Download presentation
Presentation is loading. Please wait.

1
Testicular Descent and Ascent: A Matter of Timing
Yegappan Lakshmanan, MD, FAAP Pediatric Urology Children’s Hospital of Michigan

2
Disclosures None

3
Why do testes descend? 2 to 3 degree F difference in temperature needed for spermatogenesis Only in primates do testes descend at or near birth (hibernating animals descend only during breeding season, whales cooled by water, birds by air during flight)
")
5
Testicular Descent: Why the fuss?
A fused scrotum with 2 descended testes is better than any genetic or hormonal test for “manhood” Porphyry Chair - “La Sedia Gestatoria” Middle Ages: (Paschal II) and 1513 (Leo X)
 and 1513 (Leo X)")
6
“duo testes bene pendulum” (‘he has 2 testes and they hang well’)
")
7
Terminology Cryptorchidism vs Undescended Testis Retractile testis
In and out of scrotum but returns to a dependent scrotal position Ascended testis (acquired) Documented scrotal position after birth but subsequently not in scrotum
 Documented scrotal position after birth but subsequently not in scrotum.")
8
Objectives Testicular Descent Current perspectives in treating UDT
Timing of orchidopexy Bianchi or scrotal approach Nubbins Testicular Ascent Extravaginal torsion

9
Testicular Descent: Trans-abdominal phase
Gubernaculum – swelling reaction Cranial suspensory ligament regression Insl3 from Leydig cells + MIS /DHT Few mutations of Insl3 / Lgr8 described in patients Klonisch et al, Dev Bio, 270:1-18, 2004; Hutson et al, J Ped Surg, 40: , 2005

10
Testicular Descent: Inguinoscrotal Phase
Androgen dependent Deficiency of this phase with retention of CSL in: LuRKO (LH receptor knockout) Natural hpg mouse Natural tfm mouse Androgens do not suppress CSL in male bats Klonisch et al, Dev Bio, 270:1-18, 2004; Hutson et al, J Ped Surg, 40: , 2005
 Natural hpg mouse. Natural tfm mouse. Androgens do not suppress CSL in male bats. Klonisch et al, Dev Bio, 270:1-18, 2004; Hutson et al, J Ped Surg, 40: ,")
11
Epidemiology Most frequent anomaly of the male GU system
No predilection for race or geographic location Mostly sporadic but may be associated with genetic disorders

12
Undescended Testis: Incidence
Newborn:3 to 5% (Full-term, >2500 gm) At 1 year:0.8 to 1% (after 6 months) Adults:0.8%
 At 1 year:0.8 to 1% (after 6 months) Adults:0.8%")
13
Incidence By 1 year of age: 0.8-1.5% (constant into adulthood)
75% of full term and 95% of premature testes will descend (usually in 1st 3 months) 10% bilateral 80% of UDT palpable 20% impalpable (cryptorchid) Half intra-abdominal Other half – vanishing or atrophic 14% of boys have family history of same
 10% bilateral. 80% of UDT palpable. 20% impalpable (cryptorchid) Half intra-abdominal. Other half – vanishing or atrophic. 14% of boys have family history of same.")
14
Classification Abdominal Canalicular
Ectopic- perineum, femoral canal, superficial inguinal pouch, suprapubic, contralateral scrotum (due to gubernacular attachments)
")
15
Investigations Imaging does not influence management (overall accuracy of 44%) Physical exam is 84% accurate when done by a pediatric urologist Hormonal workup Bilateral impalpable testes: HCG stimulation (if normal gonadotrophin levels) False negatives possible FSH / MIS / Inhibin B
 False negatives possible. FSH / MIS / Inhibin B.")
16
Histology The longer the testis is cryptorchid, the more likely it is to be histologically abnormal - changes appear by 1 ½ yrs of age The higher the testis the more pronounced the abnormality Hypolasia of Leydig cells, smaller seminiferous tubules, fewer spermatogonia, peritubular fibrosis Unclear whether changes in testis are due to intrinsic defect or secondary to cryptorchid state (changes often seen in contralateral testis)
")
17
Undescended Testis: Histology & Germ Cell maturation
Primary dysgenesis in 20 – 100% By 2 years, 30 – 40% are aspermatogenic (as early as 15 months) Ong et al, Pediatr Surg Int, 21: , 2005
 Ong et al, Pediatr Surg Int, 21: ,")
18
Undescended Testis: Effects on Fertility - Paternity

19
Undescended Testis: Fertility – hormone levels
Inhibin B and FSH: Biomarkers of seminiferous tubule integrity Correlate well with sperm density In a cohort of post-op patients, age at orchidopexy was found to correlate Inversely with Inhibin B levels Positively with FSH and serum Testosterone levels Indirect evidence favoring early orchidopexy Lee et al, J Urol, 160: , 1998 and 167: , 2002

20
Current recommendations
For truly undescended testes: Surgical correction anytime after 6 months, preferably before age 1 Testes that descend are likely to do so by the age of 6 months (Wenzler et al, J Urol, 2004) Biopsy at orchidopexy has demonstrated more spermatogonia per tubule and larger diameter of seminiferous tubules <1 year of age
 Biopsy at orchidopexy has demonstrated more spermatogonia per tubule and larger diameter of seminiferous tubules <1 year of age.")
21
Risk of Neoplasia Testicular Ca incidence 1 in 100,000
10% have a H/O UDT Incidence of Test Ca in UDT is 1 in 2550 (Farrer et al, 1985) for a RR of 40x Intra-abdominal testes have 6 times greater risk than inguinal testes (half the tumors) RR 3.6 in contralateral descended normal testis in men with unilateral cryptorchidism
 for a RR of 40x. Intra-abdominal testes have 6 times greater risk than inguinal testes (half the tumors) RR 3.6 in contralateral descended normal testis in men with unilateral cryptorchidism.")
22
Nubbins? Remnant gonadal tissue at inguinal exploration should be excised because 13% have viable residual testicular elements Theoretical risk: Approx 10% contain residual tubules 5.6% contain germ cells (De Luna et al, 2003)
")
23
Biopsy? Carcinoma in situ incidence – 1.7%
More common in abdominal testis But no definite correlation with later development of malignancy Justifiable in high risk groups: Danish Older boys presenting with cryptorchidism Transplant considerations

24
Surgical Intervention
EUA to locate testis Palpable – Inguinal orchidopexy Impalpable – Laparoscopy

25
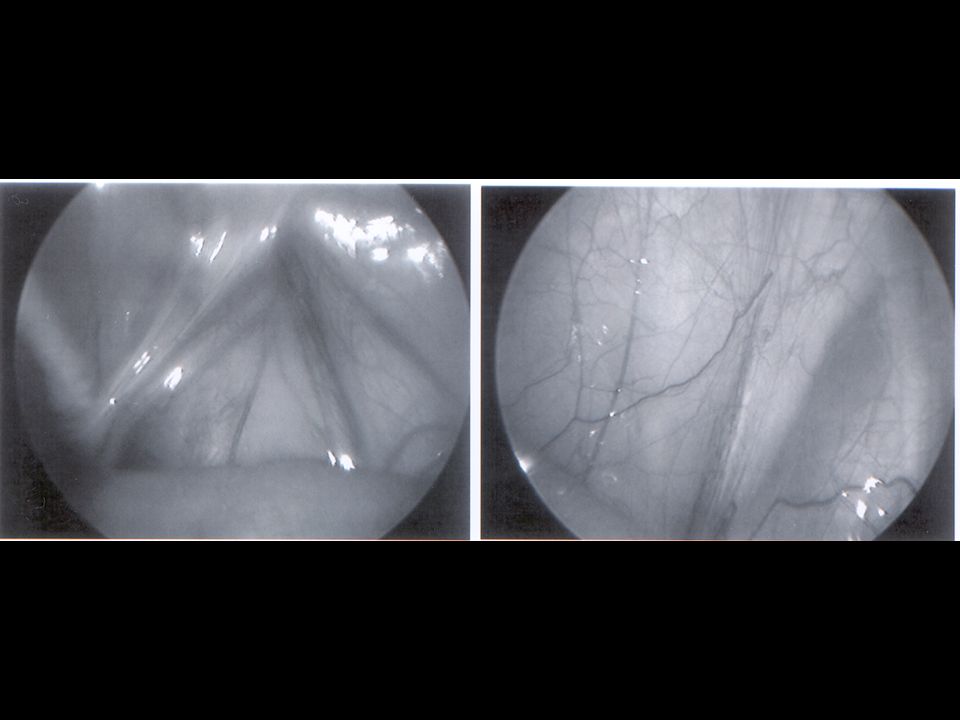
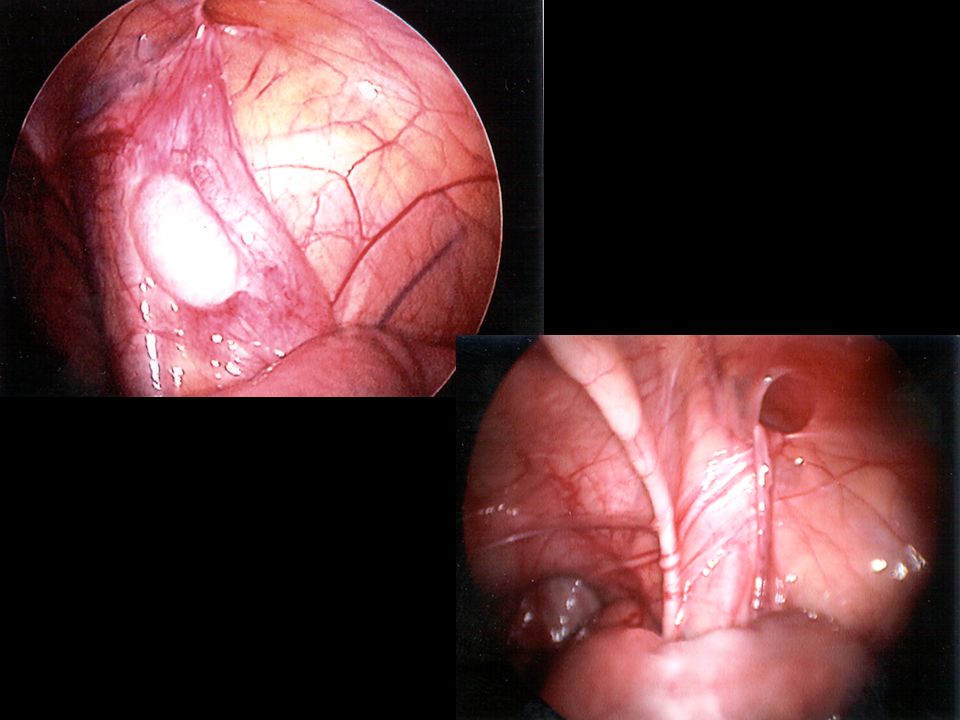
Laparoscopy For locating non-palpable testes (>95% accuracy)
Findings: Blind ending vessels above internal ring Cord structures entering internal ring Intra-abdominal testis

30
Surgical Intervention
Nubbin – excise Contralateral orchidopexy? Role of Scrotal Orchidopexy Bianchi approach

31
Bianchi procedure Single high scrotal incision – 1980’s
Several large reported series since Rajimwale et al, Ped Surg Int 2004 (Denver) Samuel and Izzidien, Ped Surg Int 2008 (Cardiff) Bassel et al, J Urol, 2007 (Atlanta) Applicable in UDT situated in the superficial inguinal pouch or lower Processus vaginalis approachable Single incision
 Samuel and Izzidien, Ped Surg Int 2008 (Cardiff) Bassel et al, J Urol, 2007 (Atlanta) Applicable in UDT situated in the superficial inguinal pouch or lower. Processus vaginalis approachable. Single incision.")
33
Extravaginal Torsion “Bilateral neonatal torsion” – LaQuaglia et al, J Urol, 1987 4 cases between ; 2 asynchronous, 1 salvaged “Perinatal extravaginal torsion of the testis in the first month of life is a salvageable event” – Sorensen et al, Urology, 2003 10 boys < 30 days old, with unilateral torsion – 4 saved

34
Extravaginal Torsion “Management of perinatal torsion: today, tomorrow or never?” – Yerkes et al, J Urol, 2005 18 pts in 3 institutions over 3 years; 4 had contralateral unsuspected torsion resulting in atrophy (22%) – 2 others in early stages were salvaged “Perinatal testicular torsion: preoperative radiological findings and the argument for urgent surgical exploration.” – Ahmed et al, J Pediatric Surg 2008 (San Diego – 2 pts) “Neonatal bilateral testicular torsion: a plea for emergency exploration” – Baglaj and Carachi, J Urol, 2007 (Scotland – 3 cases and lit review)
 – 2 others in early stages were salvaged. Perinatal testicular torsion: preoperative radiological findings and the argument for urgent surgical exploration. – Ahmed et al, J Pediatric Surg 2008 (San Diego – 2 pts) Neonatal bilateral testicular torsion: a plea for emergency exploration – Baglaj and Carachi, J Urol, 2007 (Scotland – 3 cases and lit review)")
35
Extravaginal Torsion Management: Timing: If diagnosis certain: If not:
Scrotal exploration / orchiectomy / contralateral orchidopexy If not: Inguinal exploration Timing: If seen immediately: at next available opportunity If seen later: decide after due counseling

37
Testicular Ascent Prevalence of undescended testes stable after age 1 ~ 1% Reported orchidopexy rates are as high as 2 to 3% of all boys up to age 14 to 17 years Barthold et al, J Urol, 170: , 2003 Initially thought to be due to treatment of retractile testes

38
Testicular Ascent Possible Etiologies: Persistent processus vaginalis
Ligamentous PV causing tethering Cremaster spasticity i.e Cerebral Palsy High scrotal testes (“gliding”) Mobile superficial inguinal pouch testes Failure of testicular vessels to elongate Scarring after groin surgery Error in diagnosis – missed during infancy
 Mobile superficial inguinal pouch testes. Failure of testicular vessels to elongate. Scarring after groin surgery. Error in diagnosis – missed during infancy.")
39
Testicular Ascent: To Pex or Not to Pex?
Dutch ‘national testis registry’ – 1986 Orchidopexy in ascended testis only for failure to descend at puberty (with testicular volume appropriate for age) In 2003, of 63 boys with 74 ascended testes: Hack et al, Br J Surg, 90:728-31, 2003 15 boys (20 testes) – operated at parental request 4 boys (4 testes) – lost to followup 42 of remaining 50 descended at puberty Recommended conservative management
 In 2003, of 63 boys with 74 ascended testes: Hack et al, Br J Surg, 90:728-31, boys (20 testes) – operated at parental request. 4 boys (4 testes) – lost to followup. 42 of remaining 50 descended at puberty. Recommended conservative management.")
40
Testicular Ascent: To Pex or Not to Pex?
Confirm diagnosis by serial examination of “retractile testes” 5 to 7% incidence of secondary ascent Conservative management if testicular volume appropriate for age, until puberty Operate if progressively higher location, or smaller volume Histological changes and germ cell counts similar to UDT ? Role of HCG

41
Conclusions Testicular location after birth variable
Spontaneous descent & ascent occur All boys need routine examination throughout childhood Closer surveillance of ‘retractile testes’ If undescended, orchidopexy between age 6 to 12 months Ascended testes may also need orchidopexy

Similar presentations



















; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")





