Download presentation
Presentation is loading. Please wait.

1
St Luke’s Symposium November 2010 National Clinical Programmes Dr Barry White Director of Quality & Clinical Care HSE 1

2
St Luke’s Symposium November 2010 How does the Directorate link to other HSE Management functions? The Directorate of Quality and clinical care is one of a number of integrated HSE management trams design to deliver an efficient and effective patient centric Health Service 2 PLAN IMPROVE Define the way clinical services should be delivered, resourced & measured Objective Leadership responsibility Co-ordinate the development of Service Plan Management Plans Mange the allocation of resources Identification of service improvement solutions Corporate Planning & Control Processes Directorate (CPCP) Quality & Clinical Care Directorate (DQCC) Integrated Services Division (ISD) Tactical – ISD Strategic – DQCC Operational – Infrastructure Monitor & report performance against targets and plans Monitor – ISD Report – CPCP Key Management processes Enabling management processes Human Resource Management Financial Management Infrastructure & IT Management Communications DEFINE MANAGE MONITOR & REPORT
 Quality & Clinical Care Directorate (DQCC) Integrated Services Division (ISD) Tactical – ISD Strategic – DQCC Operational – Infrastructure Monitor & report performance against targets and plans Monitor – ISD Report – CPCP Key Management processes Enabling management processes Human Resource Management Financial Management Infrastructure & IT Management Communications DEFINE MANAGE MONITOR & REPORT.")
3
St Luke’s Symposium November 2010 3 Mission Better care and better use of resources

4
St Luke’s Symposium November 2010 3 key issues Clinical leadership for subject matter expertise and credibility (public and clinical) Standardised care (save lives and saves money) Programmatic approach 4
 Standardised care (save lives and saves money) Programmatic approach 4")
5
St Luke’s Symposium November 2010 5 What is the mission of the Directorate of Quality & Clinical Care? Better care and better use of resources If patients get the right treatment we can save lives and money 70% of healthcare spend is on 6 chronic diseases (with 80% of this on patients with >3 chronic diseases) 70% of deaths are associated with these chronic diseases Chronic disease management is delivered in an unstructured manner and 50% of patients do not receive the right treatment If patients received the right treatment this would save 25%-40% of healthcare spend E.g. Stroke in Ireland Sustainable healthcare improvements are clinically led (KP, Finland Asthma etc) A structured and clinically led approach to chronic disease management will improve outcomes and save money
 70% of deaths are associated with these chronic diseases Chronic disease management is delivered in an unstructured manner and 50% of patients do not receive the right treatment If patients received the right treatment this would save 25%-40% of healthcare spend E.g. Stroke in Ireland Sustainable healthcare improvements are clinically led (KP, Finland Asthma etc) A structured and clinically led approach to chronic disease management will improve outcomes and save money.")
6
St Luke’s Symposium November 2010 6 Why take a programmatic approach to change? The advantages of developing chronic disease management programs are: – Structured approach to disease management to ensure patients gets the right treatment – Change is led by experienced clinicians with expertise in disease and service delivery. – Generates clinical buy-in and ownership from the start. Also provides opportunity for bottom-up and top down change by engaging Colleges and professional bodies. – Enables greater organisational responsiveness i.e. frontline staff can access the top of the organisation in one step via the national lead. – Provides a sustained focus – The appointment of Prof. Keane as the Director of the National Cancer Control Programme (NCCP), demonstrates the importance of having an expert in the relevant clinical area to engage with evidence to the public, media, politicians and other clinicians.
, demonstrates the importance of having an expert in the relevant clinical area to engage with evidence to the public, media, politicians and other clinicians..")
7
St Luke’s Symposium November 2010

8
8 Overall principles Set goals that achieve gains in cost, quality, access and compliance Set goals that are simple and meaningful – e.g. prevent 300 stroke deaths Target what is achievable Target areas that can sustainable short term gains Nationalise existing local good practice - do not reinvent the wheel Ensure local ownership (authority, accountability and responsibility) Ensure patient involvement Embed data at the centre of all assessments and decisions Detailed implementation and communication plans
 Ensure patient involvement Embed data at the centre of all assessments and decisions Detailed implementation and communication plans.")
9
St Luke’s Symposium November 2010 9 What are the stages of the standardised approach to managing change? Initiate program Scope the program Set Goals Measure & analyse performance Validate solutions Detailed solution design Implement solutions Sustain & improve performance 12345678 1 2 3 4 Define key issues & solutions Checkpoints with the Program Advisory Group, the Director of Quality & Clinical Care and Steering group

10
St Luke’s Symposium November 2010 10 Programs & leads Medication Management - PM Mairead Gleeson 4. Acute Hospital Services To be appointed Paediatrics Rehab

11
St Luke’s Symposium November 2010 11 Overall principles 1.Clinician led change supported by multidisciplinary teams 2.Patient involvement 3.Programmatic approach focused on implementation 4.Set quality, access & cost goals that are meaningful – e.g. prevent 300 stroke deaths 5.Nationalise existing local best practice 6.Ensure local ownership How success will be assessed : 5% of marks for the solution 95% for successful implementation

12
St Luke’s Symposium November 2010

15
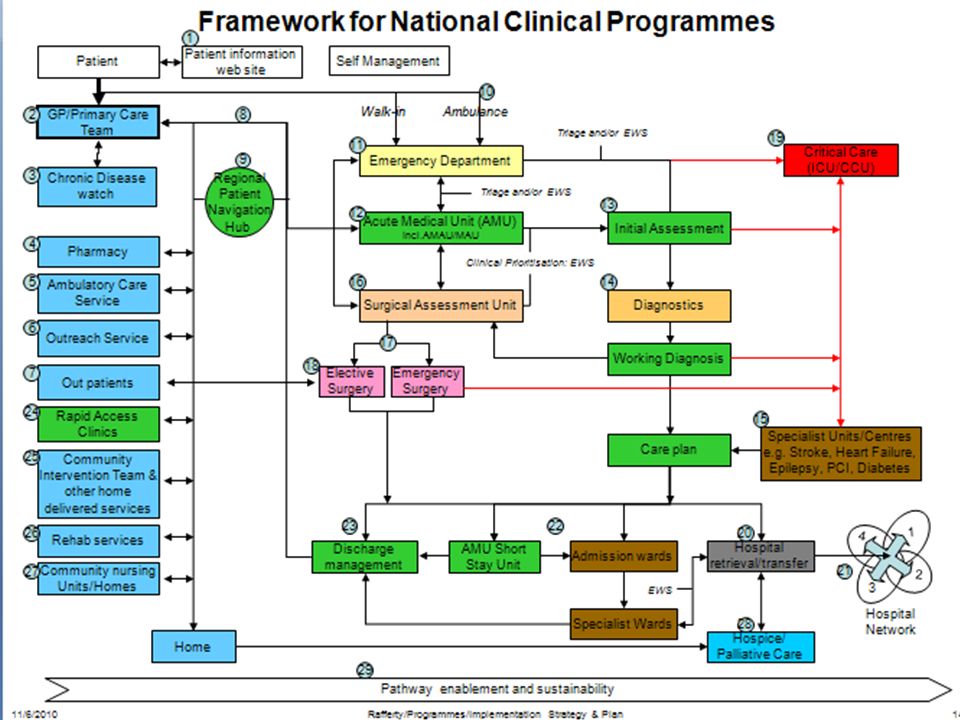
Key Acute Medicine features of the Blue Print Acute Medical Units, Acute Medical Assessment Units and Medical Assessment Units New working practices/continuous presence National Early Warning Score Rapid access to out-patients Navigation hub/bed bureau and Case Manager Retrieval service Hospital models Metrics New approach to education, training and development 15

16
St Luke’s Symposium November 2010

17
17 Key Achievements of Programmes to date 1.Establish programme teams, governance structures and objectives 2.Detailed solution design phase for Heart failure, COPD, epilepsy, Diabetes, Asthma, Stroke and Acute Medicine 3.Guidelines, Bundles, Models of care complete for above 4.Design complete and implementation commenced neurology and dermatology OPD 5.Agreement of Avlos / Day of Surgery & Day Surgery Rates – Roll out 2011 6.Productive theatre – 5 Sites commenced 7.Surgical and Critical Care Audit implementation planning underway 8.Patient information website – 2011 9.Blue print for the future

18
St Luke’s Symposium November 2010 Heart Failure Prevent 2000 heart failure exacerbations requiring admission per year Every appropriate patient admitted to hospital with heart failure has access to structured heart failure programme Save 200 beds per year ROI 3:1 in 3 years Investment involves redeployment of existing nursing staff 18

19
St Luke’s Symposium November 2010 Epilepsy Convert 8000 patients to being seizure free Save one life per week All patients have access to structured epilepsy programme Save 60 beds ROI 3:1 in 3 yrs Investment requires redeployment of existing staff 19

20
St Luke’s Symposium November 2010 20 Summary Major change in clinical leadership and role of Colleges has been implemented Programmes rapidly progressing Solutions identified Excellent clinical engagement (doctors, nurses, and Therapists) Wide stakeholder buy in (Colleges, Nursing, Therapists, HSE SMT, HSE Board, DOHC, Patient groups, Unions) Integration underway into single plan Major financial cutbacks underway Increasing need for radical change which needs to be clinician led Enough talking – time for action
 Wide stakeholder buy in (Colleges, Nursing, Therapists, HSE SMT, HSE Board, DOHC, Patient groups, Unions) Integration underway into single plan Major financial cutbacks underway Increasing need for radical change which needs to be clinician led Enough talking – time for action")
Similar presentations







>")



, the Irish Association of Directors of Nursing.>")







