Download presentation
Presentation is loading. Please wait.

2
History: Gross hematuria Frothy urine HTN Recent/chronic illness (URI, Hep C, HIV, etc.) History of rheum disease or + ROS History of Cancer or + ROS Family history Increased edema
 History of rheum disease or + ROS History of Cancer or + ROS Family history Increased edema")
3
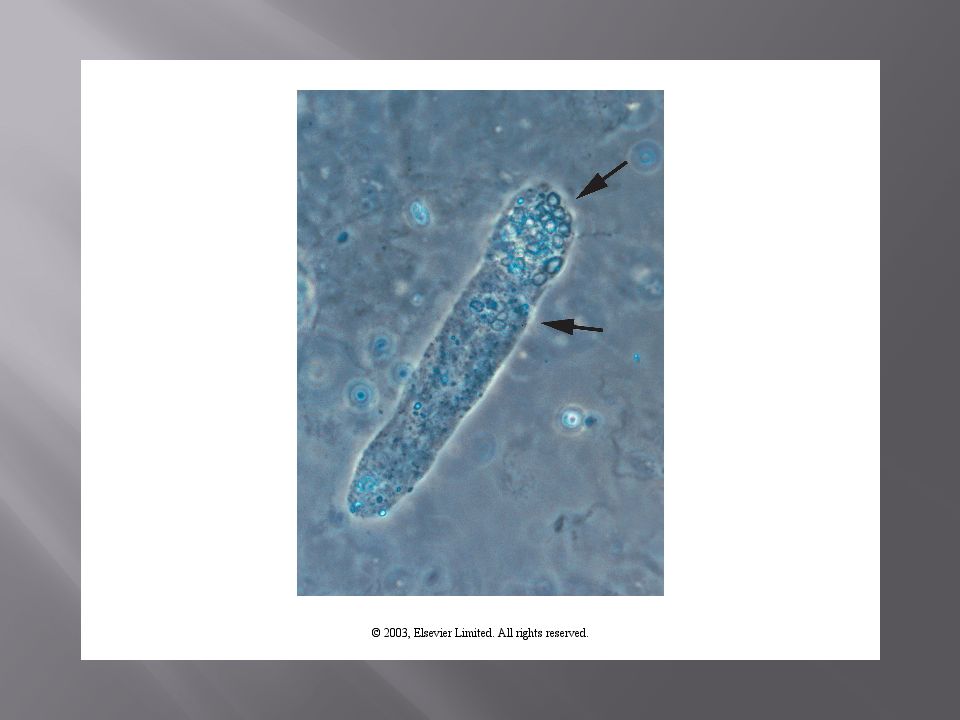
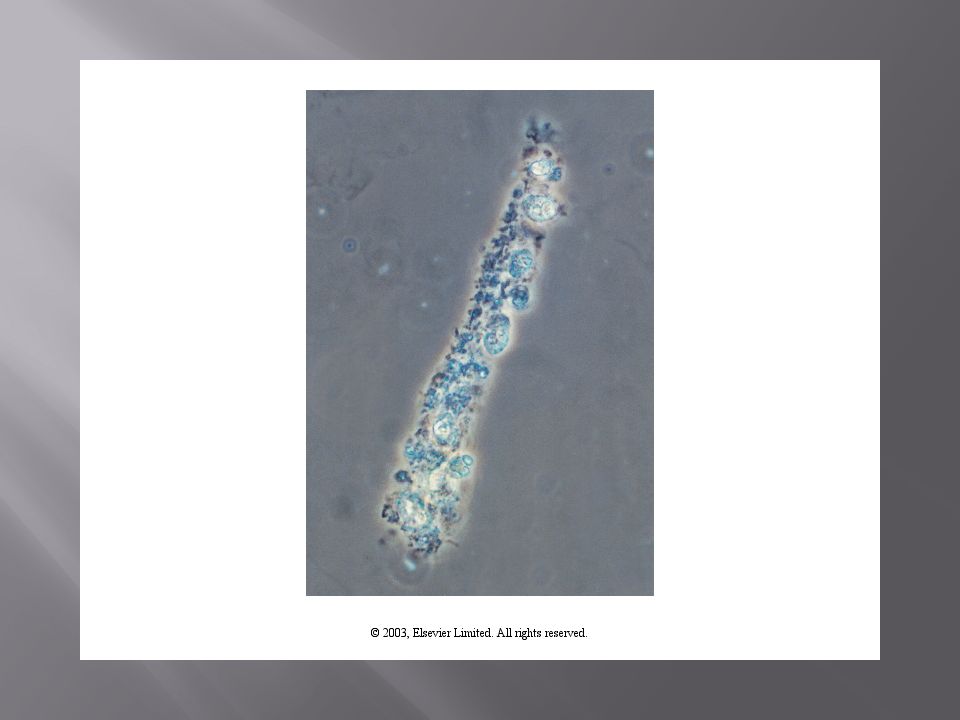
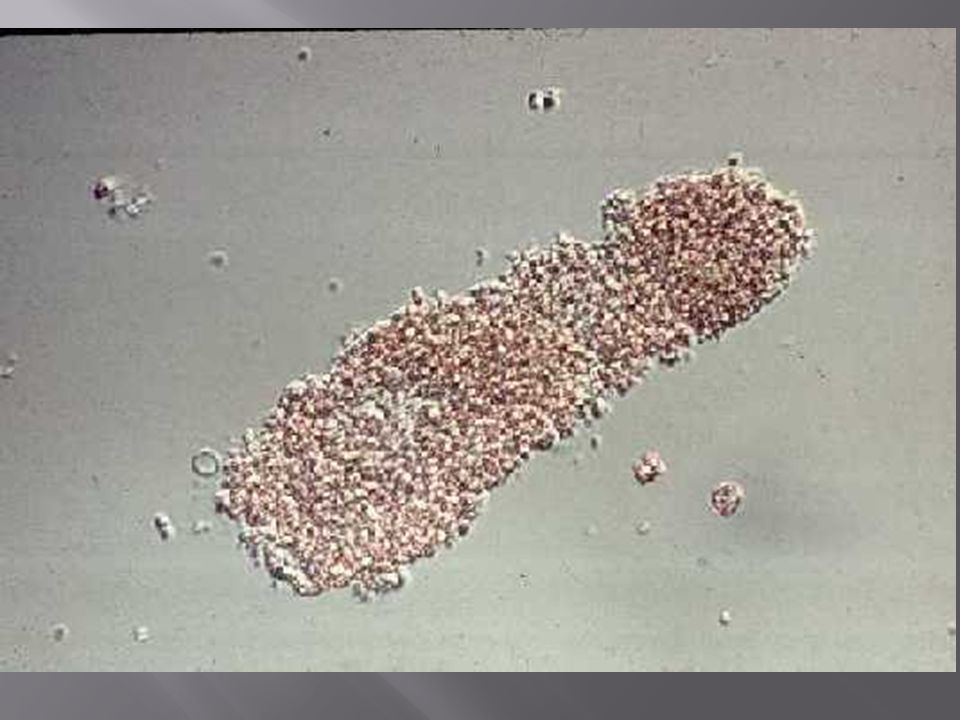
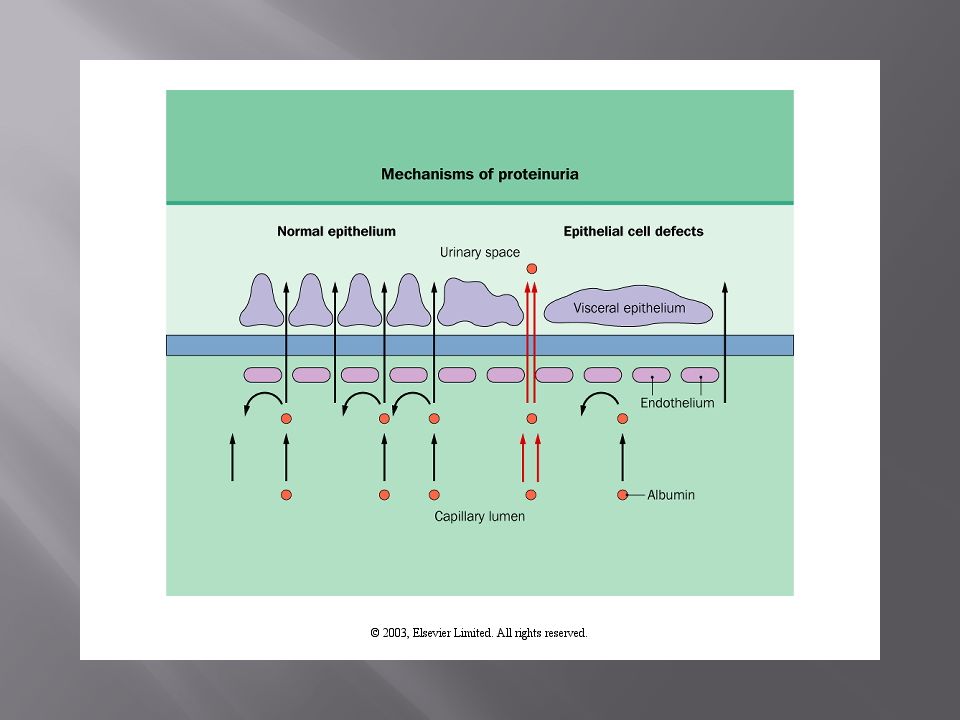
Active urine sediment: Granular/muddy brown casts Sterile pyuria vs. WBC casts Dysmorphic RBCs vs. RBC casts Proteinuria Nephrotic range proteinuria Non-nephrotic range proteinuria Paraproteinemia Progressive unexplained decline in GFR

12
Nephrotic syndrome: NRP: > 3.5 gm Low Albumin High cholesterol Lipiduria Edema More bland urine sediment Decreased change of HTN Pro-thrombotic state

13
MCD Membranous GN: primary and secondary FSGS: primary and secondary IGM nephropathy DM Fibrillary GN C1q nephropathy Amyloidosis IgA nephropathy PSGN, Lupus etc

14
Nephritic HTN Active urine sediment (Dysmorphic RBC/RBC cast) NNRP or NRP Edema with volume overload Oliguric Reduced GFR
 NNRP or NRP Edema with volume overload Oliguric Reduced GFR")
15
Lupus IgA nephropathy PSGN Vasculitis (Wegener’s, MPA, CS) Anti-GBM disease MPGN and Cryoglobulinemia Malignant HTN TTP/HUS Embolic/immune complex deposition disease
 Anti-GBM disease MPGN and Cryoglobulinemia Malignant HTN TTP/HUS Embolic/immune complex deposition disease")
16
Nephrotic Syndrome As previous Acute Glomerulonephritis As previous Chronic Glomerulonephritis Insidious/smoldering/slow progressive GN

17
Rapidly progressive glomerulonephritis Focal proliferative/necrotizing/Crescents Rapid decline in renal function (days/weeks) Vasculitis vs. Anti-GBM dz vs. TMA/TTP vs. IgA nephropathy vs. DPLN vs. PSGN vs. MPGN Asymptomatic Urinary Abnormalities Recurrent/persistent non-GU hematuria TBMD; Alport’s syndrome, IgA Isolated NNR proteinuria or sterile pyuria Same differential of NRP or TI dz Only one finding with no HTN, GFR decline abnormal exam findings

18
Each disease not limited to one classification IgA can present with all five Lupus can present with all five Disease continuum AUA to NRP to Acute GN to RPGN (Lupus) The neurology game of “guess the lesion” while awaiting renal biopsy (our MRI) Biopsy gold standard, but: Sample variation: may miss FSGS; Lupus IV/V Each histopathology diagnosis likely represents multiple pathophysiology mechanisms
 The neurology game of guess the lesion while awaiting renal biopsy (our MRI) Biopsy gold standard, but: Sample variation: may miss FSGS; Lupus IV/V Each histopathology diagnosis likely represents multiple pathophysiology mechanisms")
19
‘Permeability factor’ (evident post transplant) Genetic (nephrin, podocin, alpha-actin IV) ESRD common endpoint (hyperfiltration) Viral infection (Parvovirus, HIV) Elevated GH levels Obesity Reflux nephropathy Drugs (palmidronate, heroin)
 Genetic (nephrin, podocin, alpha-actin IV) ESRD common endpoint (hyperfiltration) Viral infection (Parvovirus, HIV) Elevated GH levels Obesity Reflux nephropathy Drugs (palmidronate, heroin)")
20
Membranous GN mesangial involvement suggests secondary cause: CA screening ANA; //DNA Hepatitis panel FSGS HIV Genetic testing MPGN Hepatitis panel Cryoglobulins C3/C4

21
Lupus Nephritis ANA // DNA C3/C4/C50 Vasculitis P-ANCA; C-ANCA CRP Anti-GBM disease Anti-GBM antibody Acute interstitial nephritis Serum/urine eosinophils

22
TMA/TTP Platelets Hgb Haptoglobin, LDH, indirect bilirubin Peripheral smear PSGN ASO Anti-DNAase Cryoglobulinemia Serum cryoglobulins

23
Paraproteinemia SPEP, UPEP, Kappa/Lambda light chain ratio IgA nephropathy IgA levels NOT diagnostic Galactose deficient IgA1 associated with disease IgM nephropathy IgM levels NOT diagnostic IgM to IgG ratio could be diagnostic Minimal Change Disease none Fibrillary GN none

24
Lupus Nephritis MPGN PSGN Cryoglobulinemia Embolic/Immune Complex deposition disease

25
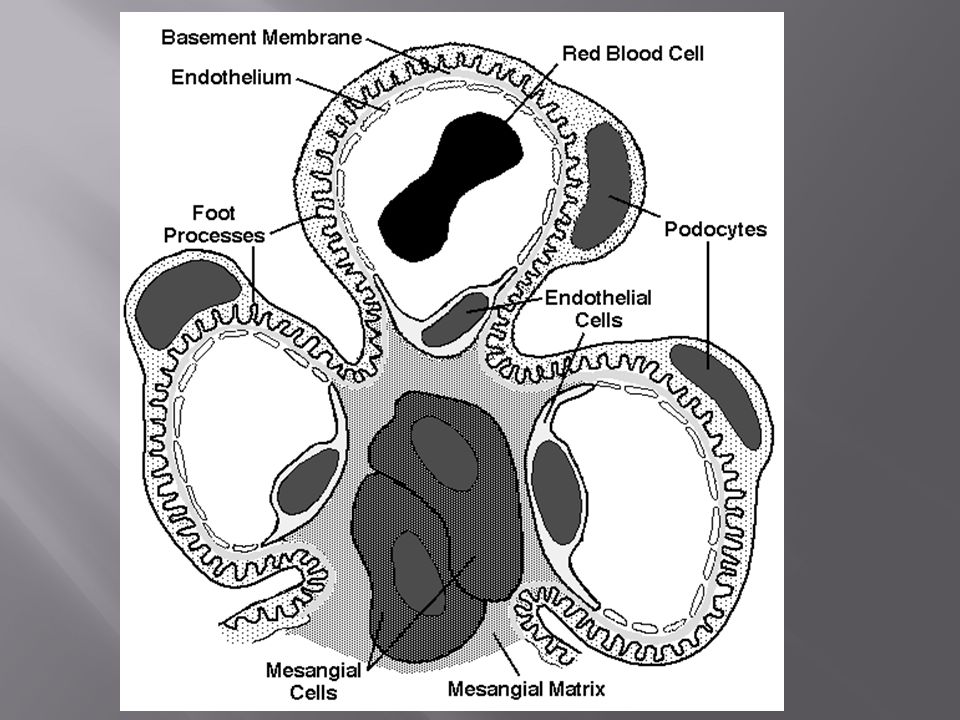
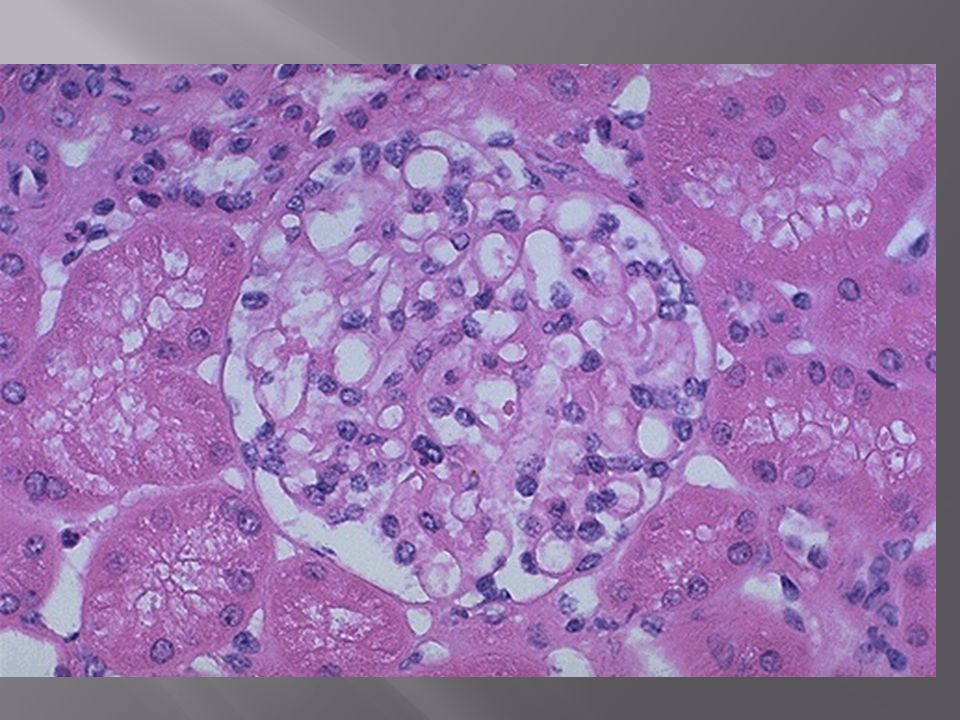
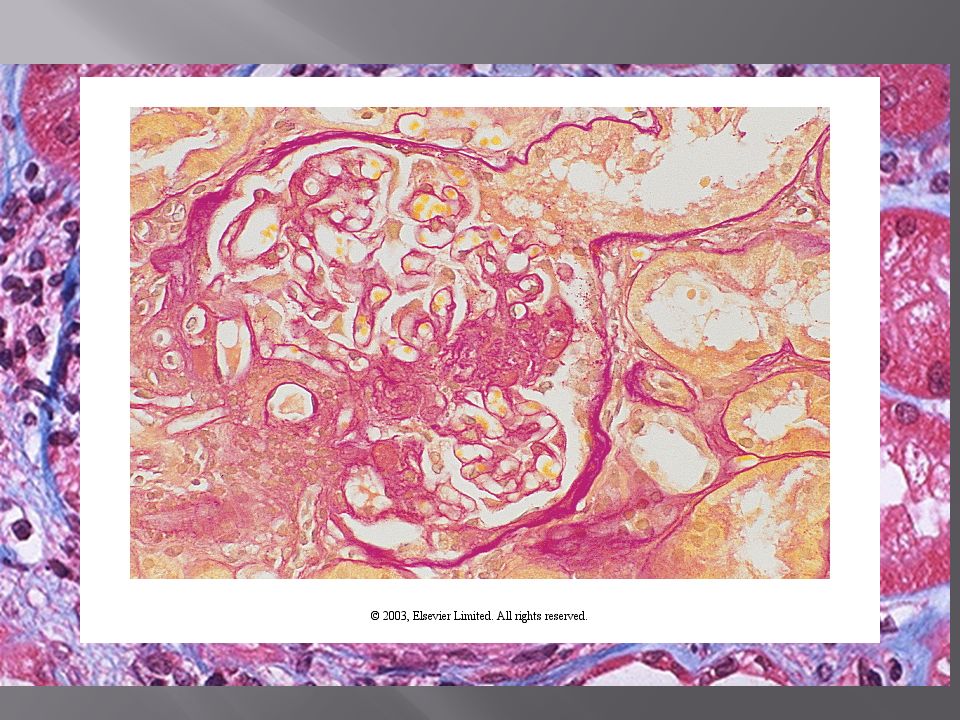
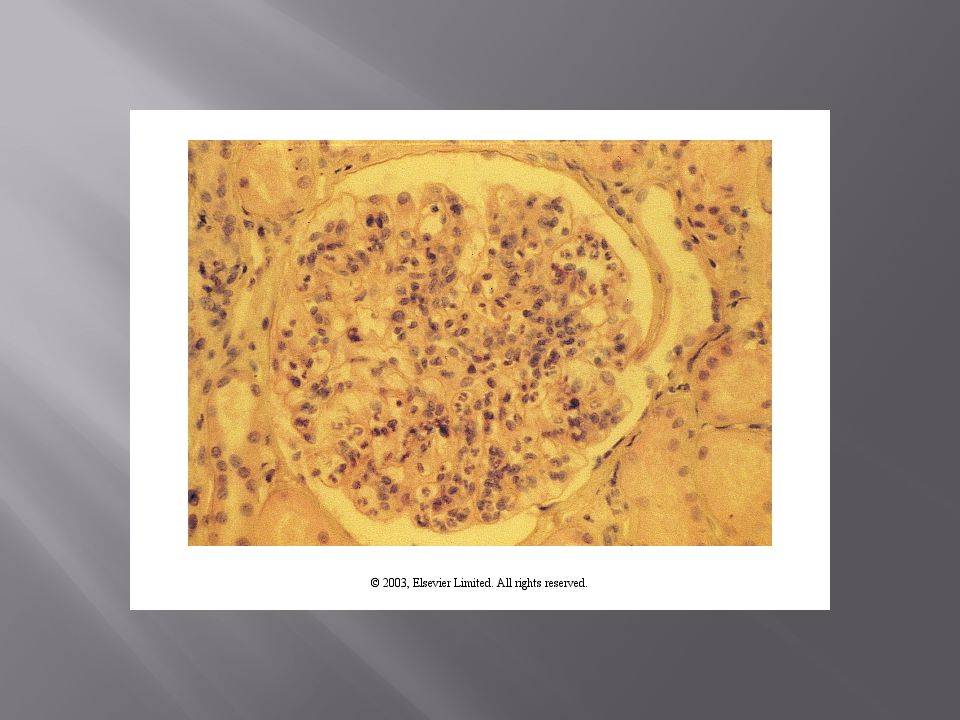
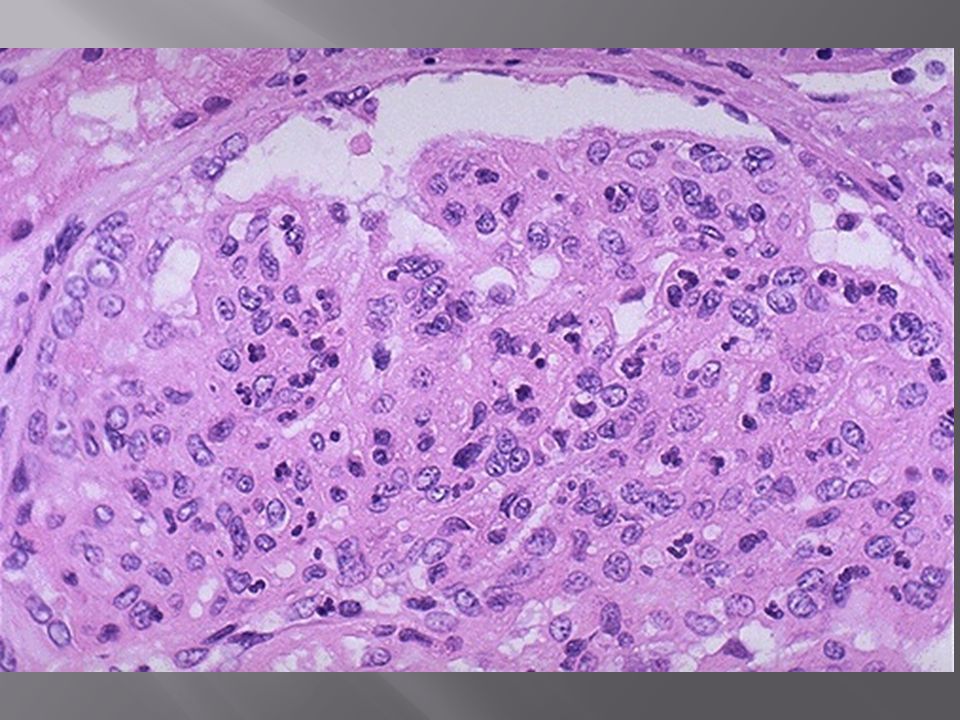
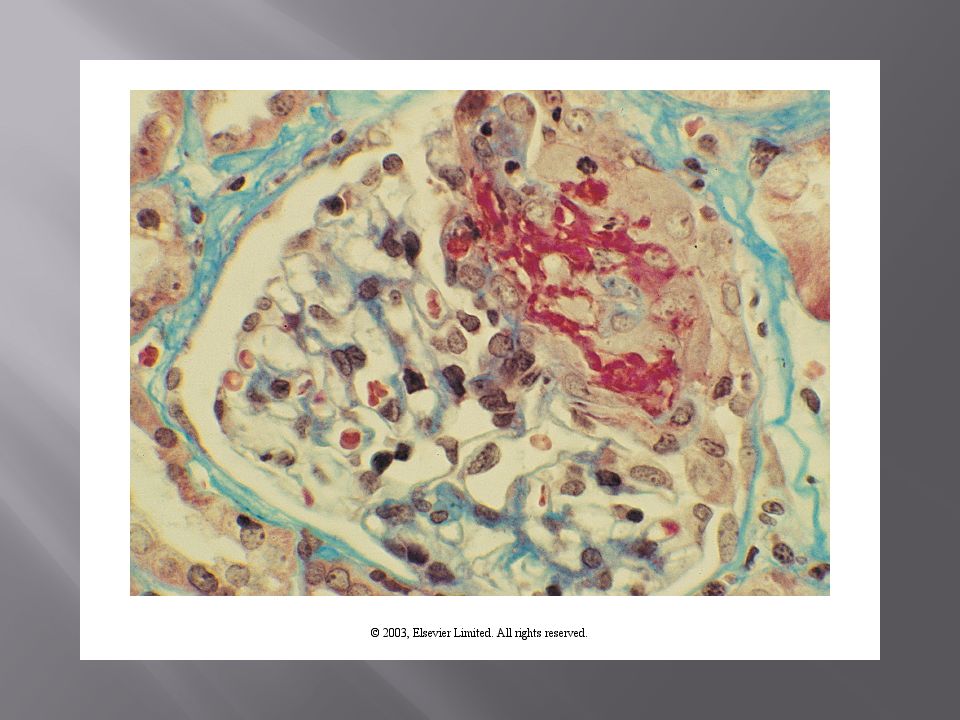
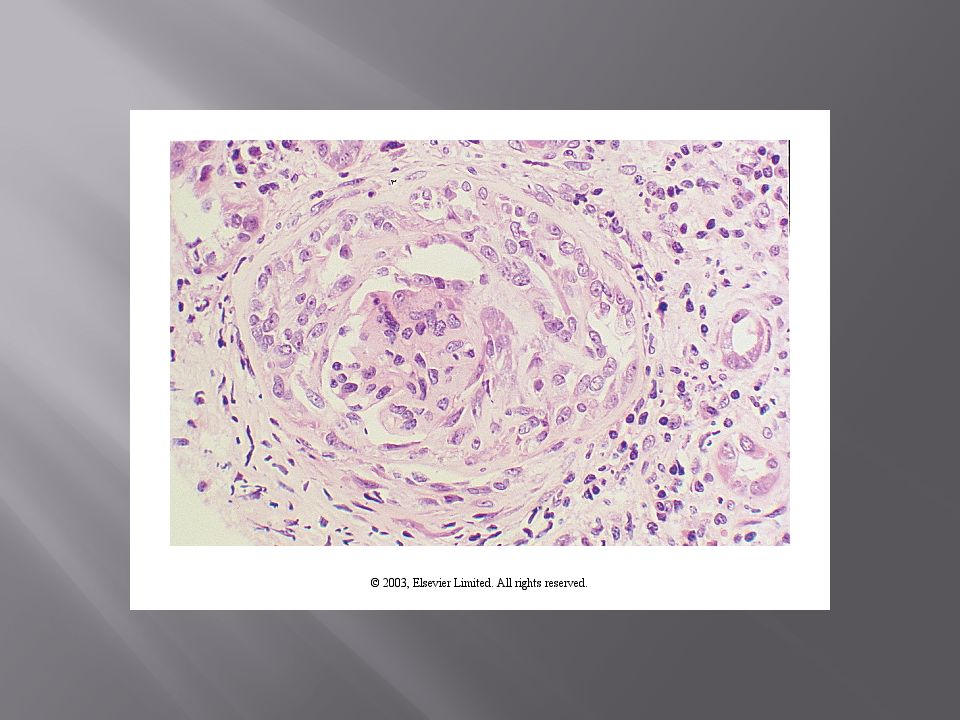
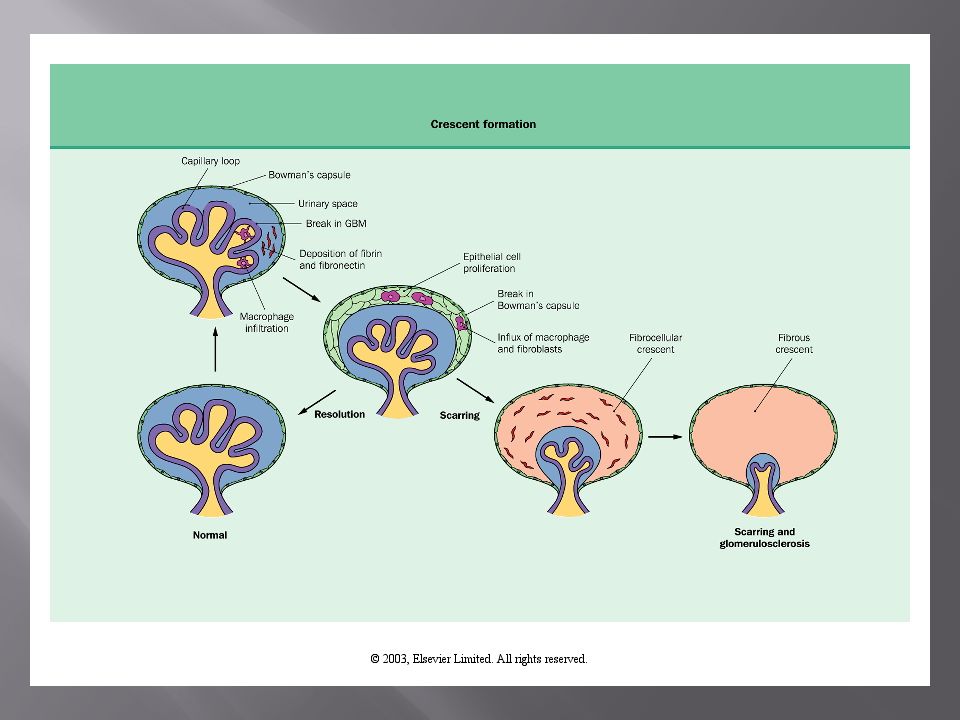
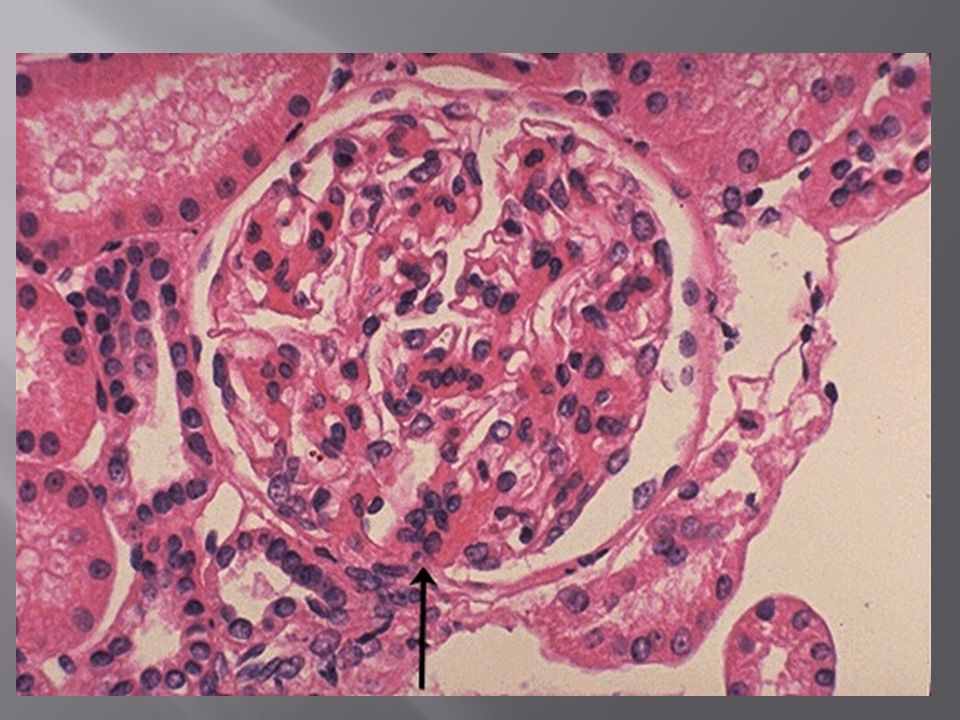
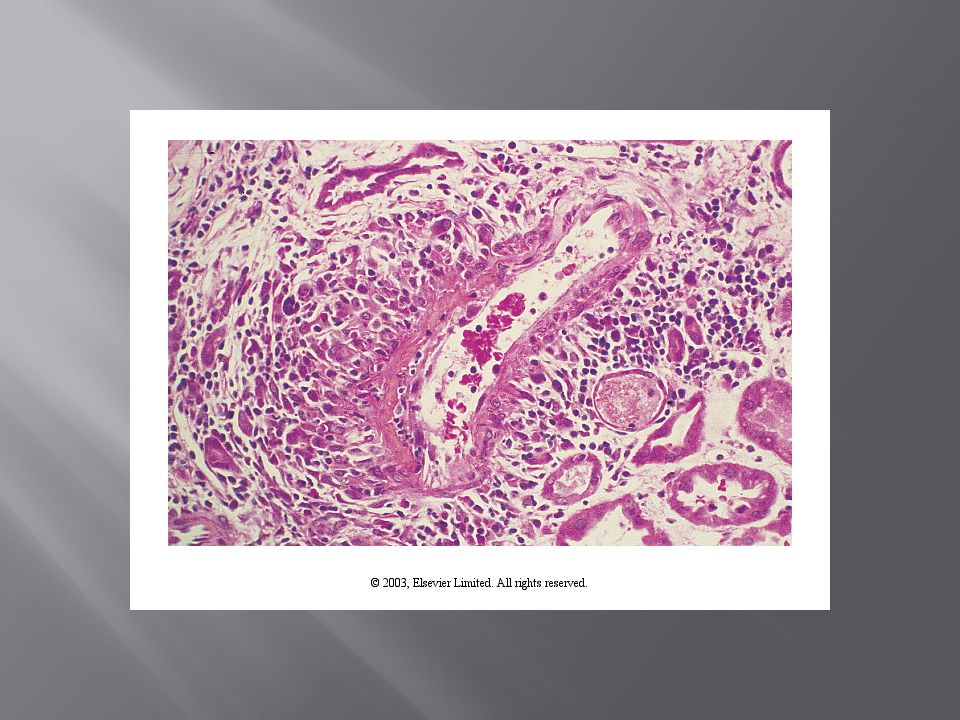
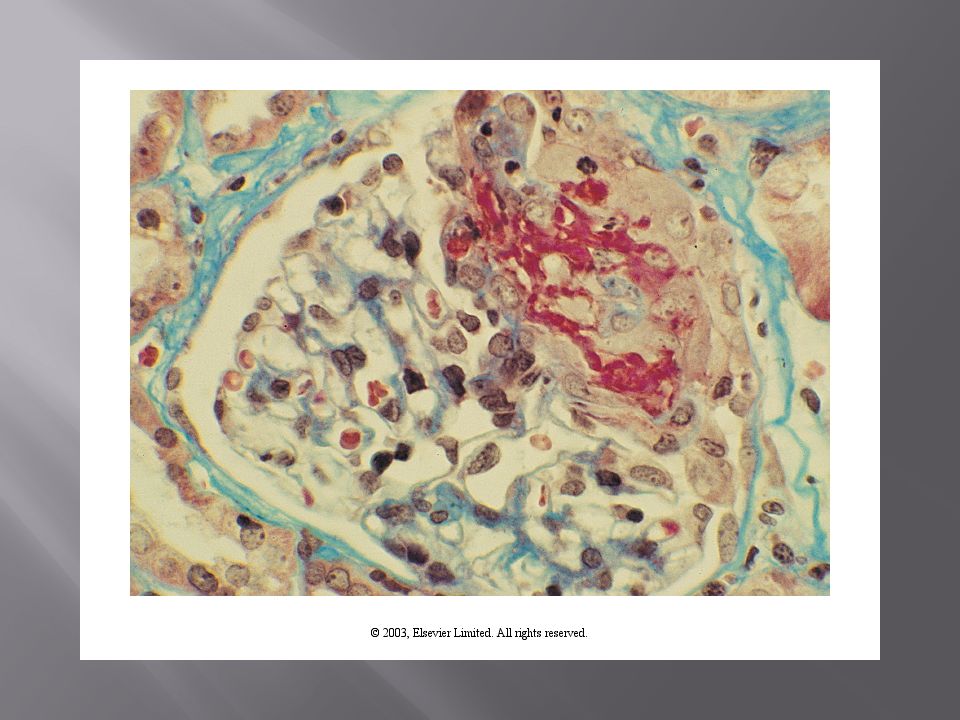
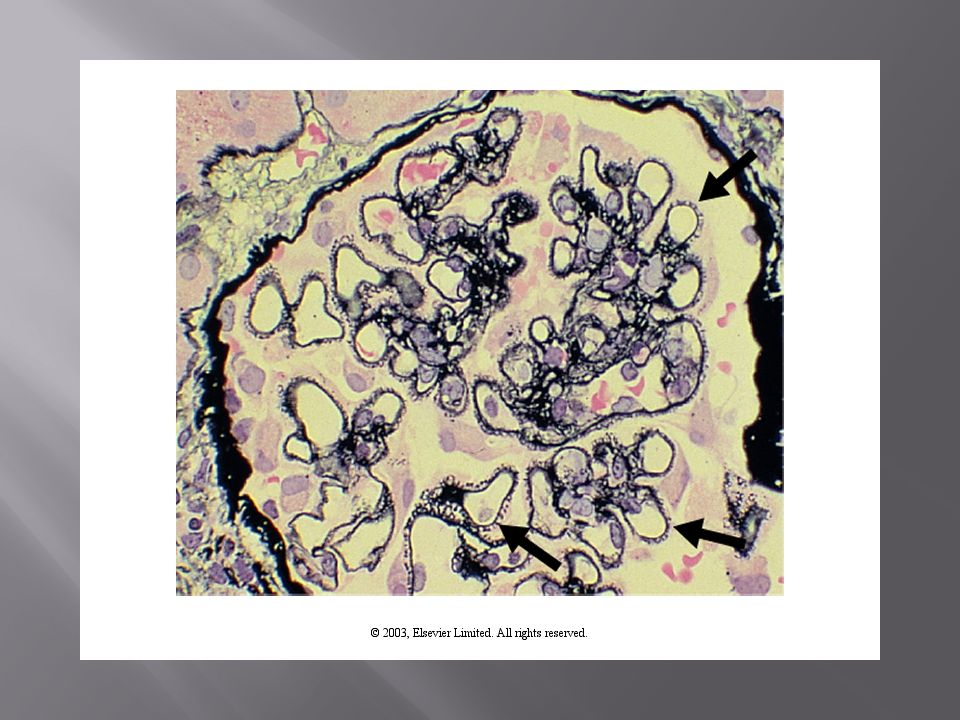
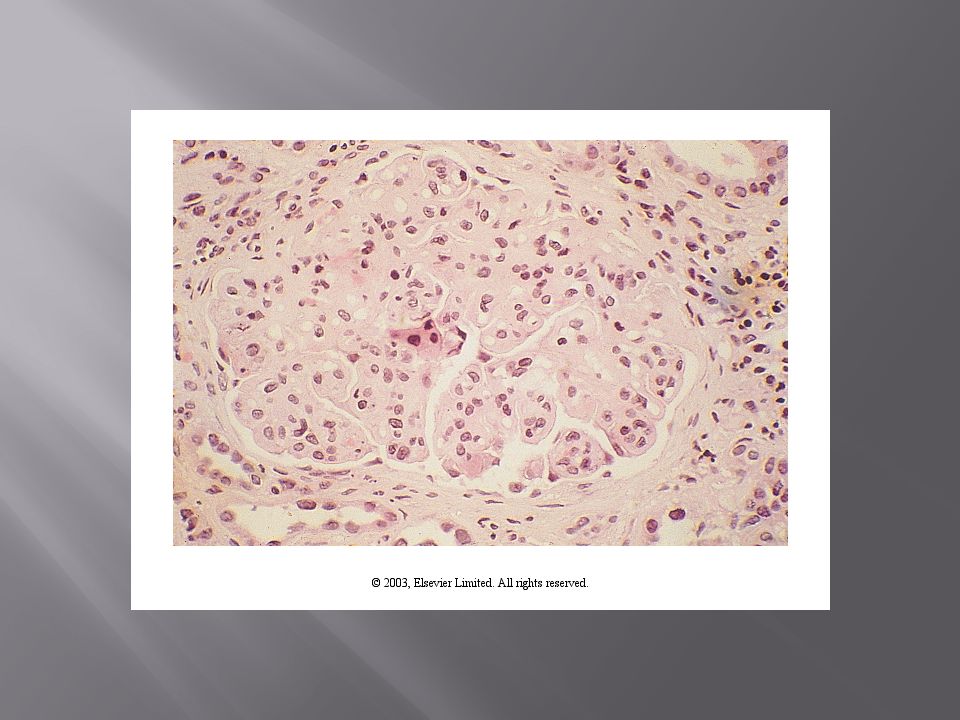
Light Microscopy Numerous stains: Silver stain GBM/matrix Hypercellular (proliferative) mesangial/endothelial Hypercellular (Exudative): Inflammatory leukocytes Glomerular necrosis : RPGN Crescents: Collection of inflammatory cells in Bowman’s space Capillary loop collapse; attachment to Bowman’s Thickening/division of capillary loops Tublules: Cells; cell inclusions, lumen contents Interstitium: Edema, infiltration, fibrosis
 mesangial/endothelial Hypercellular (Exudative): Inflammatory leukocytes Glomerular necrosis : RPGN Crescents: Collection of inflammatory cells in Bowman’s space Capillary loop collapse; attachment to Bowman’s Thickening/division of capillary loops Tublules: Cells; cell inclusions, lumen contents Interstitium: Edema, infiltration, fibrosis")
26
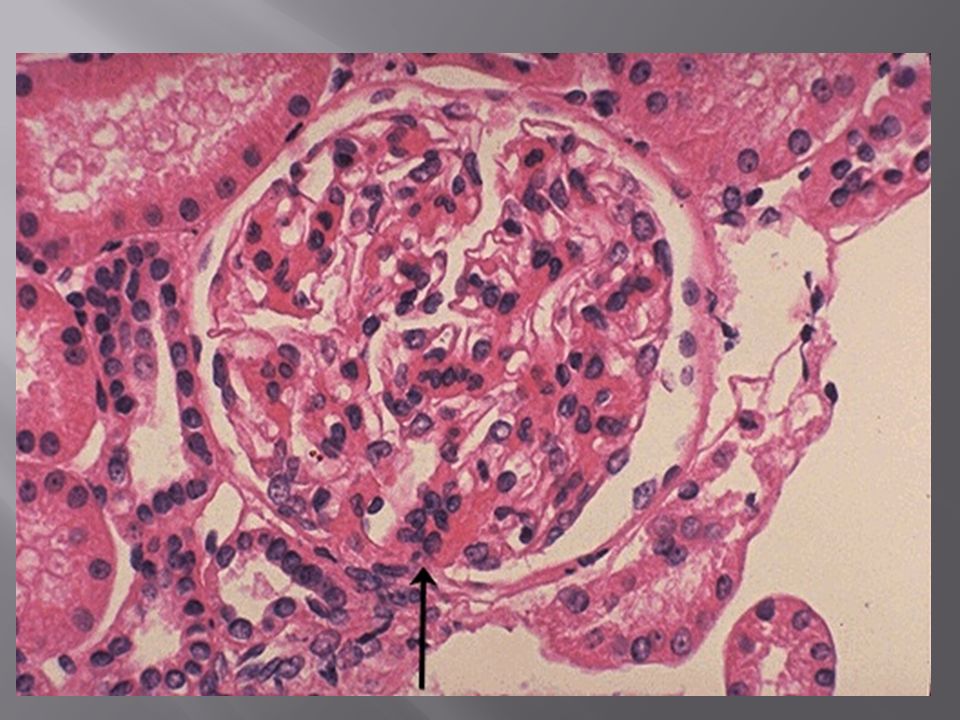
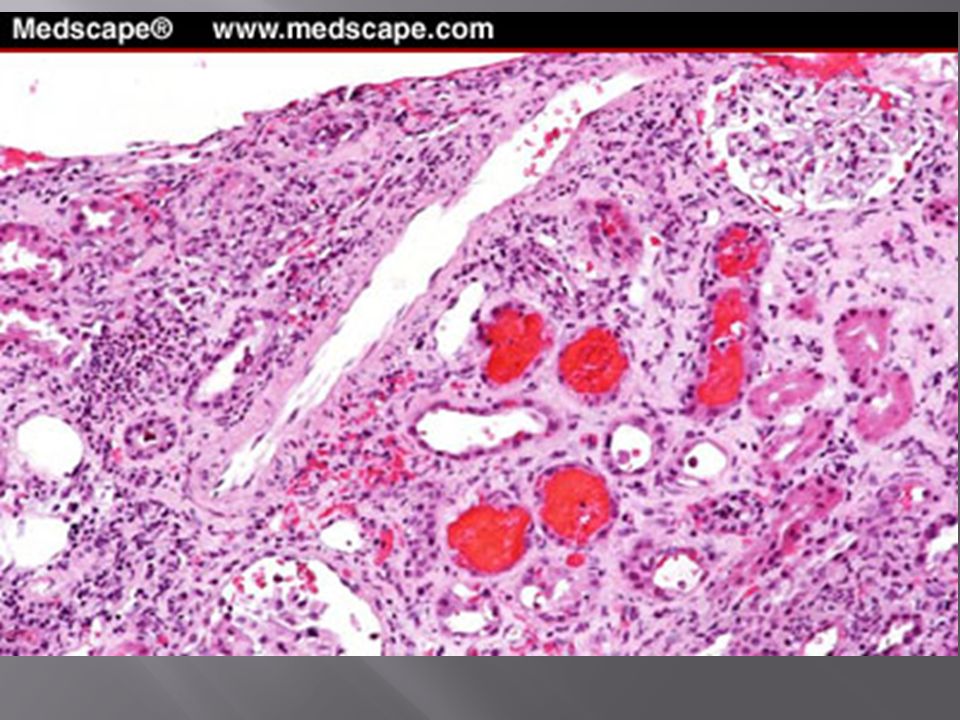
Interstitial Edema Interstitial inflammatory infiltrate Glomerular hypercellularity Glomerular Necrosis Increased mesangial matrix Congested tubules Cellular crescents

27
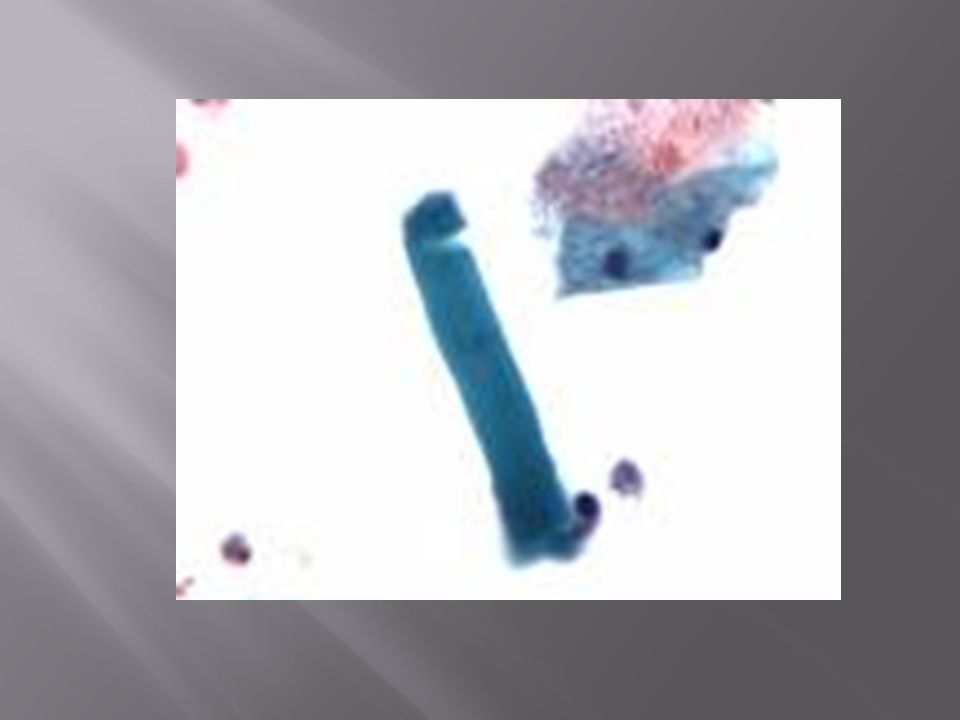
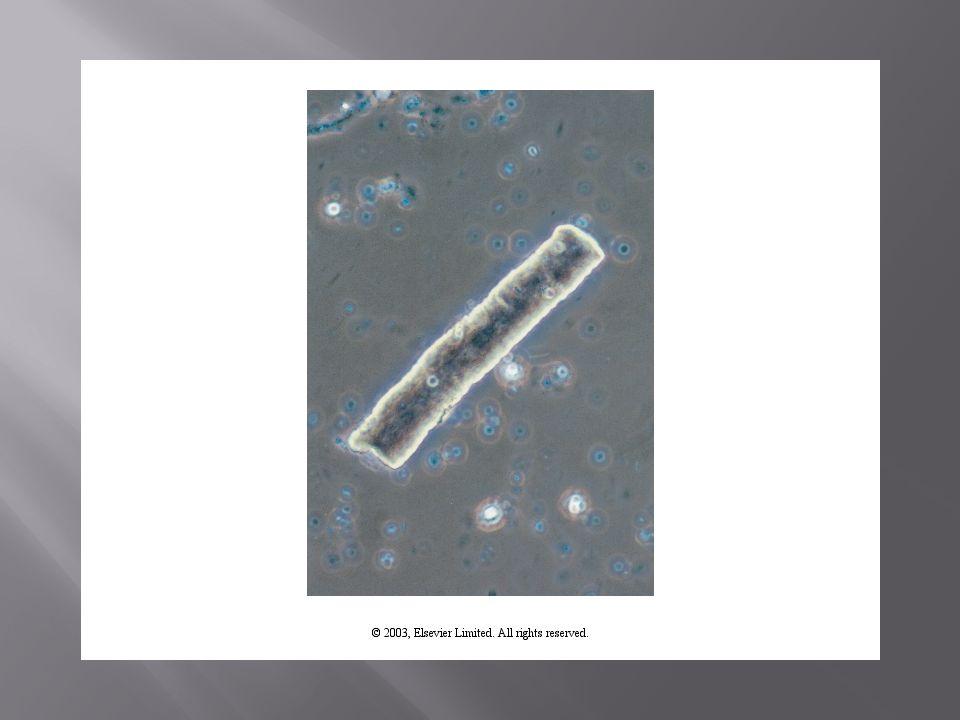
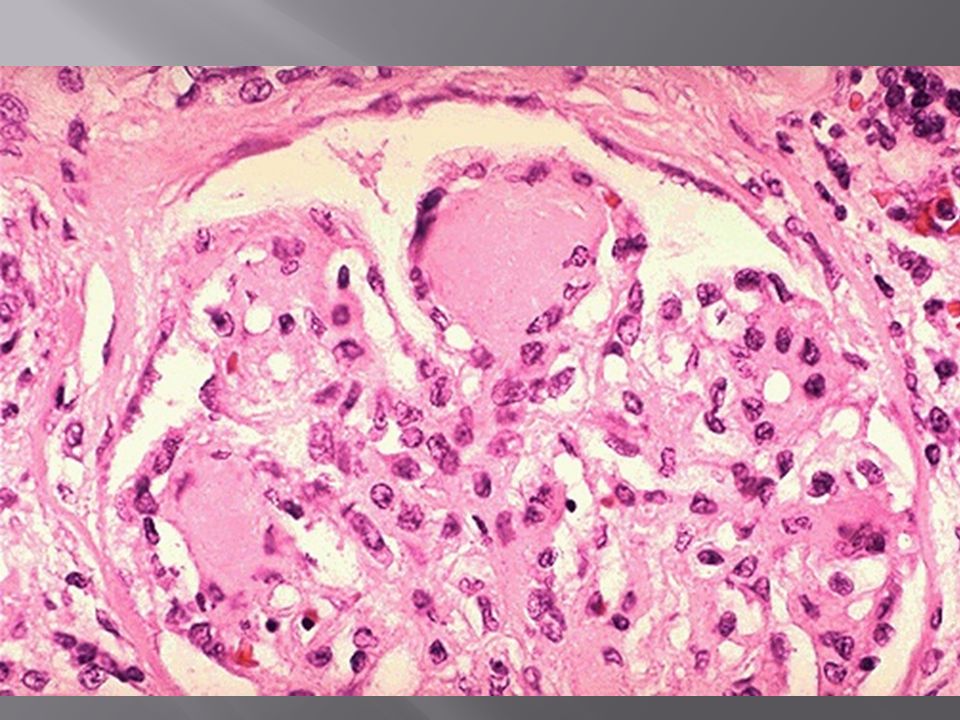
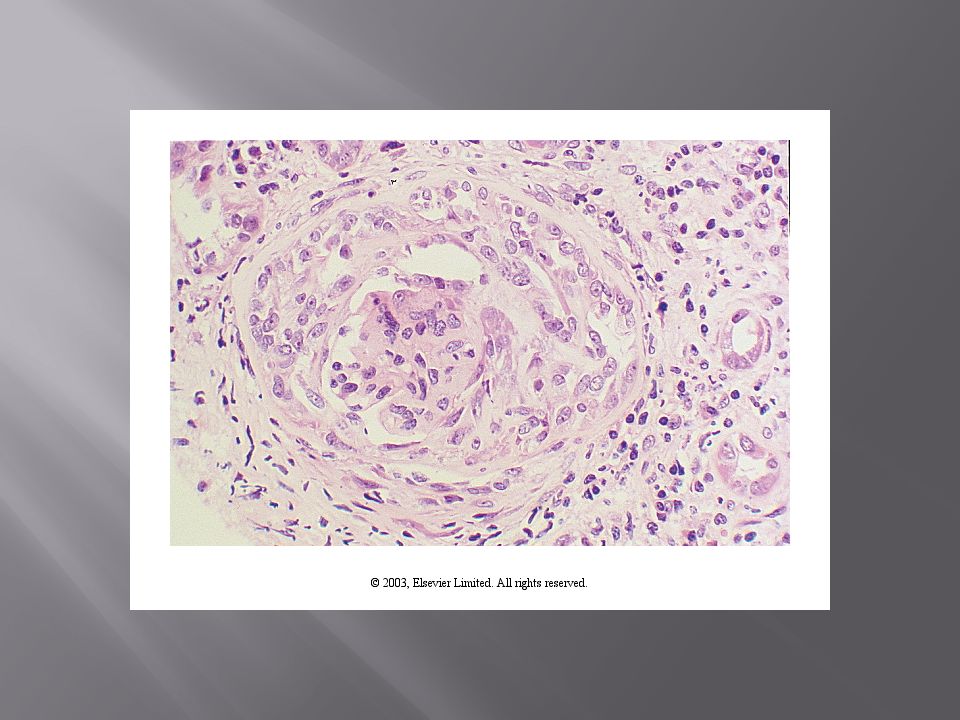
Interstitial Fibrosis Tubular Atrophy Glomerular sclerosis (obsolescence) Dilated tubules Results in broad waxy casts on urine microscopy
 Dilated tubules Results in broad waxy casts on urine microscopy")
42
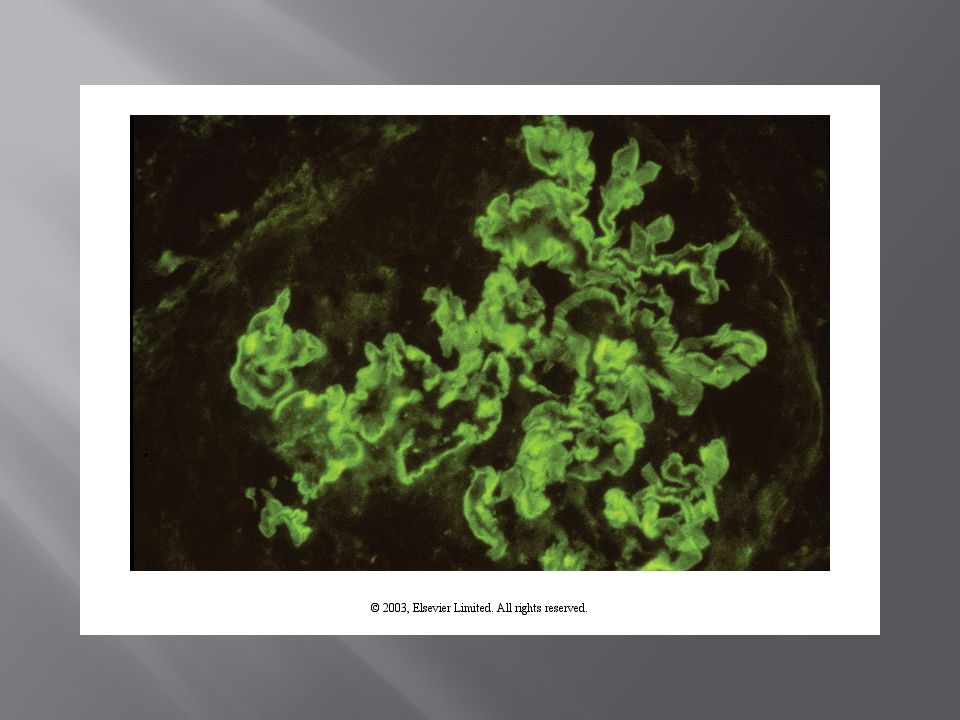
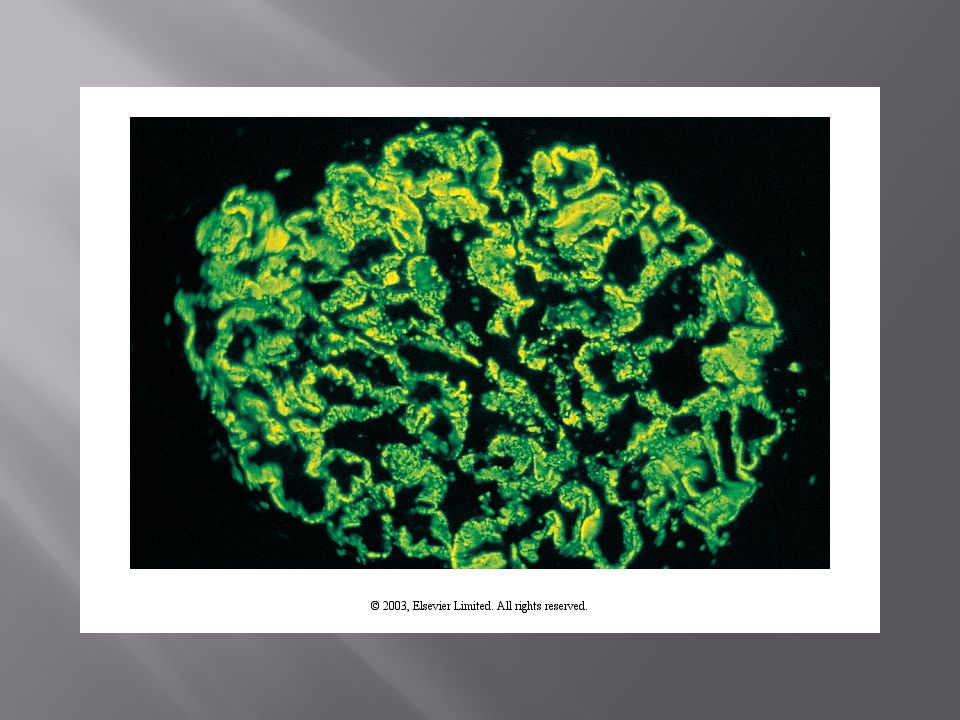
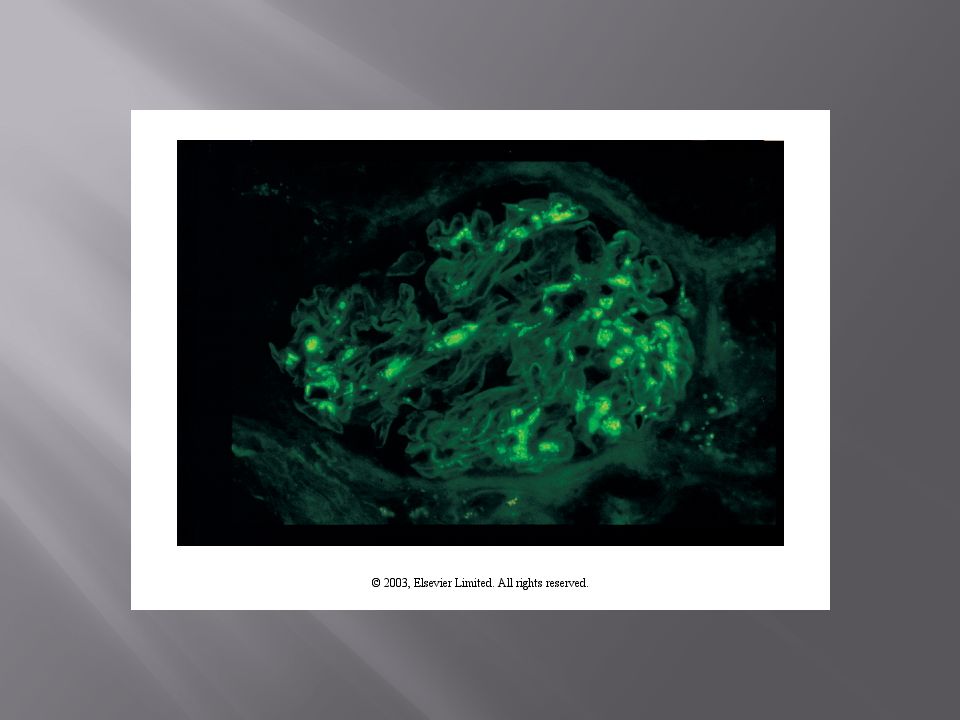
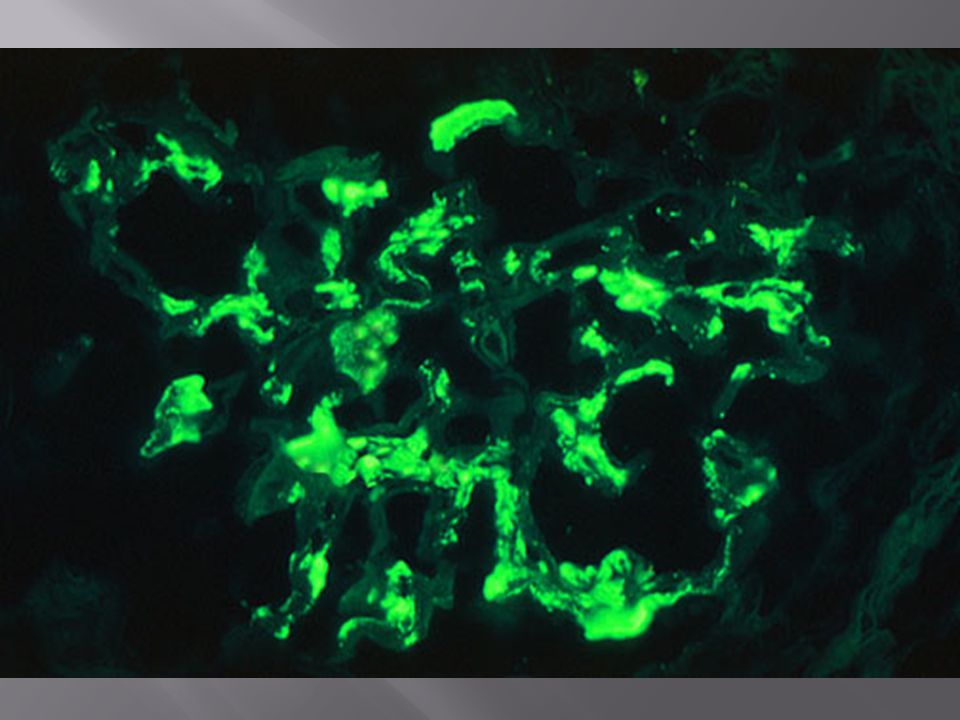
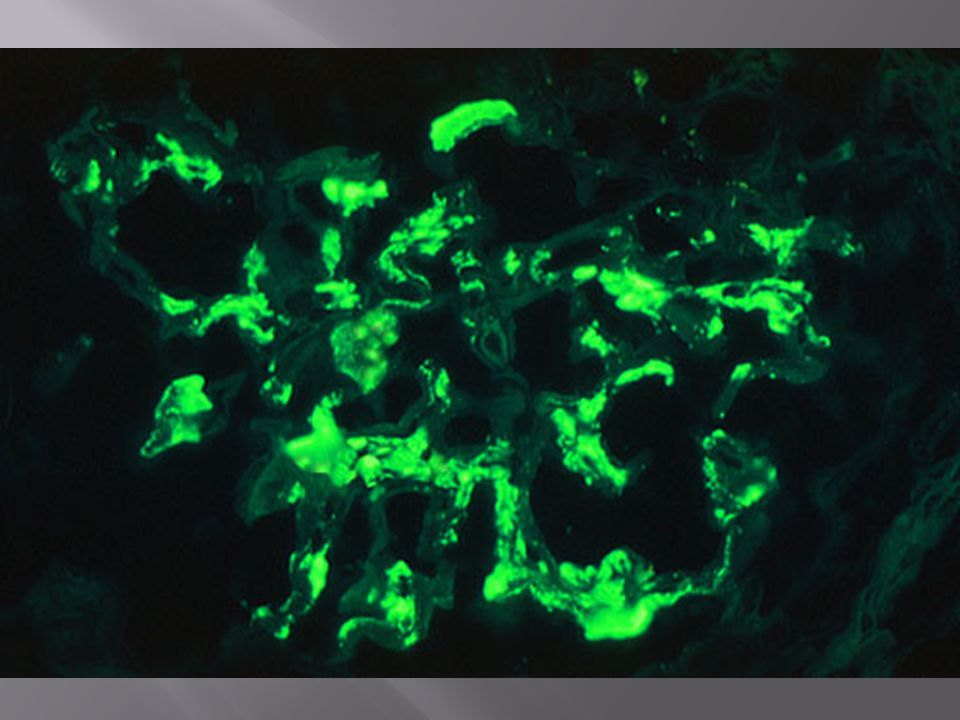
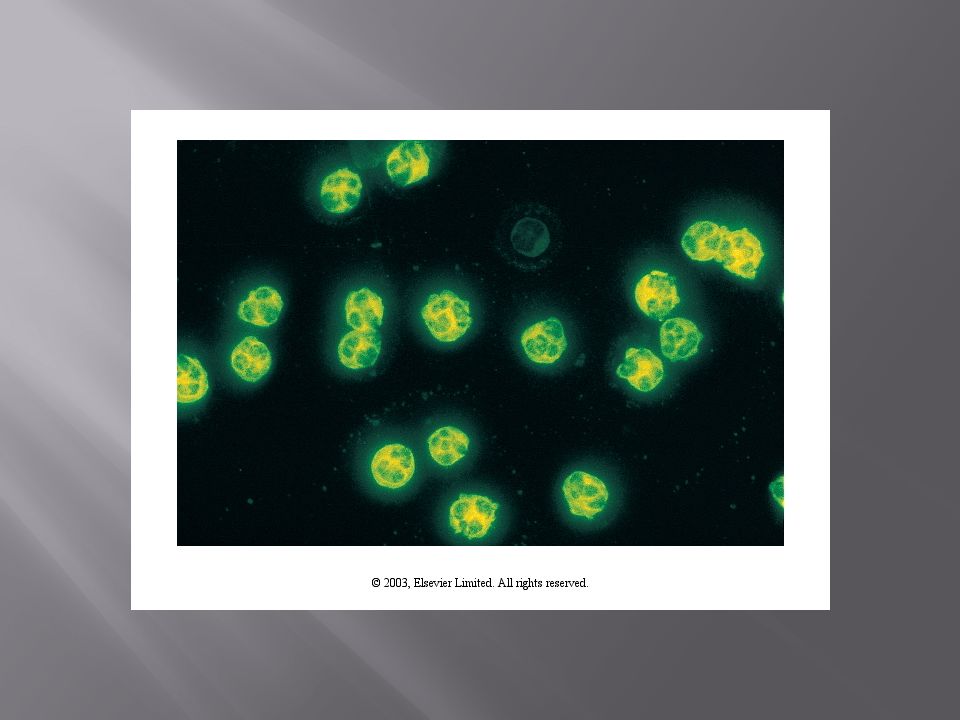
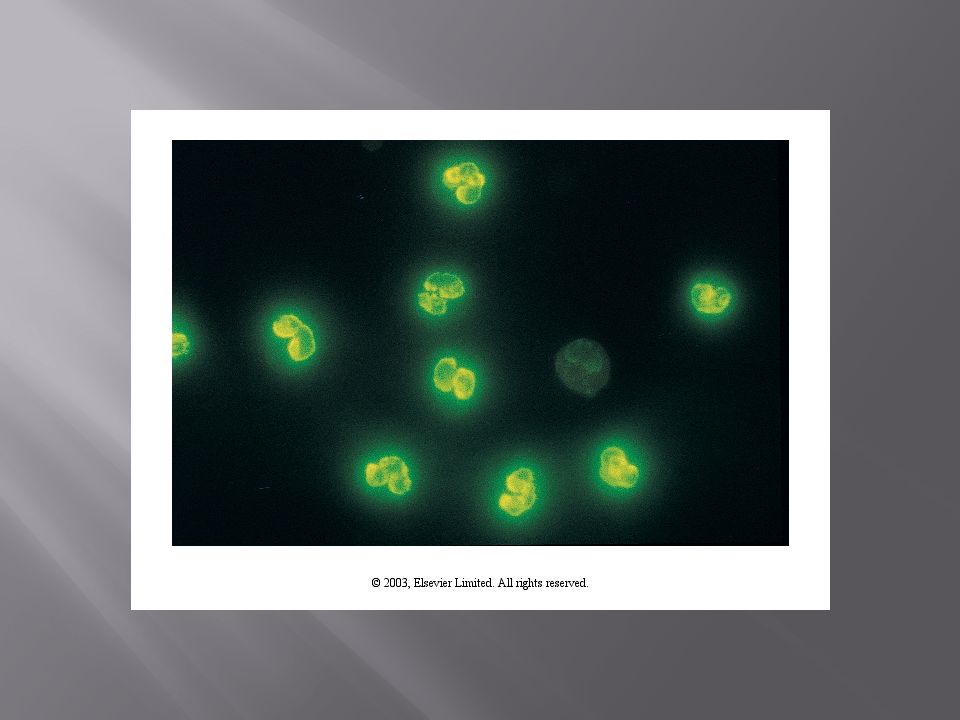
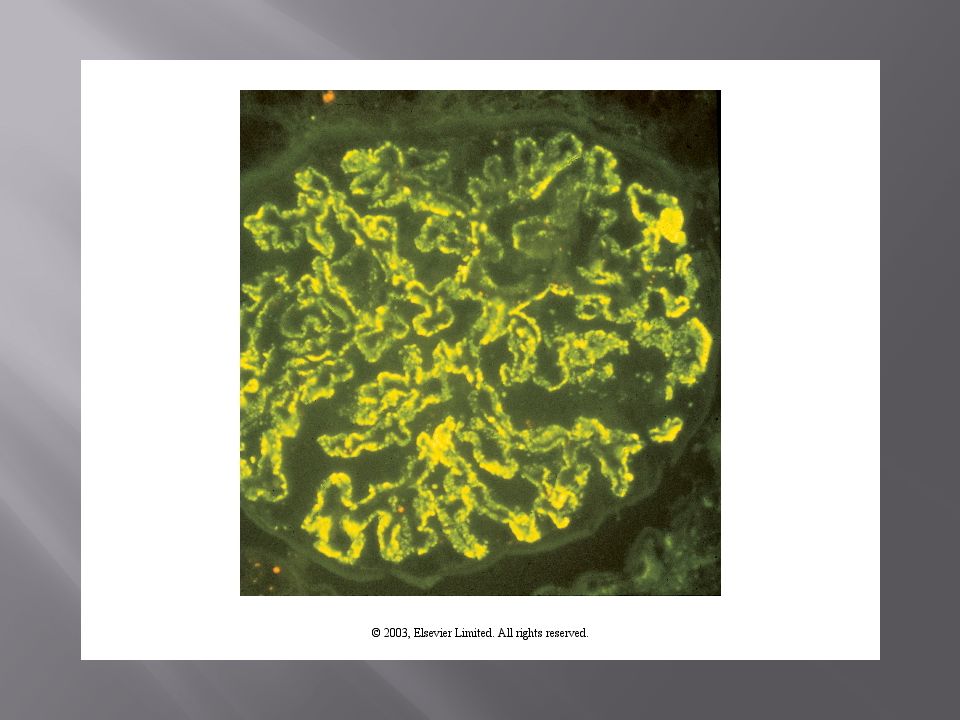
Immunofluorescence Evaluation for immune deposits Detect IgA, IgM, IgG, C3, C4, and C1q Also Fibrin (Crescents; capillaries in thrombotic dz) Linear (continuous) or granular (discontinuous) Anti-GBM: Linear GBM deposits Membranous GN: Granular GBM deposits Capillary walls or mesangium Vasculitis has a ‘pauci-immune’ IF Lupus has a ‘full house’ IF
 Linear (continuous) or granular (discontinuous) Anti-GBM: Linear GBM deposits Membranous GN: Granular GBM deposits Capillary walls or mesangium Vasculitis has a ‘pauci-immune’ IF Lupus has a ‘full house’ IF")
47
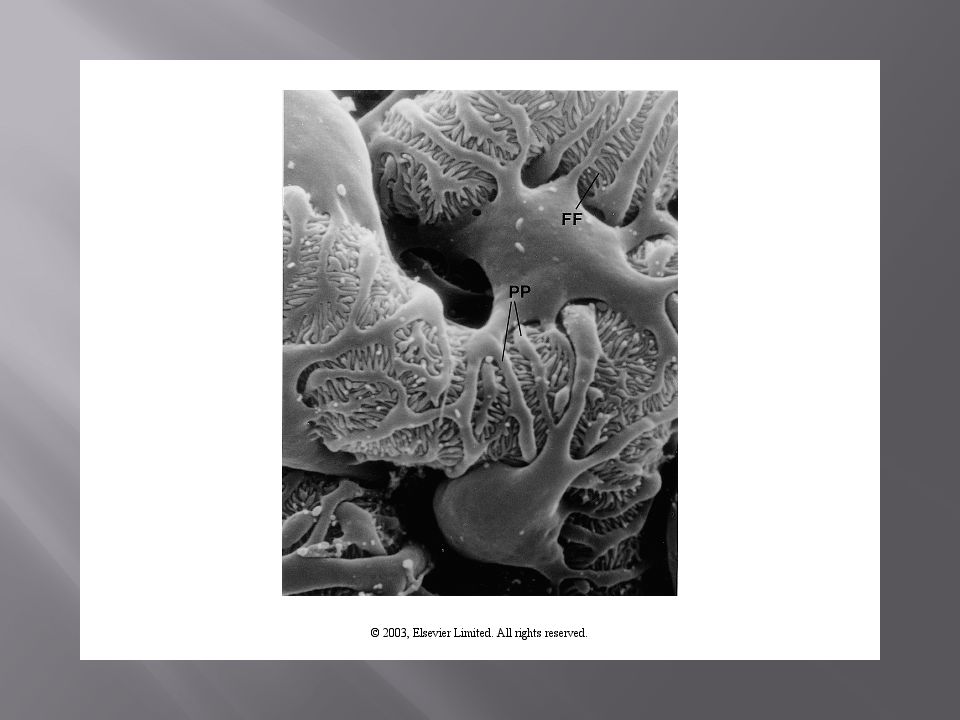
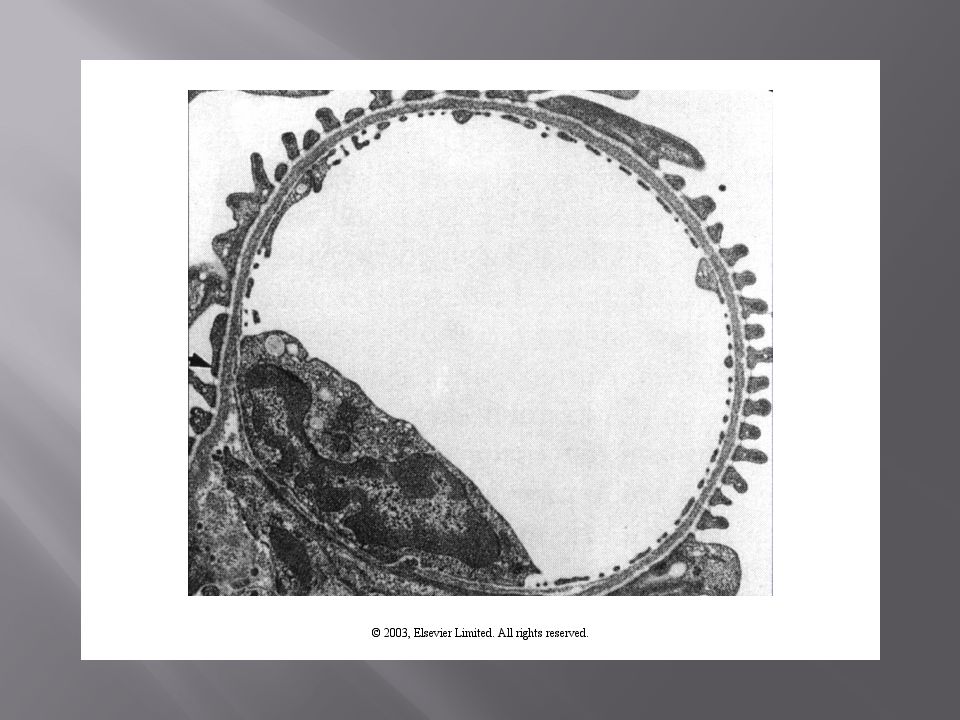
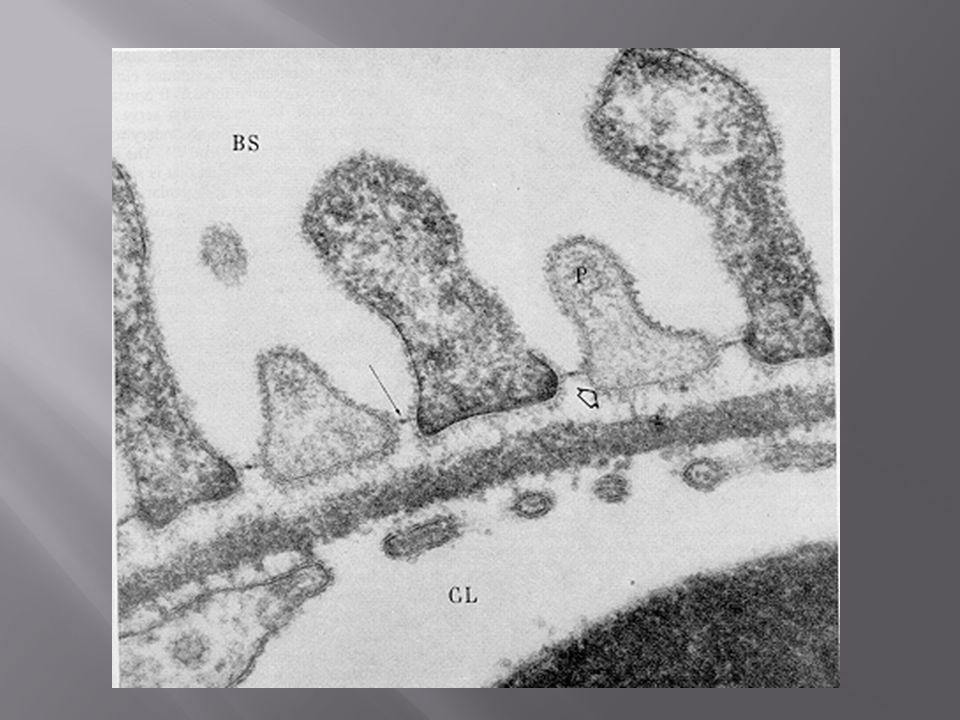
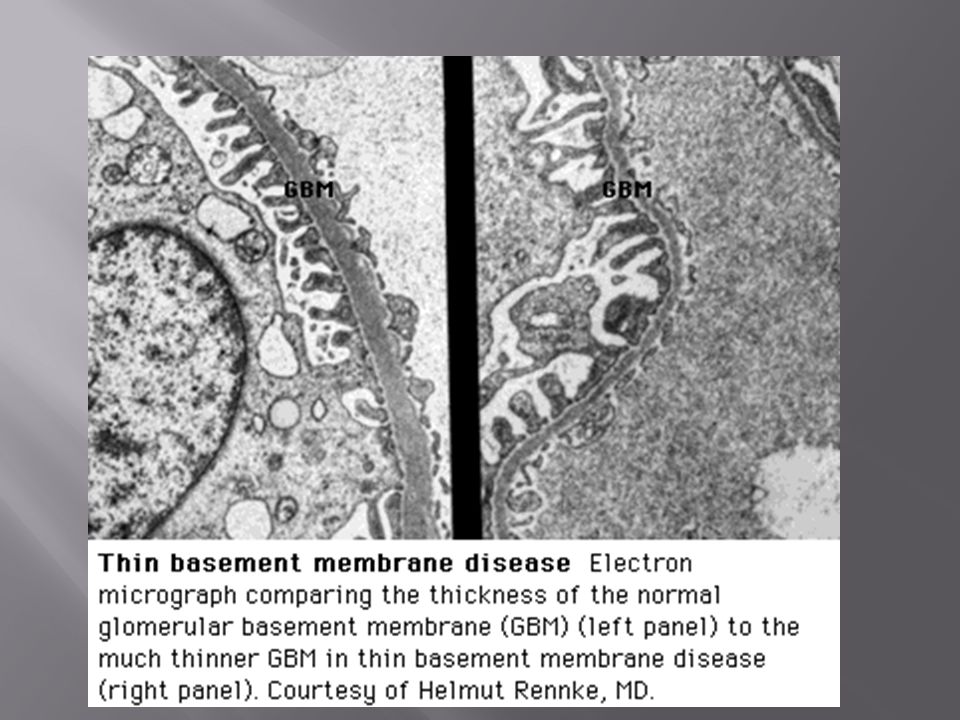
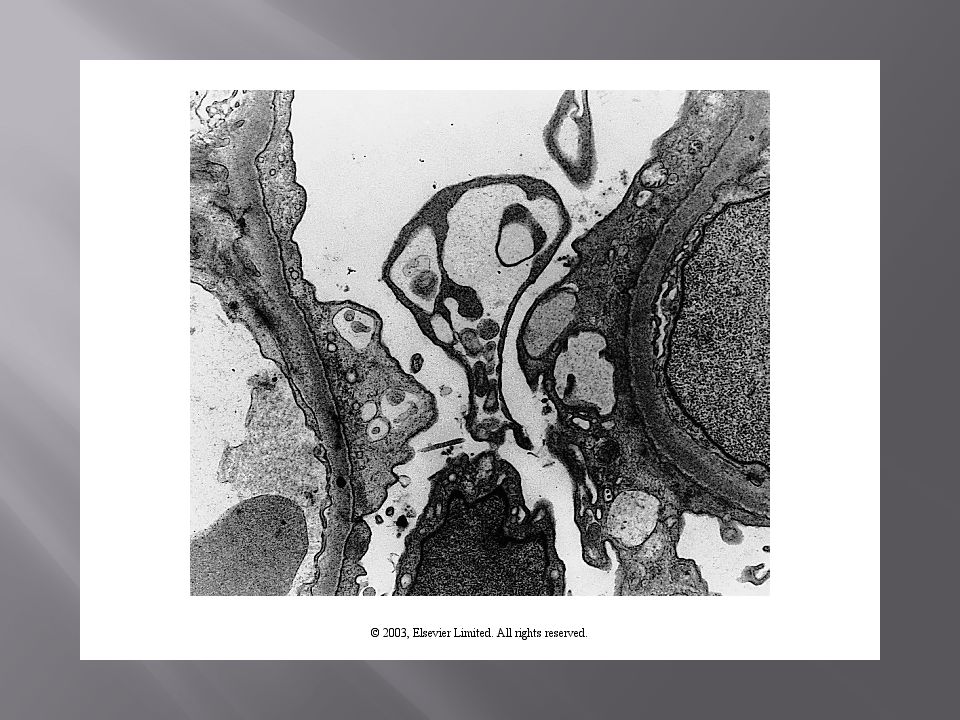
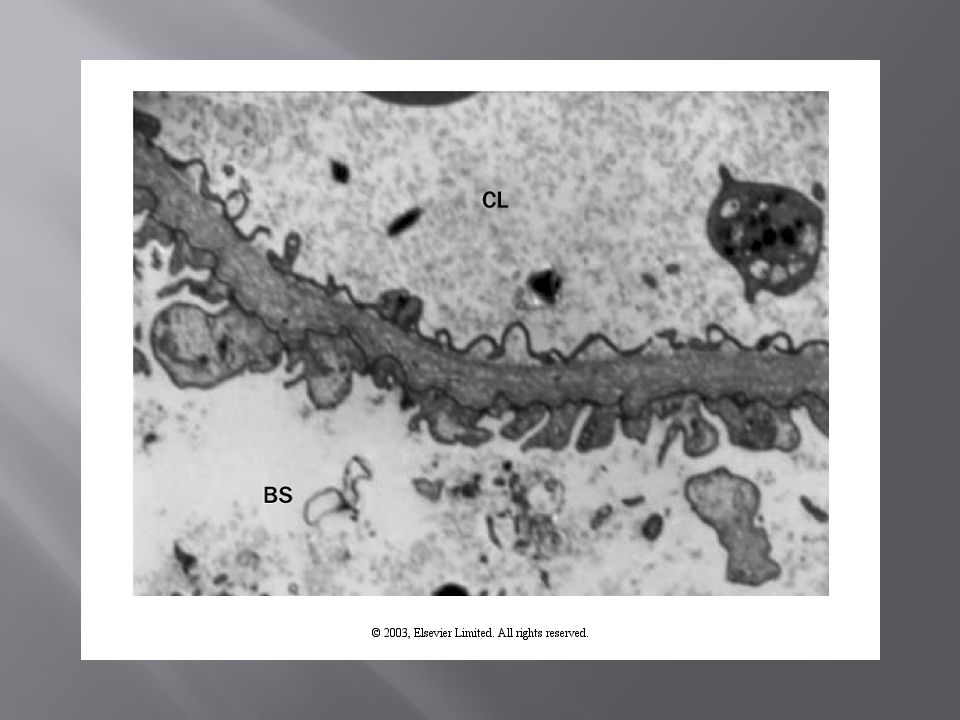
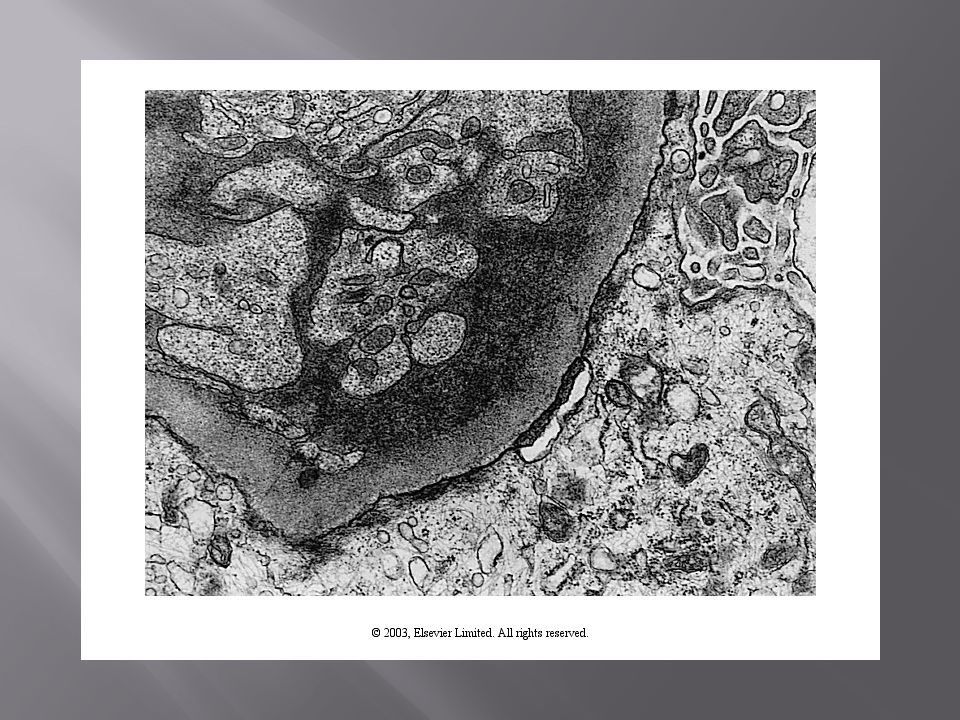
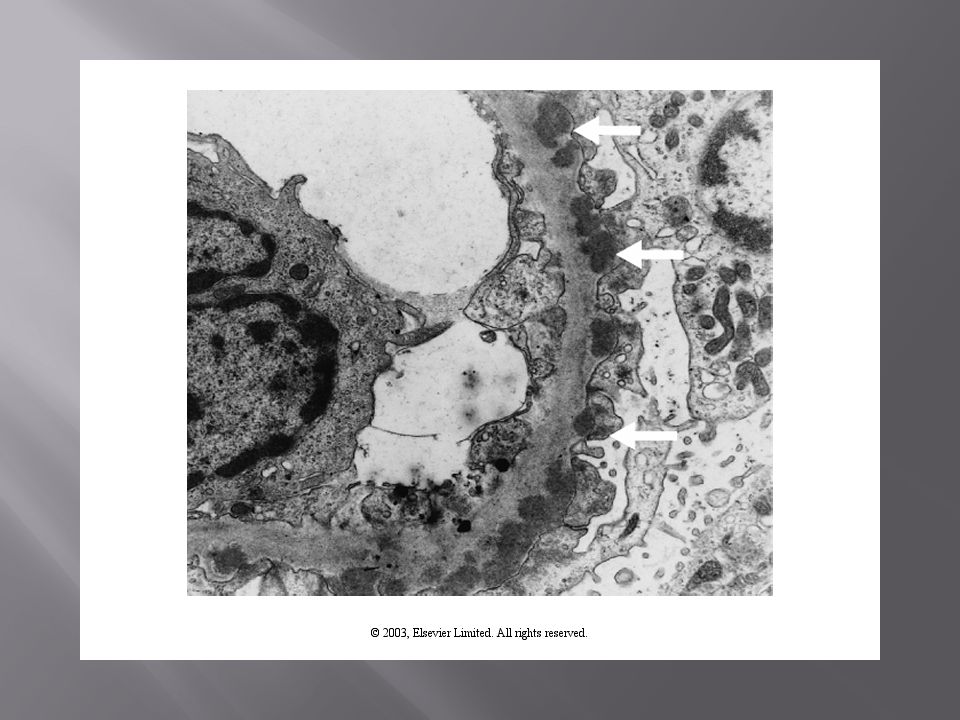
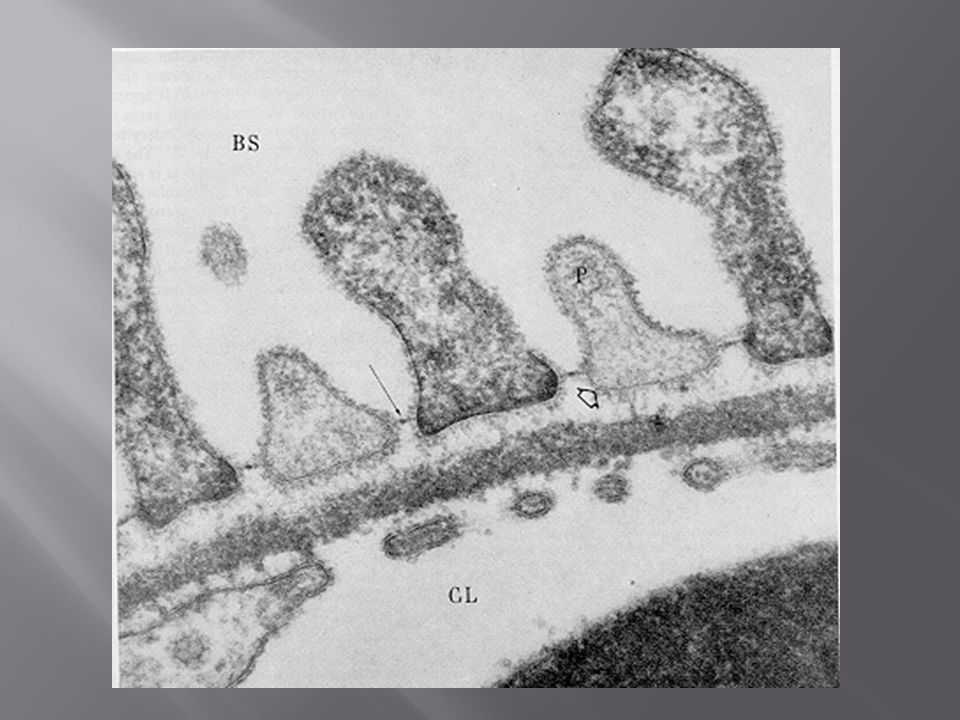
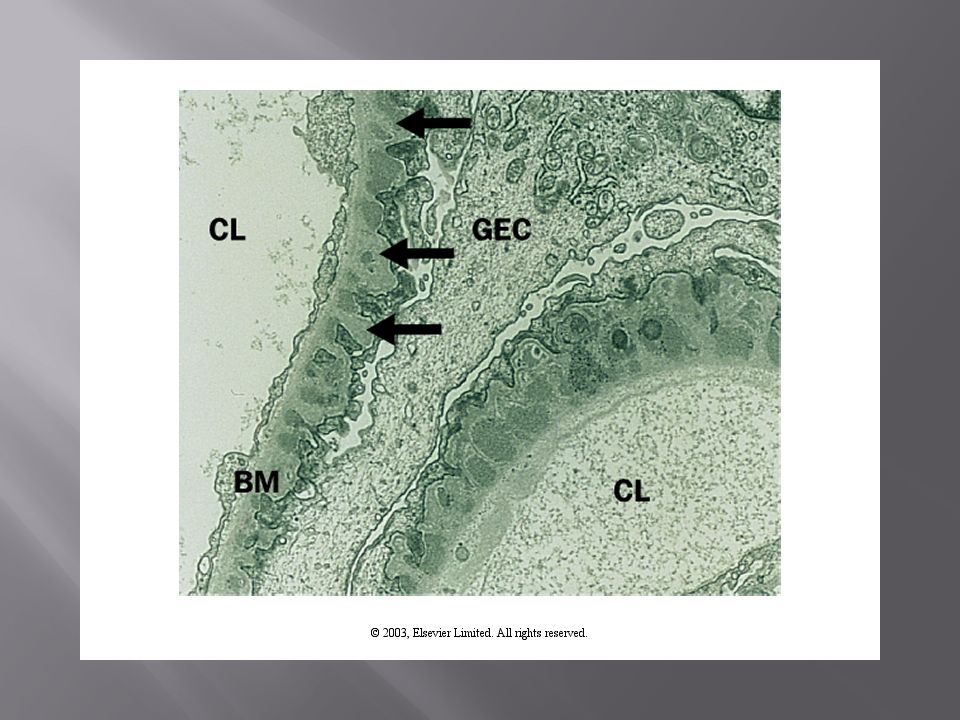
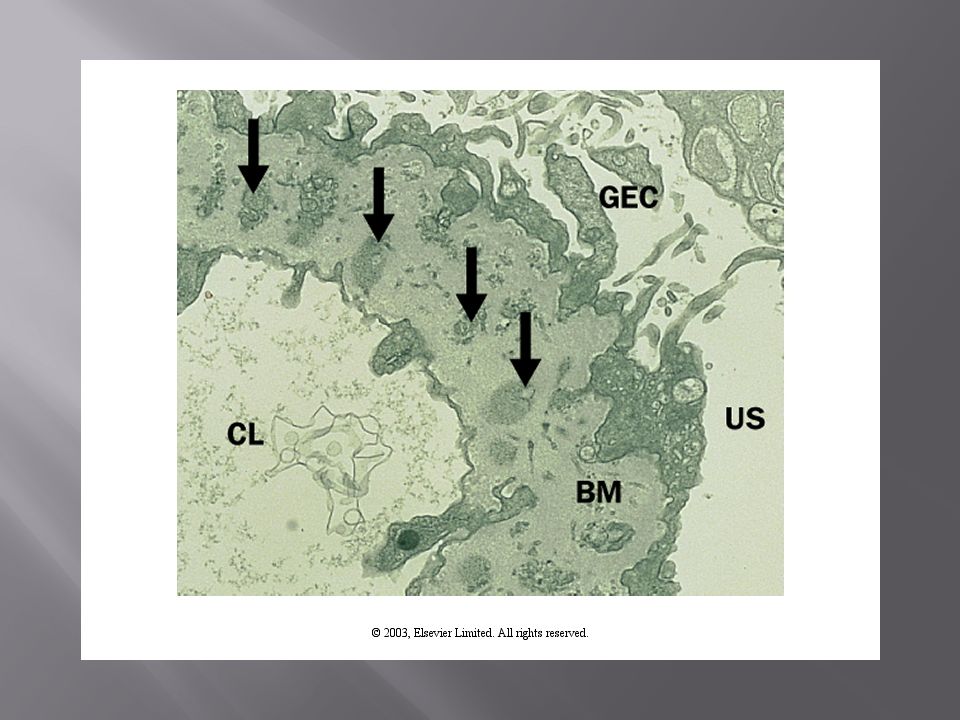
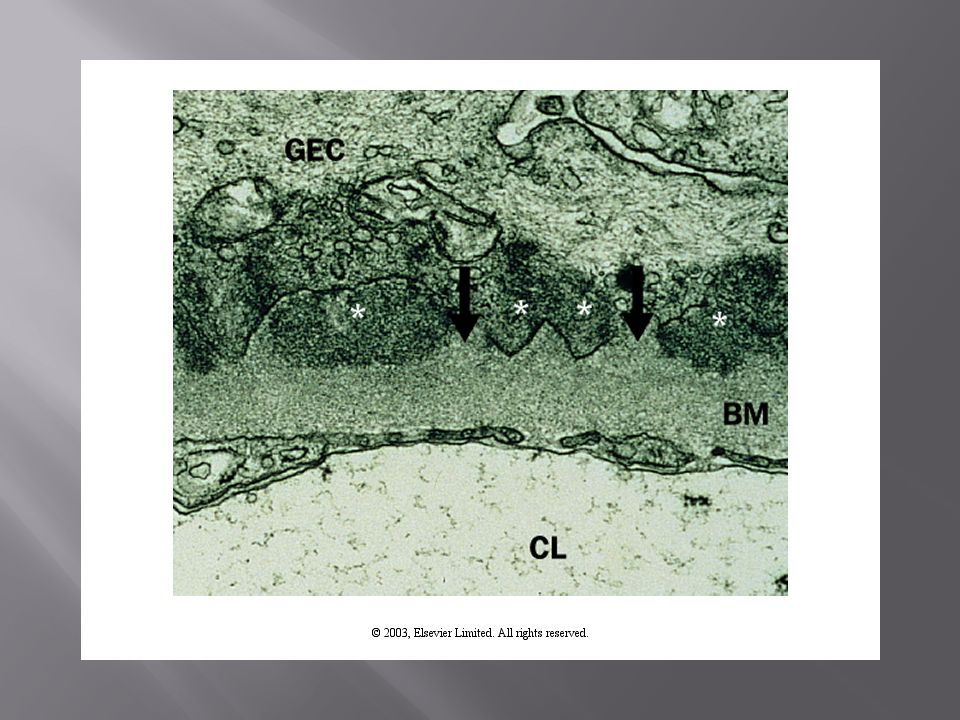
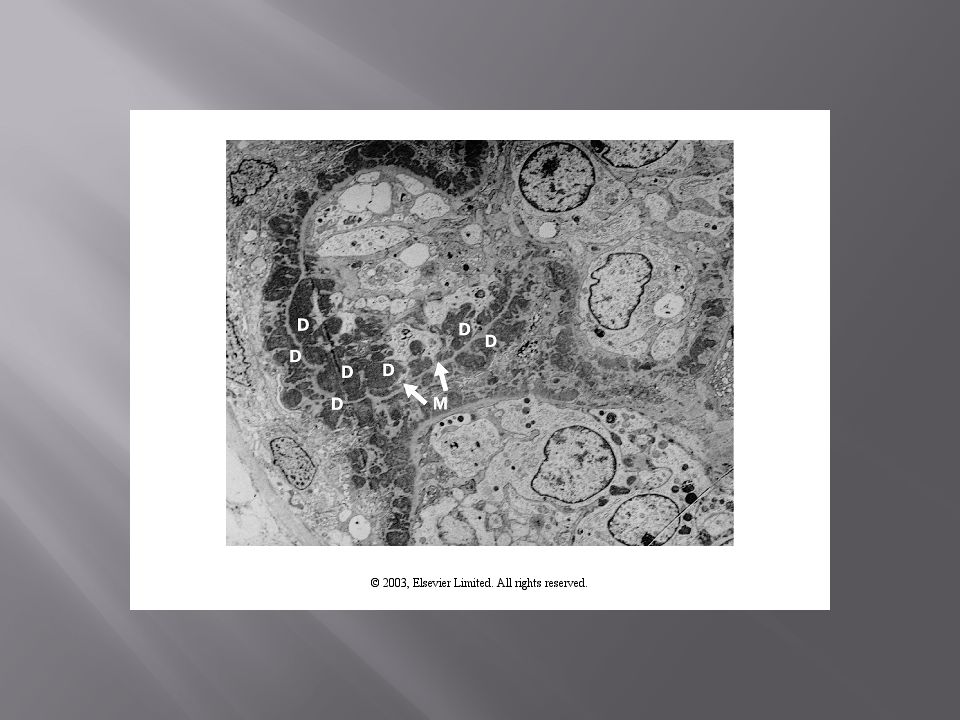
Electron Microscopy Anatomy of GBM (Alport’s, TBMD, MPGN II) Localization of deposits: Subepithelial (nephrotic) Subendothelial (nephritic) Mesangial (nephritic); secondary membranous Foot process fusion (nephrotic) Special deposits (Fibrillary, amyloidosis, LCDD)
 Localization of deposits: Subepithelial (nephrotic) Subendothelial (nephritic) Mesangial (nephritic); secondary membranous Foot process fusion (nephrotic) Special deposits (Fibrillary, amyloidosis, LCDD)")
57
Acute therapy (RPGN) Pulse steroids: ALL Cytoxan: Lupus; vasculitis; anti-GBM disease, IgA Plasmapheresis: TTP, Anti-GBM; Vaculitis Consolidation therapy MMF (Lupus) Azothiaprine (vasculitis, lupus) Acute/Chronic GN PO steroids Cyclosporin/tacrolimus MMF Rituximab; IVIG; Sirolimus
 Pulse steroids: ALL Cytoxan: Lupus; vasculitis; anti-GBM disease, IgA Plasmapheresis: TTP, Anti-GBM; Vaculitis Consolidation therapy MMF (Lupus) Azothiaprine (vasculitis, lupus) Acute/Chronic GN PO steroids Cyclosporin/tacrolimus MMF Rituximab; IVIG; Sirolimus")
59
64 y/o African American female with a history of “arthritis” presents for evaluation of progressive lower extremity edema of two weeks duration. She has no history of CKD, HTN, or DM. Her cancer screening is up to date (all negative/normal). She denies changes in her urination, SOB, fatigue, malaise, loss of appetite, fever, chills or night sweats. She has no personal or family history of renal disease. Her medications include a multivitamin and celecoxib. Her vitals are normalis totalis. Her exam was significant for lower extremity pitting edema to her waist bilaterally. Her labs reveal a serum creatinine of 2.1 mg/dL (up from 0.7 one month ago at her yearly PCM appointment). 24-hour urine protein was 5.6gm. Urine sediment revealed 10-20 WBCs with 3-4 WBC casts.
. She denies changes in her urination, SOB, fatigue, malaise, loss of appetite, fever, chills or night sweats. She has no personal or family history of renal disease. Her medications include a multivitamin and celecoxib. Her vitals are normalis totalis. Her exam was significant for lower extremity pitting edema to her waist bilaterally. Her labs reveal a serum creatinine of 2.1 mg/dL (up from 0.7 one month ago at her yearly PCM appointment). 24-hour urine protein was 5.6gm. Urine sediment revealed WBCs with 3-4 WBC casts..")
61
Additional questions? Differential Diagnosis? Additional diagnostic evaluation? Kidney Biopsy? Therapeutic intervention?

62
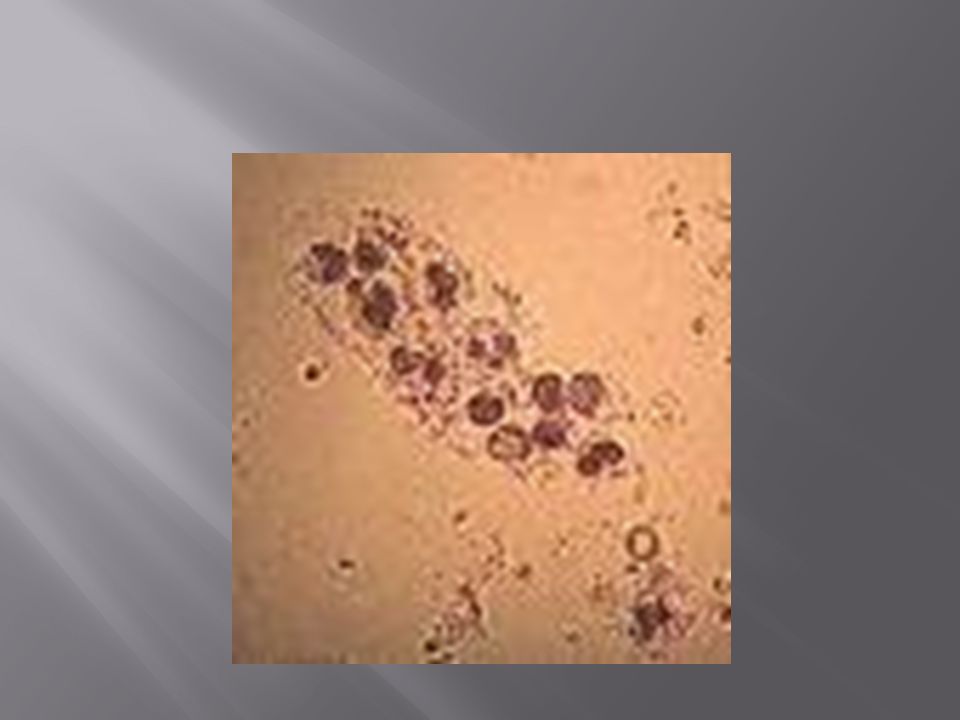
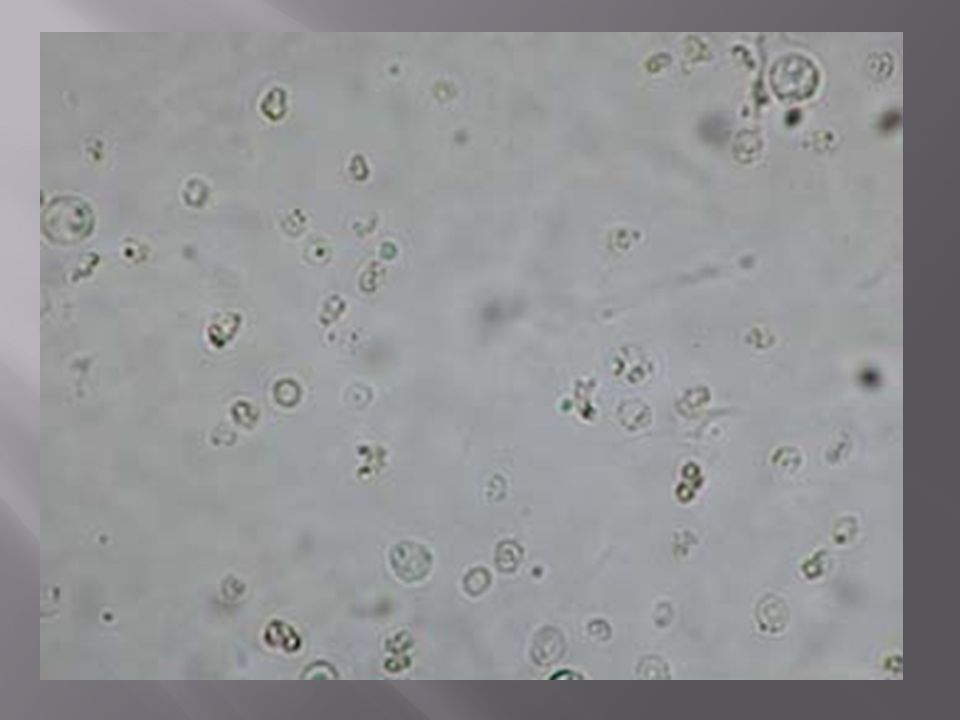
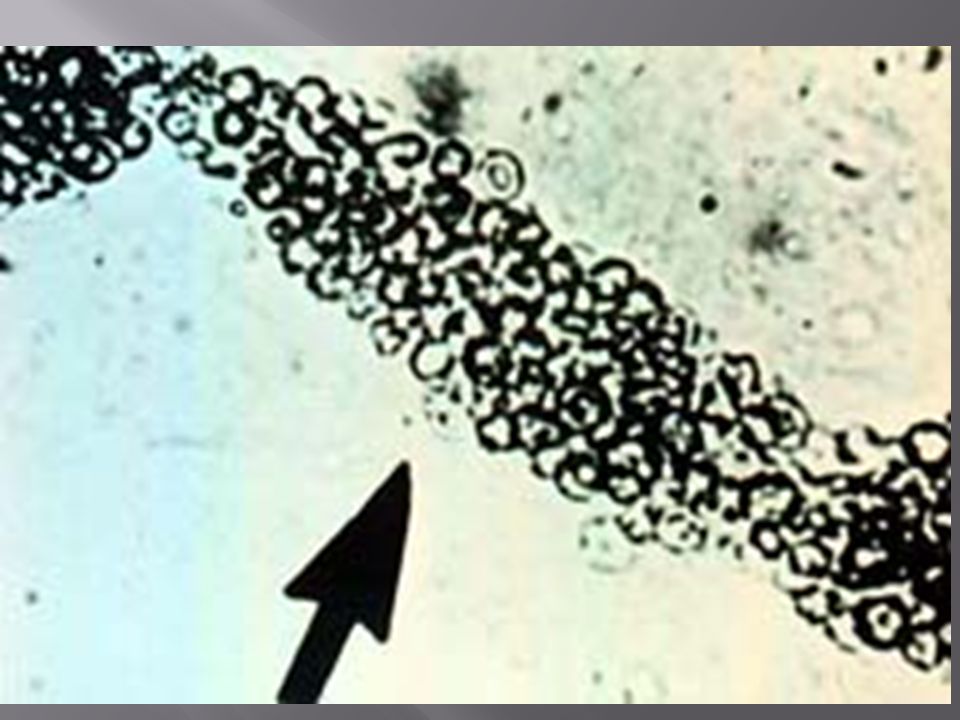
19 year old active duty male with no past medical history presents with the chief complaint “I was peeing blood doc. I mean straight up tomato soup.” Further questioning reveals that he had a sore throat 1 week ago. He first noted gross hematuria 2-3 days later which has gotten progressively better over the past few days and now it “looks normal.” He also reports 3/10 bilateral flank pain and some overall fatigue/malaise. He denies recent trauma, dysuria, urgency, frequency, nausea, vomiting, lower abdominal discomfort, fever/chills/night sweats, rashes, or skin lesions. He is not sexually active. He denies past gross hematuria but did have one episode of “dusky” urine a few years back. He denies past kidney problems but thinks that his mom “has always had a little blood in her urine but not so you can see it.” He takes no medications and denies taking dietary supplements. Vitals normalis totalis. There were no significant findings on exam. Labs reveal a serum Creatinine of 0.7mg/dL with no historical comparison. UA is negative for protein. Urine sediment reveals:

66
Differential Diagnosis? Additional diagnostic evaluations? Kidney Biopsy? Therapeutic intervention? Would a Cr of 2.0 and 4gm of proteinuria change the differential diagnosis, diagnostic work up, and/or therapy?

70
A 92 y/o Caucasian female presents with progressive fatigue, malaise, loss of appetite, and weight loss of 3 months duration. She also reports a chronic URI of 3 months duration unresponsive to 3 separate courses of different antibiotics. She denies hemoptysis, fever, chills, night sweats, nausea, vomiting, abdominal pain, early satiety, bloody/black BMs, HA, focal motor/sensory deficits, bony pain, change in urination. Her cancer screening is up to date (all normal/negative). She takes only a daily MVI and weakly Fosamax. She denies a personal or family history of kidney disease. She was mildly hypertensive. There were no significant findings on exam. Her labs reveal a serum Creatinine of 2.5 mg/dL up from a baseline of 0.9mg/dL 3 months ago. Her urine sediment revealed 30-50 RBCs phf (<10% dysmorphic) with occasional RBC cast. A 24-hour urine protein was 1.3gm. Her serum albumin was 2.2 and Hgb was 9.7.
. She takes only a daily MVI and weakly Fosamax. She denies a personal or family history of kidney disease. She was mildly hypertensive. There were no significant findings on exam. Her labs reveal a serum Creatinine of 2.5 mg/dL up from a baseline of 0.9mg/dL 3 months ago. Her urine sediment revealed RBCs phf (<10% dysmorphic) with occasional RBC cast. A 24-hour urine protein was 1.3gm. Her serum albumin was 2.2 and Hgb was 9.7. .")
72
Differential Diagnosis? Additional diagnostic evaluations? Kidney Biopsy? Therapeutic intervention?

79
A 55 y/o Caucasian male saw his PCM 2 weeks prior for progressive LE swelling of 2 weeks duration. He had no complaints and his ROS was negative. At the time his creatinine was noted to be at baseline 0.9mg/dL. His 24-hour urine protein was 13gm. His UA was negative for blood. LE dopler US was negative for clot. He presents for his nephrology consult 2 weeks later complaining of right sided loin/flank pain of 2 days duration with worsening LE edema, decreased appetite, early satiety, and feeling bloated. Exam reveals anasarca with no flank tenderness. Labs reveal a Cr of 1.4 mg/dL and an albumin of 1.5. His urine sediment reveals 20-30 non-dysmorphic RBCs phf.

80
Differential Diagnosis? Additional diagnostic evaluations? Kidney Biopsy? Therapeutic intervention?

86
A 22 y/o African American female admitted for bilateral pleural effusions and desaturation with ambulation after presenting with complaints of DOE during her runs. ROS is significant for increased fatigue prior to the DOE, arthralgias and some hair loss. Decreased BS at the bases with no m/r/g or distant heart sounds appreciated. Asymetry left lower extremity swelling of 1 week duration. Her labs reveal a creatinine of 1.3. Her spot urine protein/cr ratio demonstrates 1.5gm of protein. Hgb 9.7. Her urine sediment has 10-20 RBCs phf (20% dysmorphic) with no WBCs and no casts.
 with no WBCs and no casts..")
87
Additional diagnostic evaluations? Kidney Biopsy? Therapeutic intervention?

Similar presentations








![OS 214 [A]: Digestive and Excretory Lab 01.3: Lab Skills Session – Case 2 Dr. Sonia L. Chicano March 12, 2014 2 NIKA, ADA, GUDO.](/9/2477058/big_thumb.jpg "OS 214 [A]: Digestive and Excretory Lab 01.3: Lab Skills Session – Case 2 Dr. Sonia L. Chicano March 12, 2014 2 NIKA, ADA, GUDO.>")








 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")









 is the sudden onset of: – Haematuria (macroscopic/microscopic)>")