate, or low. The results from duplex ultrasound are incorporated as follows: If the patient is high or moderate risk and the duplex ultrasound study is positive, treat for DVT.

36
If the duplex study is negative and the patient is low risk, DVT has been ruled out.
When discordance exists between the pretest probability and the duplex study result, further evaluation is required. If the patient is high risk but the ultrasound study was negative, the patient still has a significant probability of DVT

37
a venogram to rule out a calf vein DVT
surveillance with repeat clinical evaluation and ultrasound in 1 week. results of a D-dimer assay to guide management If the patient is low risk but the ultrasound study is positive, some authors recommend a second confirmatory study such as a venogram before treating for DVT

38
EMERGENCY DEPARTMANT CARE
The primary objectives of the treatment of DVT are to prevent pulmonary embolism, reduce morbidity, and prevent or minimize the risk of developing the postphlebitic syndrome.

39
Anticoagulation Thrombolytic therapy for DVT Surgery for DVT Filters for DVT Compression stockings

40
Anticoagulation Heparin prevents extension of the thrombus
Heparin's anticoagulant effect is related directly to its activation of antithrombin III. Antithrombin III, the body's primary anticoagulant, inactivates thrombin and inhibits the activity of activated factor X in the coagulation process.

41
Heparin is a heterogeneous mixture of polysaccharide fragments with varying molecular weights but with similar biological activity. The larger fragments primarily interact with antithrombin III to inhibit thrombin. The low molecular weight fragments exert their anticoagulant effect by inhibiting the activity of activated factor X. The hemorrhagic complications attributed to heparin are thought to arise from the larger higher molecular weight fragments.

42
The optimal regimen for the treatment of DVT is anticoagulation with heparin or an LMWH followed by full anticoagulation with oral warfarin for 3-6 months Warfarin therapy is overlapped with heparin for 4-5 days until the INR is therapeutically elevated to between 2-3.

43
After an initial bolus of 80 U/kg, a constant maintenance infusion of 18 U/kg is initiated. The aPTT is checked 6 hours after the bolus and adjusted accordingly. . The aPTT is repeated every 6 hours until 2 successive aPTTs are therapeutic. Thereafter, the aPTT is monitored every 24 hours as well as the hematocrit and platelet count.

44
Advantages of Low-Molecular-Weight Heparin Over Standard Unfractionated Heparin
Superior bioavailability Superior or equivalent safety and efficacy Subcutaneous once- or twice-daily dosing No laboratory monitoring* Less phlebotomy (no monitoring/no intravenous line) Less thrombocytopenia Earlier/facilitated
 Less thrombocytopenia. Earlier/facilitated.")
45
At the present time, 3 LMWH preparations,
Enoxaparin, Dalteparin, and Ardeparin

46
warfarin Interferes with hepatic synthesis of vitamin K-dependent coagulation factors Dose must be individualized and adjusted to maintain INR between 2-3 2-10 mg/d PO caution in active tuberculosis or diabetes; patients with protein C or S deficiency are at risk of developing skin necrosis

47
Thrombolytic therapy for DVT
Advantages include prompt resolution of symptoms, prevention of pulmonary embolism, restoration of normal venous circulation, preservation of venous valvular function, and prevention of postphlebitic syndrome.

48
Thrombolytic therapy does not prevent
clot propagation, rethrombosis, or subsequent embolization. Heparin therapy and oral anticoagulant therapy always must follow a course of thrombolysis.

49
Thrombolytic therapy is also not effective once the thrombus is adherent and begins to organize
The hemorrhagic complications of thrombolytic therapy are formidable (about 3 times higher), including the small but potentially fatal risk of intracerebral hemorrhage. The uncertainty regarding thrombolytic therapy likely will continue
, including the small but potentially fatal risk of intracerebral hemorrhage. The uncertainty regarding thrombolytic therapy likely will continue.")
50
Surgery for DVT indications when anticoagulant therapy is ineffective
unsafe, contraindicated. The major surgical procedures for DVT are clot removal and partial interruption of the inferior vena cava to prevent pulmonary embolism.

51
These pulmonary emboli removed at autopsy look like casts of the deep veins of the leg where they originated.

52
This patient underwent a thrombectomy
This patient underwent a thrombectomy. The thrombus has been laid over the approximate location in the leg veins where it developed.

53
Filters for DVT Indications for insertion of an inferior vena cava filter Pulmonary embolism with contraindication to anticoagulation Recurrent pulmonary embolism despite adequate anticoagulation

54
Controversial indications:
Deep vein thrombosis with contraindication to anticoagulation Deep vein thrombosis in patients with pre-existing pulmonary hypertension Free floating thrombus in proximal vein Failure of existing filter device Post pulmonary embolectomy

55
Inferior vena cava filters reduce the rate of pulmonary embolism but have no effect on the other complications of deep vein thrombosis. Thrombolysis should be considered in patients with major proximal vein thrombosis and threatened venous infarction

57
Compression stockings (routinely recommended

58
Further Inpatient Care
Most patients with confirmed proximal vein DVT may be treated safely on an outpatient basis. Exclusion criteria for outpatient management are as follows: Suspected or proven concomitant pulmonary embolism Significant cardiovascular or pulmonary comorbidity Morbid obesity Renal failure Unavailable or unable to arrange close follow-up care

59
Patients are treated with a low molecular weight heparin and instructed to initiate therapy with warfarin 5 mg PO the next day. Low molecular weight heparin and warfarin are overlapped for about 5 days until the international normalized ratio (INR) is therapeutic. If inpatient treatment is necessary, low molecular weight heparin is effective and obviates the need for IV infusions or serial monitoring of the PTT. With the introduction of low molecular weight heparin, selected patients qualify for outpatient treatment only if adequate home care and close medical follow-up care can be arranged.

60
Platelets also should be monitored and heparin discontinued if platelets fall below 75,000.
While on warfarin, the prothrombin time (PT) must be monitored daily until target achieved, then weekly for several weeks. When the patient is stable, monitor monthly. Significant bleeding (ie, hematemesis, hematuria, gastrointestinal hemorrhage) should be investigated thoroughly since anticoagulant therapy may unmask a preexisting disease (eg, cancer, peptic ulcer disease, arteriovenous malformation).
 must be monitored daily until target achieved, then weekly for several weeks. When the patient is stable, monitor monthly. Significant bleeding (ie, hematemesis, hematuria, gastrointestinal hemorrhage) should be investigated thoroughly since anticoagulant therapy may unmask a preexisting disease (eg, cancer, peptic ulcer disease, arteriovenous malformation).")
61
Duration of anticoagulation in patients with deep vein thrombosis
Transient cause and no other risk factors: 3 months Idiopathic: 3-6 months Ongoing risk for example, malignancy: 6 -12 months Recurrent pulmonary embolism or deep vein thrombosis: 6-12 months Patients with high risk of recurrent thrombosis exceeding risk of anticoagulation: indefinite duration (subject to review)
")
62
Further Outpatient Care:
Patients with suspected or diagnosed isolated calf vein DVT may be discharged safely on a nonsteroidal anti-inflammatory drug (NSAID) or aspirin with close follow-up care and repeat diagnostic studies in 3-7 days to detect proximal extension. At certain centers, patients with isolated calf vein DVT are admitted for full anticoagulant therapy.
 or aspirin with close follow-up care and repeat diagnostic studies in 3-7 days to detect proximal extension. At certain centers, patients with isolated calf vein DVT are admitted for full anticoagulant therapy.")
63
Patients with suspected DVT but negative noninvasive studies need to be reassessed by their primary care provider within 3-7 days. Patients with ongoing risk factors may need to be restudied at that time to detect proximal extension because of the limited accuracy of noninvasive tests for calf vein DVT.

64
Complications Acute pulmonary embolism Hemorrhagic complications
Chronic venous insufficiency

65
Prognosis: All patients with proximal vein DVT are at long-term risk of developing chronic venous insufficiency. About 20% of untreated proximal (above the calf) DVTs progress to pulmonary emboli, and 10-20% of these are fatal. With aggressive anticoagulant therapy, the mortality is decreased 5- to 10-fold. DVT confined to the calf virtually never causes clinically significant emboli and thus does not require anticoagulation
 DVTs progress to pulmonary emboli, and 10-20% of these are fatal. With aggressive anticoagulant therapy, the mortality is decreased 5- to 10-fold. DVT confined to the calf virtually never causes clinically significant emboli and thus does not require anticoagulation.")
66
Patient Education: Advise women taking estrogen of the risks and common symptoms of thromboembolic disease. Discourage prolonged immobility, particularly on plane rides and long car trips

67
PROPHYLAXIS Ideidentify any patiant who is at risk.
Prevent dehydration. During operation avoid prolonged calf compression. Passive leg exercises should be encourged whilst patient on bed. Foot of bed should be elevated to increase venous return. Early mobilization should be rule for all surgical patients.

Similar presentations









 in a deep vein, usually in the legs, which partially or completely.>")

 around valves propagation Virchow’s triad.>")





 (Venous Thromboembolism) Presented by Maribeth Desiongco MA, RN-BC 2008.>")



