Download presentation
Presentation is loading. Please wait.

1
Renal System Case Scenario

2
Case Study Tia Smith is a 26 year old female patient who is 10 hours post-partum following an emergency C-section for twins. She was 33.5 weeks pregnant and had a difficult pregnancy with PIH (pregnancy induced hypertension) and frequent urinary tract infections. On admission Tia was diagnosed with HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) which necessitated immediate delivery of her babies. During the C-section Tia became hypovolemic resulting from massive hemorrhaging and required blood products and fluid replacements. Tia eventually developed hypovolemic shock and remained unstable for 2 hours. For the past nursing shift Tia has been hypotensive with blood pressures ranging from 59/37 to 95/52. Tia’s urinary output has been 2-12cc/hr of brown cloudy foul smelling urine. During your morning assessment you discover the following:
 and frequent urinary tract infections. On admission Tia was diagnosed with HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) which necessitated immediate delivery of her babies. During the C-section Tia became hypovolemic resulting from massive hemorrhaging and required blood products and fluid replacements. Tia eventually developed hypovolemic shock and remained unstable for 2 hours. For the past nursing shift Tia has been hypotensive with blood pressures ranging from 59/37 to 95/52. Tia’s urinary output has been 2-12cc/hr of brown cloudy foul smelling urine. During your morning assessment you discover the following:")
3
Case cont’d VS: T: 37.4 P: 125bpm R: 33 BP: 96/62
Respiratory: Chest is clear fine crackles heard throughout all lung fields, there is diminished A/E at the bottom of the R & L lobes CV: S1, S2 audible with pericardial friction, bounding rapid pulse Mental Status: drowsy and with assistance will orient slowly to PPT, pt c/o persistent hiccups Neurovascular: edema, skin cool & pale, bruises observed throughout extremities, skin turgor poor, bilateral decreased sensation in feet GI: pt c/o N&V Genitourinary: pt has foley catheter draining brown cloudy foul smelling urine at 2-12cc/hr Psychosocial: pt very emotional and crying at times because she cannot be with her newborn babies and is unable to breastfeed, she is concerned for their health, and does not understand how this happened to her

4
So… What is Tia’s diagnosis?
Acute Renal Failure

5
Definition Acute renal failure (ARF) is an abrupt and sudden reduction in renal function resulting in the inability to excrete metabolic wastes and maintain proper fluid & electrolyte balance It is usually associated with oliguria (urine output <30cc/hr or <400cc/day), although urine output may be normal or increased BUN & creatinine values are elevated
 is an abrupt and sudden reduction in renal function resulting in the inability to excrete metabolic wastes and maintain proper fluid & electrolyte balance. It is usually associated with oliguria (urine output <30cc/hr or <400cc/day), although urine output may be normal or increased. BUN & creatinine values are elevated.")
6
Statistics of ARF Frequency: condition develops in 5% of hospitalized patients and 0.5% patients require dialysis Elderly are at high risk Post-op patients Mortality: the mortality rate estimates vary from 25-90% Race: no racial predilection is recognized

7
Incidence of ARF 2-5% of all hospitalized patients
10-20% are critically ill Mortality Rate- 25% increases to 75% if complicated by other life threatening conditions

8
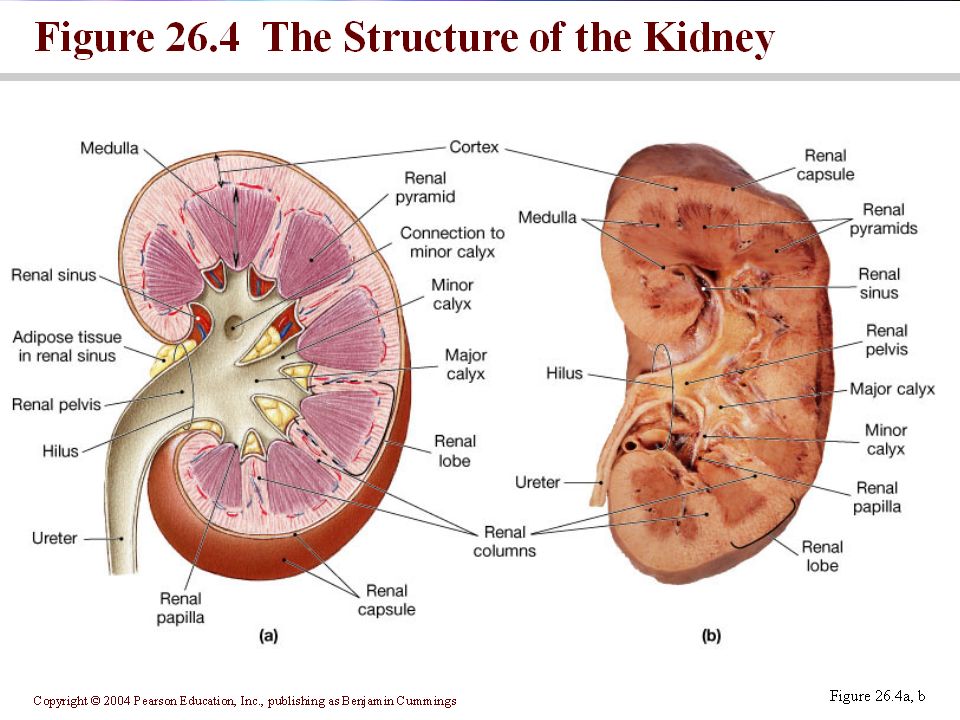
Anatomy of the Kidney

9
Composition of the Renal System

11
Vascular Structure of the Nephron
Renal artery Segmental artery Lobar artery Interlobar arteries Arcuate arteries Small interlobular arteries Smaller afferent arteries Capillary bed (Glomerulous) Efferent arteriole Peritubular capillaries Interlobular vein Arcuate vein Renal vein
 Efferent arteriole Peritubular capillaries Interlobular vein Arcuate vein Renal vein.")
12
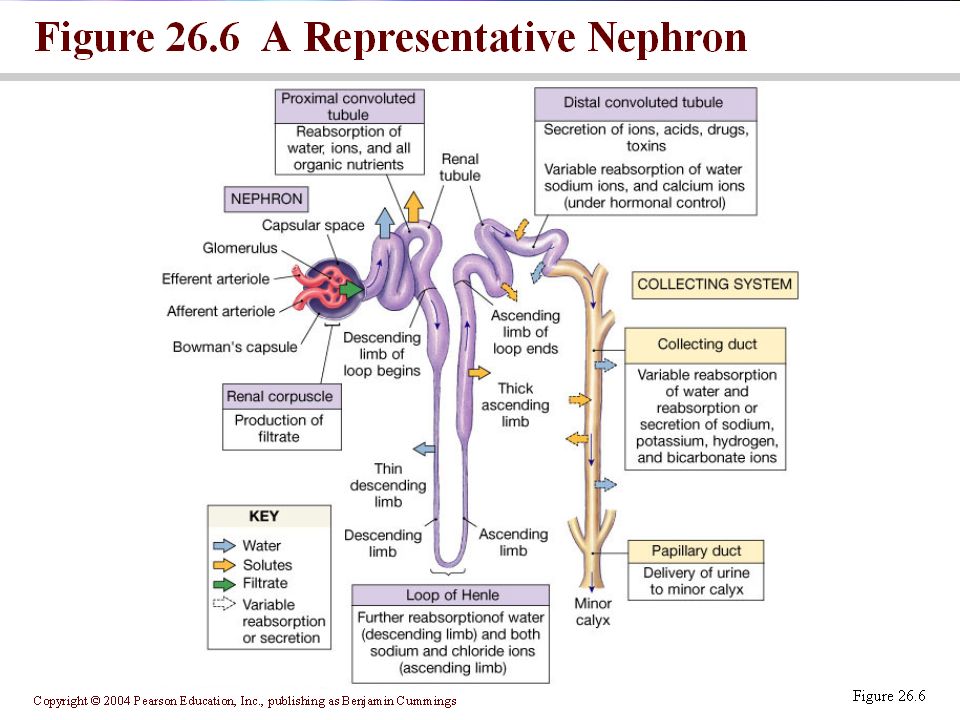
Nephron

14
Renal Corpuscle Initial filtering component of the nephron.
Consists of glomerulus (small network of capillaries enclosed in a Bowman’s capsule). Fluids from blood in the glomerulus is collected in the Bowman’s capsule to form ‘glomerulus filtrate. This is then further processed along the nephron to form urine.
. Fluids from blood in the glomerulus is collected in the Bowman’s capsule to form ‘glomerulus filtrate. This is then further processed along the nephron to form urine.")
15
Renal Corpuscle

16
Glomerular Capsule Not everything can pass through What fits through?
Na+, K+, Ca2+, Mg2+, Cl-, S04-, P042- Hc03 and H+ Nutrients such as monomers Wastes (nitrogenous wastes) Small hormones WATER!!!
 Small hormones. WATER!!!")
17
Glomerular Capsule What doesn’t fit through?? Cells Plasma proteins

18
Glomerular Filtration Rate (GFR)
The speed with which we pass our blood through our kidneys and filter it is proportional to how well we can clean our blood. Speed of filtration is the GFR In one minute both kidneys using all their nephrons can filter 125ml/min=180 liters/day!! We have on average 5 liters of blood in our bodies

19
Glomerular Filtration Rate
Amount of filtration changes with blood pressure Built in regulatory system

20
Glomerular Filtration Rate Pressures
Out of the Blood (into the capsule) Blood Pressure=60mm Hg Into the Blood (Out of the Capsule) Osmotic Pressure=32mm Hg Capsular hydrostatic pressure=18mm Hg
 Blood Pressure=60mm Hg. Into the Blood (Out of the Capsule) Osmotic Pressure=32mm Hg. Capsular hydrostatic pressure=18mm Hg.")
21
Glomerular Filtration Rate
Net pressure on fluids within the renal corpuscle. 60 mm Hg- (32 mm Hg + 18 mm Hg)= 10 mm Hg Therefore, in the renal corpuscle, the net force on fluids is OUT of the blood (into the capsule) and this is called the filtration pressure
= 10 mm Hg. Therefore, in the renal corpuscle, the net force on fluids is OUT of the blood (into the capsule) and this is called the filtration pressure.")
22
Specialized Cells of the Proximal Convoluted Tubule
Brush boarder cells Large surface area allowing for reabsorption of the filtrate into the blood stream Key Feature: Highly permeable to water & many solutes

23
Specialized Cells of the Descending Loop of Henle
Simple squamous epithelial cells that lack brush boarders Small surface area resulting in a decrease in the amount of filtrate reabsorbed into the blood stream Key feature: Highly permeable to water but not solutes

24
Ascending Loop of Henle
Similar to those of the PCT except fewer microvilli Key feature: Highly permeable to solutes (particularly sodium chloride), not permeable to water
, not permeable. to water.")
25
Juxtaglomerular Apparatus
Endocrine structure that secretes the hormones erythropoietin and renin Key Feature: Renin triggers angiotensin to turn into angiotensin I which turns to angiotensin II which constricts the walls of arteries to increase BP Erythopoietin stimulates the production of RBC when kidneys are exposed to low O2 concentrations

26
Renin-Angiotensin System

27
Specialized Cells of the Late Distal Convoluted Tubule
Cuboidal cells that fall into two distinct regions, principle cells and intercalated cells Key feature (principle cells): Permeable to water & solutes and regulated by hormones Key feature (intercalated cells): Involved in the secretion of H ions for acid/base balance
: Permeable to water & solutes and regulated by hormones. Key feature (intercalated cells): Involved in the secretion of H ions for acid/base balance.")
28
Specialized Cells of the Medullary Collecting Duct
Cuboidal cells Key feature: Hormonally regulated permeability to water and urea

29
Normal Kidney Function Summary
Maintain Homeostasis How does it do this….

30
10 Functions of the Kidney’s
Urine Formation: Formed in the nephrons through a complex three-step process: GF, tubular reabsorption, and tubular secretion Excretion of waste products: eliminates the body’s metabolic waste products (urea, creatinine, phosphates, sulfates) Regulation of electrolytes: volume of electrolytes excreted per day is exactly equal to the volume ingested Na – allows the kidney to regulate the volume of body fluids, dependent on aldosterone (fosters renal reabsorption of Na) K – kidneys are responsible for excreting more than 90% of total daily intake RETENTION OF K IS THE MOST LIFE-THREATENING EFFECT OF RENAL FAILURE
 Regulation of electrolytes: volume of electrolytes excreted per day is exactly equal to the volume ingested. Na – allows the kidney to regulate the volume of body fluids, dependent on aldosterone (fosters renal reabsorption of Na) K – kidneys are responsible for excreting more than 90% of total daily intake. RETENTION OF K IS THE MOST LIFE-THREATENING EFFECT OF RENAL FAILURE.")
31
Kidney Function con’td
Regulation of acid-base balance: elimination of sulphuric and phosphoric acid

32
Kidney function cont’d
Control of water balance: Normal ingestion of water daily is 1-2L and normally all but mL is excreted in the urine Osmolality: degree of dilution or concentration of urine (#particles dissolved/kg urine (glucose & proteins are osmotically active agents) Specific Gravity: measurement of the kidney’s ability to concentrate urine (weight of particles to the weight of distilled water) ADH: vasopressin – regulates water excretion and urine concentration in the tubule by varying the amount of water reabsorbed.
 Specific Gravity: measurement of the kidney’s ability to concentrate urine (weight of particles to the weight of distilled water) ADH: vasopressin – regulates water excretion and urine concentration in the tubule by varying the amount of water reabsorbed.")
33
Still talking about kidney function…
Control of blood pressure: BP monitored by the vasa recta. Juxtaglomerular cells, afferent arteriole, distal tubule, efferent arteriole Renal clearance: ability to clear solutes from plasma Dependent on… rate of filtration across the glomerulus, amount reabsorbed in the tubules, amount secreted into the tubules Regulation of red blood cell production: Erythropoeitin is released in response to decreased oxygen tension in renal blood flow. This stimulates the productions of RBCs (increases amount of hemoglobin available to carry oxygen)
")
34
Kidney function cont’d
Synthesis of vitamin D to active form: final conversion of vit D into active form to maintain Ca balance Secretion of prostaglandins: important in maintaining renal blood flow (PGE & PGI). They have a vasodilatory effect
. They have a vasodilatory effect.")
35
Timeline of Events ACUTE RENAL FAILURE EMERGENCY C-SECTION PIH HELLP
HEMORRHAGE HYPOVOLEMIC SHOCK HYPOVOLEMIA ACUTE RENAL FAILURE

36
HELLP SYNDROME A syndrome featuring a combination of "H" for hemolysis (breakage of red blood cells), "EL" for elevated liver enzymes, and "LP" for low platelet count (an essential blood clotting element). PREGNANCY COMPLICATION - occurring in 25% of pregnancies with toxemia or pre-eclampsia. Symptoms include- Shortness of breath H/A Dimmed vision Nausea Dizziness & Fainting Edema Pain in the upper abdomen
, EL for elevated liver enzymes, and LP for low platelet count (an essential blood clotting element). PREGNANCY COMPLICATION - occurring in 25% of pregnancies with toxemia or pre-eclampsia. Symptoms include- Shortness of breath. H/A. Dimmed vision. Nausea. Dizziness & Fainting. Edema. Pain in the upper abdomen.")
37
Effects of HELLP on Mom & Baby
Mothers with HELLP are at increased risk for: Liver rupture, DIC, abruptio placentae, and acute renal failure, stroke, seizure, ARD, pulmonary edema 1st order of tx is management of blood clotting issues Women with a hx of HELLP are considered at risk for future pregnancies After delivery, mothers vitals are CLOSELY monitored to observe for complications

38
NURSING PROCESS

39
Acute Renal Failure Definition:
“Acute Renal Failure is an abrupt reduction in renal function.”

40
Acute Renal Failure Three Stages to Renal Failure
1) Prerenal acute renal failure 2) Intrarenal acute renal failure 3) Postrenal acute renal failure
 Prerenal acute renal failure. 2) Intrarenal acute renal failure. 3) Postrenal acute renal failure.")
41
Pathophysiology ARF may occur in 3 clinical settings:
As an adaptive response to severe volume depletion and hypotension, with structurally and functionally intact nephrons (Prerenal) In response to cytotoxic or ischemic insults to the kidney, with structural and functional damage (Intrinsic or Intrarenal) Obstruction to the passage of urine (Postrenal)
 In response to cytotoxic or ischemic insults to the kidney, with structural and functional damage (Intrinsic or Intrarenal) Obstruction to the passage of urine (Postrenal)")
42
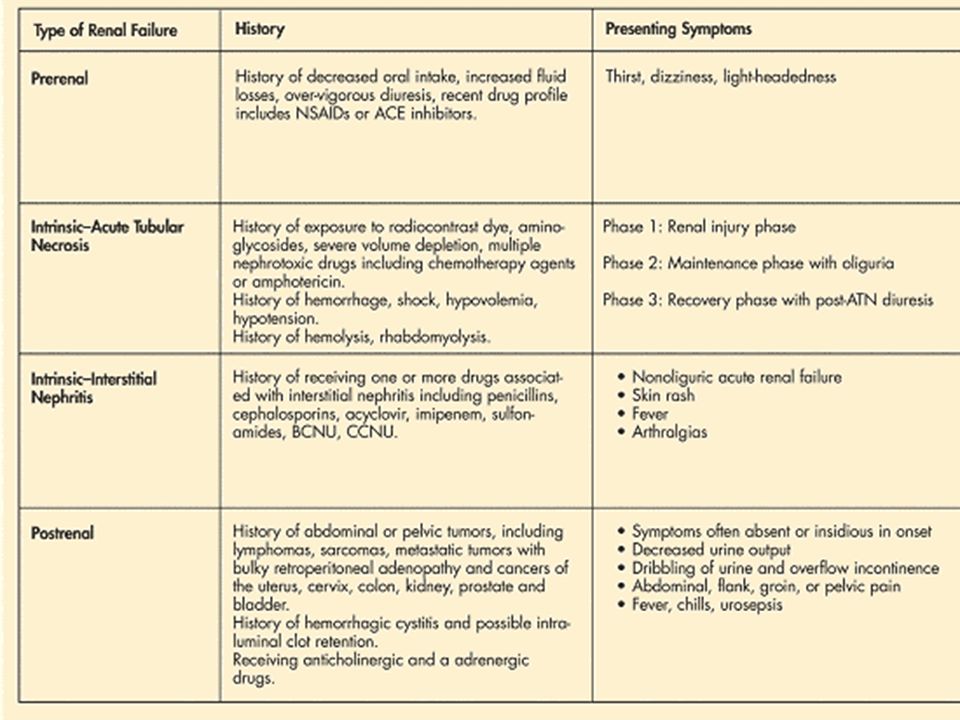
Acute Renal Failure: Classification

43
Prerenal Acute Renal Failure
60-70% of patients with Acute Renal Failure are Prerenal. GFR declines because of the decrease in filtration pressure. Poor perfusion results from renal vasoconstriction, hypotension, hypovolemia Failure to restore blood volume or blood pressure may cause acute tubular necrosis or acute cortical necrosis.

44
Prerenal acute renal failure
It is caused by impaired blood flow as a result of intravascular depletion, which leads to decreased effective circulating volume to the kidneys In patients with prerenal ARF, the parenchymal is undamaged, and the kidneys respond as if volume depletion has occurred.

45
Prerenal ARF Causes include:
Secondary to renal hypoperfusion which occurs in setting of extracellular fluid loss Diarrhea Vomiting Diuretics Impaired/inadequate cardiac output Drugs NSAIDs ACE Inhibitors Hypovolemia Hemorrhage Renal vasoconstriction

46
Intrarenal ARF May result from: Acute tubular necrosis (ATN), cortical necrosis, acute glomerulonephritis, drug allergy, . ATN caused by ischemia occurs most commonly after surgery (40%-50%) ATN also caused by sepsis, severe burns, or trauma Can be caused by antibiotics
 ATN also caused by sepsis, severe burns, or trauma. Can be caused by antibiotics.")
47
Intrinsic acute renal failure
Is the result of actual parenchymal damage to the glomeruli or kidney tubules A physiologic hallmark is failure to maximally concentrate urine Is divided into 4 categories: Acute tubular disease Glomerular disease Vascular disease Interstitial disease

48
Intrinsic ARF Acute Tubular Necrosis Glomerulonephritis
most common type of ARF, a more ischemic insult to the kidneys, usually induced by ischemia or toxins Caused by: Burns, and crush injuries – myoglobin & hemoglobin are liberated causing renal toxicity or ischemia Drugs – NSAIDs, ACE inhibitors, aminoglycosides Infections Nephrotoxic agents – contrast agent Glomerulonephritis uncommon cause, most associated with CRF Can be a primary disorder or can occur secondary to systemic disease Systemic lupus erythematosus

49
Intrinsic ARF Vascular Disease Acute Interstitial Nephritis
Can occur on microvascular and macrovascular Caused by: Microvascular Hemolytic anemia ARF secondary to small vessel thrombosis or occlusion Macrovascular Suspected in elderly Renal artery stenosis or thrombosis Atheroembolism secondary to atrial fibrillation and aortic disease Acute Interstitial Nephritis Interstitial disturbance that leads to ARF Allergic reaction to drugs

50
Postrenal acute renal failure
Is rare and occurs with urinary tract obstruction that affects the kidneys bilaterally Pressure rises in the kidney tubules, eventually the GFR decreases

51
Postrenal ARF Causes include:
Bladder tract obstruction Prostatic hypertrophy Catheters Neurogenic bladder Postrenal causes are typically reversible

53
Clinical Manifestations of ARF
Cardiovascular Arrhythmias BP, N, high or low Anemia P, rapid, bounding, or N Pericardial-type chest pain Respiratory Dyspnea Crackles Tachypnea Kussmaul’s respirations Mental Status Lethargy Tremors Memory loss Confusion Musculoskeletal Muscle spasms Weakness Genitourinary Oliguria Anuria abN urine colour, clarity, smell GI Moist tongue & increased saliva Dry tongue & mucous membranes N&V Integumentary Moist, warm skin & pitting edema Decreased skin turgor bruises Pallor Thin, brittle hair & nails

54
Nursing Care Plan Fluid volume deficit related to hemorrhage (hypovolemic shock) Priority to restore fluid balance and circulation The patient will: show stable vital signs have adequate urine output >30cc/hr have strong peripheral pulses indicating tissue perfusion display LOC normal for patient

55
Nursing Care Plan Rationales Interventions
Early intervention can prevent progression of hypovolemia to hypovolemic shock that may result in renal damage S&S correlate with the approximate percentage of volume loss Medullary vasomotor center stimulation via the baroreceptor reflex ADH Foley catheter facilitates monitoring of urine output Shock pt hemodynamically unstable with compromised compensatory mechanisms, volume admin may cause fld overload Interventions Bleeding reduction, fluid resuscitation, blood product administration, IV therapy Monitor VS q2h Monitor weight daily Skin & tongue turgor Monitor and document I&O Monitor CBC, ABG, urinalysis, ECG

56
Nursing Care Plan Electrolyte imbalance related to decreased electrolyte excretion, and metabolic acidosis Priority to prevent complications of electrolyte imbalance Within 24h of admission and then continuously, the pt will: Maintain serum electrolyte levels within acceptable limits Have normal sinus rhythm

57
Nursing Care Plan Interventions Rationales
Monitor & document electrolyte levels q8-12h, especially: K+, P, Ca, Mg Monitor ABG Monitor ECG especially: High tented T waves, prolonged PR interval or widened QRS complex Limit dietary & drug intake of potassium Rationales Kidneys’ ability to regulate electrolyte excretion & reabsorption may result in high K+ & P, low Ca, & high/low Mg levels. ARF causes metabolic acidosis which may increase the release of K+ from cells in exchange for H+ ions Electrolyte abN can trigger arrhythmias & cardiac arrest When kidneys cannot excrete K+, excess intake can increase serum K+ to dangerous levels

58
Nursing Care Plan Knowledge deficit of acute renal failure related to lack of exposure to information on management of complex condition Priority to provide in depth information on acute renal failure Upon discharge the patient will: Be able to identify signs and symptoms to report to nurse or physician Commitment to comply with treatments, including dialysis, dietary modifications, and activity restrictions

59
Nursing Care Plan Interventions Rationales
Provide as appropriate information on the severity of ARF & dialysis Stages of ARF Medications including action and adverse effects S&S Procedures such as dialysis including schedule and adverse effects Dietary modifications including limitations of proteins (catabolism), electrolytes and fluids Rest and activity restrictions Rationales The patient and family need assistance, explanation, and support during this time. Teaching may decrease anxiety and fear, and enhance recovery to patient and family members. Continued assessment of the patient for complications of ARF and of its precipitating cause is essential.
, electrolytes and fluids. Rest and activity restrictions. Rationales. The patient and family need assistance, explanation, and support during this time. Teaching may decrease anxiety and fear, and enhance recovery to patient and family members. Continued assessment of the patient for complications of ARF and of its precipitating cause is essential.")
60
Measuring kidney function
Diagnostic Testing Measuring kidney function

61
Diagnostic Tools Urinalysis Blood Work X-ray
Urogram (intravenious pyelogram) Ultrasound Doppler Scopes Biopsies
 Ultrasound. Doppler. Scopes. Biopsies.")
62
The Urinalysis Also called a routine UA (urinalysis)- gross and microscopic examination of urine to determine pH, gravity and substance Gross Assessment- appearance and odor of the urine Microscopic Assessment- bacteria, RBC, WBC, crystals, casts. Normal Findings of Urinalysis: pH Gravity to 1.030 Protein- Negative RBC/WBC- Negative Glucose- Negative Ketones- Negative Nitrates- Negative

63
The Urinalysis Normal Abnormal
inorganic material such as NA+, Cl-, Mg+, SO4-, PO4-, and NH4+ and organic materials such as urea, creatinine, and uric acid in the urine. Abnormal RBCs, WBCs, bacteria protein, glucose, ketones Urinalysis involves evaluation of color, turbidity, protein, pH, specific gravity, sediment Presence of bacteria, RBCs, WBCs, casts or crystals in the urine sediment may indicate a renal disorder.

64
Assessing Urine The first morning void is considered ideal as it has the greatest concentration and lowest pH (maximizing the ability to detect formed elements). A regular void (with appropriate washing of the genitals) is usually satisfactory. A midstream or catheterized specimen is more appropriate for culture and bacteria count.
. A regular void (with appropriate washing of the genitals) is usually satisfactory. A midstream or catheterized specimen is more appropriate for culture and bacteria count.")
65
Assessing Blood Why assess the blood? Electrolyte balance
Acid-base homeostasis Regulates serum concentrations of BUN and Creatinine Produce erythropoietin

66
BUN, creatinine, creatinine clearance presentation by students

67
Normal Blood and Serum Lab Values
Sodium mEq/L Potassium mEq/L Chloride mEq/L BUN mg/dL Creatinine umol/L (Female) umol/L (Male) Phosphorus mmol/L Calcium mmol/L Magnesium mg/dL Hemoglobin g/L (Female) g/L (Male)
 umol/L (Male) Phosphorus mmol/L. Calcium mmol/L. Magnesium mg/dL. Hemoglobin g/L (Female) g/L (Male)")
68
Lab Tests for Renal Function: Blood Tests
Blood Urea Nitrogen Measures the concentration of urea in the blood Urea is formed from protein metabolism and is elevated when glomerular filtration is reduced BUN rises in states of dehydration and acute chronic renal failure because passage through tubules is slowed Serum Creatinine Level Should be a stable value When creatinine levels rise and accumulate in the plasma: Double renal function is about half of Normal Tripled ~ 75% of RF is lost Represents a decrease in GRF

69
Estimating GFR and Creatinine Clearance
GFR- Filtration rate/min at the glomerulus. 170 x Serum Creatinine concentration^-0.999 X age^-0.176 X (if female) X 1.18 (if race is African) X blood urea nitrogen concentration^-0.17 X serum albumin concentration^-0.318 = GRF in Adults Creatinine Clearance- The clearance rate in mL/min of the waste product creatinine. 0.55 x Length/ Serum Creatinine
 X 1.18 (if race is African) X blood urea nitrogen concentration^ X serum albumin concentration^ = GRF in Adults. Creatinine Clearance- The clearance rate in mL/min of the waste product creatinine x Length/ Serum Creatinine.")
70
INTERVENTION

71
Medications for ARF Pharmacologic treatment of ARF has been attempted on an empirical basis, with varying success rates. Several promising experimental therapies in animal models are awaiting human trials It is critical to adjust (decrease or discontinue) medication dosages for patient in acute renal failure. Administering the average dose to patient in renal failure can kill a patient.
 medication dosages for patient in acute renal failure. Administering the average dose to patient in renal failure can kill a patient.")
72
Medications for ARF continued
Immediate goal is to retain fluid volume deficit through use of blood products and crystalloids Normal Saline (0.9% Na) – only one that is compatible with blood transfusions Restores fluid loss Provides electrolytes resembling those of plasma Packed RBC To increase blood volume To restore blood to kidneys
 – only one that is compatible with blood transfusions. Restores fluid loss. Provides electrolytes resembling those of plasma. Packed RBC. To increase blood volume. To restore blood to kidneys.")
73
Medications for ARF continued
Diuretics Furosemide (Lasix) only given with severe fluid overload Increases excretion of water by interfering with chloride-binding cotransport system, which, in turn, inhibits sodium and chloride reabsorption in the thick ascending loop of Henle and the distal renal tubule Adult dose: mg PO/IV once; repeat 6-8h prn or dose may be increased by mg no sooner than 6- 8h after previous dose until desired effect Nursing Assessments: Watch for hypokalemia, assess BP before and during therapy can cause hypotension
 only given with severe fluid overload. Increases excretion of water by interfering with chloride-binding cotransport system, which, in turn, inhibits sodium and chloride reabsorption in the thick ascending loop of Henle and the distal renal tubule. Adult dose: mg PO/IV once; repeat 6-8h prn or dose may be increased by mg no sooner than 6- 8h after previous dose until desired effect. Nursing Assessments: Watch for hypokalemia, assess BP before and during therapy can cause hypotension.")
74
Medications for ARF continued
Vasodilators Dopamine In small doses causes selective dilatation of the renal vasculature, enhancing renal perfusion. Reduces sodium absorption, thereby decreasing the energy requirement of the tubules. This enhances urine flow, which, in turn, helps prevent tubular cast obstruction. Adult dose: 2-5 mcg/kg/min Nursing Assessments: Monitor BP during administration, stop infusion if BP drops 30mm Hg, Monitor I&O

75
Medications for ARF continued
Alkalinizer Sodium Bicarbonate Increases plasma bicarbonate, which buffers Hydrogen ion concentration; reverses acidosis Adult Dose: Initial dose IV bolus 1 mEq/kg, then infuse 2-5 mEq/kg over 4-8 hr depending on CO2, pH Dilute with equal amounts of NS, 2-5 mEq/kg Nursing assessments: Assess resp. and pulse rate, rhythm, depth, lung sounds, monitor I&O, electrolytes, blood pH, PO2, HCO3, monitor urine pH, and UO during beginning of treatment, monitor for alkalosis, monitor ABGs and blood studies

76
13 have passed and now Tia is diagnosed with…
Chronic Renal Failure 13 years have passed Tia is now 39 years of age and has been experiencing declining renal function over the past 13 years. Tia has lost 15lbs on her already small frame, she feels generally ill most of the time with frequent N&V, she suffers from fatigue, muscle twitching & cramps decreased sensation in her hands and feet and generalized puritus. The Physician has diagnosed Tia with ESRD and has determined that long term dialysis will be required.

77
Chronic Renal Failure ESRF

78
Definition Also known as End-Stage Renal Failure (ESRF), is a progressive deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails, resulting in uremia (retention of urea and other nitrogenous wastes in the blood). decreased kidney glomerular filtration rate (GFR) of <60 mL/min/1.73 m2 for 3 or more months
, is a progressive deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails, resulting in uremia (retention of urea and other nitrogenous wastes in the blood). decreased kidney glomerular filtration rate (GFR) of <60 mL/min/1.73 m2 for 3 or more months.")
79
Alterations-Acute Renal Failure
Renal Impairment 50% of Normal GFR- 50mL/Min Serum Creatinine: less than 2 mg/dL BUN: High normal Renal Insufficiency 25% of Normal GFR 25-40mL/min Serum Creatinine: mg/dL (mildly elevated) BUN: Mild azotemia Renal Failure < 20% of renal fcn remains GFR < 25mL/min Serum Creatinine: > than 3.0 mg/dL Electrolyte imbalances End stage renal disease (ESRD) < 10% of renal fcn remains GFR < 10 mL/min Creatinine and BUN: marked increase Acidosis
 BUN: Mild azotemia. Renal Failure. < 20% of renal fcn remains. GFR < 25mL/min. Serum Creatinine: > than 3.0 mg/dL. Electrolyte imbalances. End stage renal disease (ESRD) < 10% of renal fcn remains. GFR < 10 mL/min. Creatinine and BUN: marked increase. Acidosis.")
80
Statistics In the U.S. The US Renal Data System (USRDS) has shown a dramatic increase in patients with CRF who require chronic dialysis or transplantation. In 1999, there were 340,000 such patients, but, by 2010, this number is projected to reach 651,000. Internationally: The incidence rates of end-stage renal disease (ESRD) have increased steadily internationally since The United States has the highest incident rate of ESRD, followed by Japan. Japan has the highest prevalence per million population, with the United States taking second place.
 has shown a dramatic increase in patients with CRF who require chronic dialysis or transplantation. In 1999, there were 340,000 such patients, but, by 2010, this number is projected to reach 651,000. Internationally: The incidence rates of end-stage renal disease (ESRD) have increased steadily internationally since The United States has the highest incident rate of ESRD, followed by Japan. Japan has the highest prevalence per million population, with the United States taking second place.")
81
Statistics Cont’d Mortality /Morbidity: CRF is a major cause of morbidity and mortality, particularly at the later stages. The 5-year survival rate for a patient undergoing chronic dialysis is approximately 35%. This is approximately 25% in patients with diabetes. The most common cause of death in the dialysis population is cardiovascular disease. Race: Affects all races

82
Chronic Renal Failure “Slow, progressive, (months to years) irreversible loss of renal function.”
 irreversible loss of renal function.")
83
Pathophysiology As renal function declines, the end products of protein metabolism (which are normally excreted in the urine), accumulate in the blood. Uremia develops and adversely effects every system in the body. The greater the buildup of waste products, the more severe the symptoms. Approximately 1 million nephrons are present in each kidney, each contributing to the total GFR. Regardless of the etiology of renal injury, with progressive destruction of nephrons, the kidney has an innate ability to maintain GFR by hyperfiltration and compensatory hypertrophy of the remaining healthy nephrons. This nephron adaptability allows for continued normal clearance of plasma solutes such that substances such as urea and creatinine start to show significant increases in plasma levels only after total GFR has decreased to 50%, when the renal reserve has been exhausted. The plasma creatinine value will double with a 50% reduction in GFR.
, accumulate in the blood. Uremia develops and adversely effects every system in the body. The greater the buildup of waste products, the more severe the symptoms. Approximately 1 million nephrons are present in each kidney, each contributing to the total GFR. Regardless of the etiology of renal injury, with progressive destruction of nephrons, the kidney has an innate ability to maintain GFR by hyperfiltration and compensatory hypertrophy of the remaining healthy nephrons. This nephron adaptability allows for continued normal clearance of plasma solutes such that substances such as urea and creatinine start to show significant increases in plasma levels only after total GFR has decreased to 50%, when the renal reserve has been exhausted. The plasma creatinine value will double with a 50% reduction in GFR.")
84
Stages of Chronic Renal Disease
3 stages in nephron function Stage 1: Reduced Renal Reserve Characterized by a 40%-75% loss of nephron funtion. The patient is usually asymptomatic because the remaining nephrons are able to carry out normal function of the kidney

85
Stage 2 of Renal Disease Stage 2: Renal Insufficiency
Occurs when 75%-90% of nephron function is lost. At this point, the serum creatinine and BUN rise, the kidney loses its ability to concentrate urine and anemia develops. The patient may report polyuria and nocturia

86
Stage 3 of Renal Disease Stage 3: End-Stage Renal Disease
The final stage, occurs when there is less than 10% of nephron function remaining. All normal regulatory, excretory, and hormonal functions of the kidneys are severely impaired. ESRD is evidenced by elevated creatinine and BUN levels as well as electrolyte imbalances. Dialysis is usually indicated at this point.

87
Glomular Filtration Rate
GFR: a Kidney function test in which results can be determined from amount of ultrafiltrate formed by plasma flowing through the glomeruli of the kidney. As glomular filtration decreases, the serum creatinine and BUN levels increase.

88
Causes Type 1 and type 2 diabetes mellitus cause a condition called diabetic nephropathy, which is the leading cause of kidney disease in the United States. High Blood Pressure (hypertension), if not controlled, can damage the kidneys over time. Glomerulonephritis is the inflammation and damage of the filtration system of the kidney and can cause kidney failure. Postinfectious conditions and Lupus are among the many causes of glomerulonephritis.
, if not controlled, can damage the kidneys over time. Glomerulonephritis is the inflammation and damage of the filtration system of the kidney and can cause kidney failure. Postinfectious conditions and Lupus are among the many causes of glomerulonephritis.")
89
More Causes Polycystic Kidney Disease is an example of a hereditary cause of chronic kidney disease wherein both kidneys have multiple cysts Use of analgesics such as acetaminophen (Tylenol) and ibuprophen regularly over long durations of time can cause analgesic nephropathy, another cause of kidney disease. Certain other medications can also damage the kidneys. Clogging and hardening of the arteries (atherosclerosis) leading to the kidneys causes a condition called ischemic nephropathy, which is another cause of progressive kidney damage. Obstruction of the flow of urine such as by stones, an enlarged prostate, strictures (narrowings), or cancers may also cause kidney disease
 and ibuprophen regularly over long durations of time can cause analgesic nephropathy, another cause of kidney disease. Certain other medications can also damage the kidneys. Clogging and hardening of the arteries (atherosclerosis) leading to the kidneys causes a condition called ischemic nephropathy, which is another cause of progressive kidney damage. Obstruction of the flow of urine such as by stones, an enlarged prostate, strictures (narrowings), or cancers may also cause kidney disease.")
90
Clinical Manifestation
Patients with CRF stage 3 or lower (GFR >30 mL/min) generally are asymptomatic and do not experience clinically evident disturbances in water or electrolyte balance or endocrine/metabolic disturbances. Generally, these disturbances clinically manifest with CRF stages 4 and 5 (GFR <30 mL/min).
 generally are asymptomatic and do not experience clinically evident disturbances in water or electrolyte balance or endocrine/metabolic disturbances. Generally, these disturbances clinically manifest with CRF stages 4 and 5 (GFR <30 mL/min).")
91
Clinical Manifestations
Hyperkalemia usually develops when GFR falls to less than mL/min because of the decreased ability of the kidneys to excrete potassium. Metabolic acidosis because the kidney cannot excrete increased loads of acid.

92
Clinical Manifestations
Extracellular volume expansion and total-body volume overload results from failure of sodium and free water excretion. Anemia principally develops from decreased renal synthesis of erythropoietin, the hormone responsible for bone marrow stimulation for red blood cell (RBC). Calcium and Phosphorus imbalance occurs because of a disorder in metabolism. They have a reciprocal relationship in the body; as one rises, the other decreases.
. Calcium and Phosphorus imbalance occurs because of a disorder in metabolism. They have a reciprocal relationship in the body; as one rises, the other decreases.")
93
Signs and Symptoms Neurologic
weakness, fatigue, confusion, disorientation, tremors, seizures, restlessness of legs, burning of soles of feet, behavioral changes. Integumentary Gray-bronze skin colour, dry, flaky skin, pruritus, ecchymosis, thin brittle nails, coarse, thinning hair Pulmonary Crackles, thick tenacious sputum, depressed cough reflex, pleuritic pain, shortness of breath, engorged neck veins, tachypnea, uremic pneumonitis, “uremic lung” Gastrointestinal Ammonia odour to breath, metallic taste, mouth ulcerations and bleeding, anorexia, N&V, hiccups, constipation or diarrhea, bleeding from GI tract. Hematologic Anemia, thrombocytopenia Musculoskeletal Muscle cramps, loss of muscle strength, renal osteodystrophy, bone pain, bone fractures, foot drop

94
Nursing Care Plan Rationale Assessment provides baseline and ongoing database for monitoring changes and evaluating interventions Fluid restriction will determine on the basis of weight, urine output, and response of therapy Understanding promotes pt and family cooperation with fluid restrictions Oral hygiene minimizes dryness of oral mucous membranes Expected Outcomes Demonstrates no rapid weight changes Maintains dietary and fluid restrictions Exhibits normal skin turgour without edema Normal vitals Reports no difficulty breathing or shortness of breath Reports decrease dryness of oral mucous membranes. Excess fluid volume r/t decreased urine output, and retention of sodium and water Goal is maintenance of ideal body weight without access fluid Nursing Interventions Assess fluid Status Daily weight I & O Skin turgour & edema Distention of neck veins BP, P, R Limit fluid intake to prescribed volume Explain to pt and family rationale for restriction of food Provide or encourage frequent oral care

95
Nursing Care Plan Hyperkalemia, pericarditis, pericardial effusion and temponade, hypertension, anemia, bone disease Goal: Patient experiences and absence of complications Nursing Interventions Hyperkalemia Monitor serum K levels and notify physician if greater than 5.5 mEq/L. Assess patient for muscle weakness, diarrhea, ECG changes( tall tented Twaves, widened QRS). Rationale Hyperkalemia causes potentially life-threatening changes to the body Cardiovascular S & S are characteristic of hyperkalemia Expected Outcomes Pt has normal K level Experiences no muscle weakness or diarrhea, Exhibits normal ECG pattern Vital signs are within normal limits
. Rationale. Hyperkalemia causes potentially life-threatening changes to the body. Cardiovascular S & S are characteristic of hyperkalemia. Expected Outcomes. Pt has normal K level. Experiences no muscle weakness or diarrhea, Exhibits normal ECG pattern. Vital signs are within normal limits.")
96
Pericarditis, Pericardial effusion, tamponade
Rationale About 30-50% of CRF pts develop pericarditis due to uremia; fever ,chest pain, and pericardial friction rub are classic signs Pericardial effusion is common following pericarditis. Signs of effusion: paradoxical pulse (> 10 mm drop in BP during inspiration) and signs of shock d/t compression of the heart by a large effusion. Cardiac tamponade exists when the pt is severely compromised hemodynamically Outcomes Has strong and equal peripheral pulse Absence of paradoxical pulse Absence of pericardial effusion, or tamponade Pericarditis, Pericardial effusion, tamponade Assess for fever, chills, chest pain and pericardial friction rub (signs of pericarditis). If pt has pericarditis, ax q 4 hrs Extreme hypotension Weak of absent peripheral pulses, altered level of consciousness, bulging neck veins.
 and signs of shock d/t compression of the heart by a large effusion. Cardiac tamponade exists when the pt is severely compromised hemodynamically. Outcomes. Has strong and equal peripheral pulse. Absence of paradoxical pulse. Absence of pericardial effusion, or tamponade. Pericarditis, Pericardial effusion, tamponade. Assess for fever, chills, chest pain and pericardial friction rub (signs of pericarditis). If pt has pericarditis, ax q 4 hrs. Extreme hypotension. Weak of absent peripheral pulses, altered level of consciousness, bulging neck veins.")
97
Monitor and record blood pressure
Hypertension Monitor and record blood pressure Administer antihypertensives as prescribes Encourage compliance with dietary and fluid restriction therapy Teach pt report signs of fluid overload, vision changes, headaches, edema, seizures Rationale Antihypertensives play a key role in tx of hypertension associated with CRF. Adherence to diet and fluid restrictions prevents excess fluid and sodium accumulation These are indications of inadequate control of hypertension, and need to alter therapy Outcomes BP is within normal limits No headaches, visual problems or seizures No edema Demonstrates compliance with dietary and fluid restrictions

98
Rationale Provides Ax of degree of anemia RBCs need iron and folic acid to be produced. Anemia is worsened by drawing numerous specimens Blood component therapy may be needed if pt has symptoms Outcomes Pt has normal colour without pallor Hematology values are within acceptable limits Experiences not bleeding form any site. Anemia Monitor RBC count, Hg, and HCT levels Administer prescribes meds: iron and folic acid Avoid drawing unnecessary blood specimens Teach pt to prevent bleeding; avoid vigorous nose blowing Administer blood component therapy

99
Monitor serum lab values ( calcium, phosphorus, aluminum)
Bone Disease Administer the following meds as prescribed: phosphate binders, calcium supplements, vit D supplements Monitor serum lab values ( calcium, phosphorus, aluminum) Assist pt with exercise program Rationale CRF causes numerous physiologic changes affecting calcium, phosphorus and vit D metabolism. Hyperphophatemia, hypocalcemia, and excess aluminum accumulation are common Bone demineraliztion decreases with immobility. Outcomes Serum calcium, phosphorus, and aluminum levels are within acceptable ranges. Has no bone demineralization Discuss importance of maintaining activity level and exercise program.
 Assist pt with exercise program. Rationale. CRF causes numerous physiologic changes affecting calcium, phosphorus and vit D metabolism. Hyperphophatemia, hypocalcemia, and excess aluminum accumulation are common. Bone demineraliztion decreases with immobility. Outcomes. Serum calcium, phosphorus, and aluminum levels are within acceptable ranges. Has no bone demineralization. Discuss importance of maintaining activity level and exercise program.")
100
Diet Protein restriction b/c urea, uric acid and organic acids- the breakdown product of dietary and tissue proteins- accumulate rapidly in the blood when there is impaired renal clearance. The allowed protein must be of high biologic value (diary products, eggs, meats). These proteins are those that are complete proteins and supply the essential amino acids necessary for cell growth and repair; also maintenance of fluid balance, healing and skin integrity, and maintenance of immune function. Fluid restrictions: fluid allowance is usually ml more than the previous day’s 24 hr output. Calories are supplied by carbs and fats to prevent wasting and malnutrition Vitamin supplementation because a protein restricted diet does provide the necessary amounts of vitamins and the pt on dialysis may lose water soluble vitamins from the blood during treatment.
. These proteins are those that are complete proteins and supply the essential amino acids necessary for cell growth and repair; also maintenance of fluid balance, healing and skin integrity, and maintenance of immune function. Fluid restrictions: fluid allowance is usually ml more than the previous day’s 24 hr output. Calories are supplied by carbs and fats to prevent wasting and malnutrition. Vitamin supplementation because a protein restricted diet does provide the necessary amounts of vitamins and the pt on dialysis may lose water soluble vitamins from the blood during treatment.")
101
Nursing Diagnoses Altered fluid volume (excess) related to compromised regulatory mechanism (renal failure) with retention of water as evidenced by intake greater then output (oliguria)
 related to compromised regulatory mechanism (renal failure) with retention of water as evidenced by intake greater then output (oliguria)")
102
Nursing Diagnoses Risk for Altered cardiac output: decrease related to fluid overload Assessments: -Monitor BP & HR -Assess color of skin, mucous membranes and nail beds -Note occurrence of slow pulse, hypotension, flushing, nausea/vomiting and depressed level of consciousness -Maintain bed rest

103
Assessments continued
Monitor lab results Potassium, Calcium, magnesium, phosphate

104
Nursing Diagnosis Altered nutrition: less than body requirements related to ulcerations of oral mucousa Patient Outcomes: Maintains/regains weight

105
Altered nutrition continued
Assessments/Interventions Document dietary intake Provide frequent, small feedings Offer frequent mouth care if possible with dilute (25%) acetic acid solution. Consult with dietician/nutritional support team Restrict K, Na, and phosphorus intake as indicated
 acetic acid solution. Consult with dietician/nutritional support team. Restrict K, Na, and phosphorus intake as indicated.")
106
Nursing Diagnosis This one is for the family
Potential knowledge deficit related to unfamiliarity with information resources as evidenced by questions/request for information

107
Knowledge Deficit continued
Review disease process, prognosis, and precipitating factors Discuss dietary plan/restrictions.

108
Medications for CRF Diuretics
Furosemide (Lasix) only given with severe fluid overload Increases excretion of water by interfering with chloride-binding cotransport system, which, in turn, inhibits sodium and chloride reabsorption in the thick ascending loop of Henle and the distal renal tubule Adult dose: mg PO/IV once; repeat 6-8h prn or dose may be increased by mg no sooner than 6-8h after previous dose until desired effect Nursing Assessments: Watch for hypokalemia, assess BP before and during therapy can cause hypotension
 only given with severe fluid overload. Increases excretion of water by interfering with chloride-binding cotransport system, which, in turn, inhibits sodium and chloride reabsorption in the thick ascending loop of Henle and the distal renal tubule. Adult dose: mg PO/IV once; repeat 6-8h prn or dose may be increased by mg no sooner than 6-8h after previous dose until desired effect. Nursing Assessments: Watch for hypokalemia, assess BP before and during therapy can cause hypotension.")
109
Medications for CRF continued
Phosphate-lowering agents Calcium acetate (Calphron, PhosLo) Combines with dietary phosphorus to form insoluble calcium phosphate, which is excreted in feces. Adult dose: 1-2 g PO bid-tid with each meal; increase to bring serum phosphate value to 6 mg/dL as long as hypercalcemia does not develop; Calcium carbonate (Caltrate, Apo-Cal, Tums) Successfully normalizes phosphate concentrations Neutralizes gastric acidity, increase serum Ca Adult dose: 1-2 g PO divided bid-tid; with meals as a phosphorous binder; between meals as a calcium supplement
 Combines with dietary phosphorus to form insoluble calcium phosphate, which is excreted in feces. Adult dose: 1-2 g PO bid-tid with each meal; increase to bring serum phosphate value to 6 mg/dL as long as hypercalcemia does not develop; Calcium carbonate (Caltrate, Apo-Cal, Tums) Successfully normalizes phosphate concentrations. Neutralizes gastric acidity, increase serum Ca. Adult dose: 1-2 g PO divided bid-tid; with meals as a phosphorous binder; between meals as a calcium supplement.")
110
Phosphate-lowering agents
Calcitriol (Rocaltrol, Calcijex) Increases intestinal absorption of calcium for treatment of hypocalcemia and increases renal tubular resorption of phosphate Adult dose for hypocalcemia during chronic dialysis: 0.25 mcg/day or every other day, may require mcg/day PO Sevelamer (Renagel) Indicated for the reduction of serum phosphorous in patients with ESRD. Adult dose: Initial: mg PO tid with meals Maintenance: Increase or decrease by mg per meal q2wk to maintain serum phosphorous at 6 mg/dL or less
 Increases intestinal absorption of calcium for treatment of hypocalcemia and increases renal tubular resorption of phosphate. Adult dose for hypocalcemia during chronic dialysis: 0.25 mcg/day or every other day, may require mcg/day PO. Sevelamer (Renagel) Indicated for the reduction of serum phosphorous in patients with ESRD. Adult dose: Initial: mg PO tid with meals Maintenance: Increase or decrease by mg per meal q2wk to maintain serum phosphorous at 6 mg/dL or less.")
111
Phosphate-lowering agents
Lanthanum carbonate (Fosrenal) for reduction of high phosphorus levels in patients with ESRD Adult dose: Initial: mg PO tid pc (chewable tabs); adjust dose q2-3wk to target serum phosphorus level Maintenance: mg PO tid pc
 for reduction of high phosphorus levels in patients with ESRD. Adult dose: Initial: mg PO tid pc (chewable tabs); adjust dose q2-3wk to target serum phosphorus level Maintenance: mg PO tid pc.")
112
Phosphate-lowering agents
Doxercalciferol (Hectorol) To lower parathyroid hormone levels in patients undergoing chronic kidney dialysis. Increases serum Ca Adult dose: 10 mcg PO 3 times/wk at dialysis; increase dose by 2.5 mcg/8 wk if iPTH is not lowered by 50% and fails to reach the target range; not to exceed 20 mcg/3 times/wk Alternatively, 4 mcg IV 3 times/wk; may adjust dose by 1-2 mcg/8 wk to maintain iPTH levels Nursing Assessment for all phosphate lowering agents: Monitor BUN, creatinine, chloride, electrolytes, urine pH, urinary calcium, mg, phosphate, urinalysis urinary Ca should be 9-10mg/dl, assess for hypocalcemia: headache, N/V, confusion
 To lower parathyroid hormone levels in patients undergoing chronic kidney dialysis. Increases serum Ca. Adult dose: 10 mcg PO 3 times/wk at dialysis; increase dose by 2.5 mcg/8 wk if iPTH is not lowered by 50% and fails to reach the target range; not to exceed 20 mcg/3 times/wk Alternatively, 4 mcg IV 3 times/wk; may adjust dose by 1-2 mcg/8 wk to maintain iPTH levels. Nursing Assessment for all phosphate lowering agents: Monitor BUN, creatinine, chloride, electrolytes, urine pH, urinary calcium, mg, phosphate, urinalysis urinary Ca should be 9-10mg/dl, assess for hypocalcemia: headache, N/V, confusion.")
113
Medications for CRF continued
Anemia Epoetin alfa (Epogen, Procrit) Stimulates RBC production Adult dose: U/kg IV/SC 3 times per week, then adjust dose by 25 U/kg/dose to maintain appropriate Hct; maintenance U/kg, titrate to target Hct, Nursing Assessment: Monitor renal studies: urinalysis, protein, blood, BUN, creatinine; I&O. Monitor blood studies, Hgb, Hct, RBC, WBC, INR, PTT
 Stimulates RBC production. Adult dose: U/kg IV/SC 3 times per week, then adjust dose by 25 U/kg/dose to maintain appropriate Hct; maintenance U/kg, titrate to target Hct, Nursing Assessment: Monitor renal studies: urinalysis, protein, blood, BUN, creatinine; I&O. Monitor blood studies, Hgb, Hct, RBC, WBC, INR, PTT.")
114
Medications for CRF continued
Darbepoetin (Aranesp) Stimulates erythropoiesis Adult dose: 0.45 ug/kg IV/SC as a single injection, titrate not to exceed a target Hgb of 12 g/dl Has a longer half-life than epoetin alfa Nursing Assessments: Assess blood studies, renal studies; assess BP, check for rising BP as Hct rises
 Stimulates erythropoiesis. Adult dose: 0.45 ug/kg IV/SC as a single injection, titrate not to exceed a target Hgb of 12 g/dl. Has a longer half-life than epoetin alfa. Nursing Assessments: Assess blood studies, renal studies; assess BP, check for rising BP as Hct rises.")
115
Medications for CRF continued
Iron Salts To treat anemia Ferrous sulfate (Feosol, Feratab, Slow FE) Replaces iron stores need for RBC development Adult dose: mg tid Iron sucrose (Venofer) Used to treat iron deficiency dute to chronic hemodialysis Adult dose: IV 5ml (100mg of elemental iron) given during dialysis, most will need 1000mg of elemental iron over 10 dialysis Nursing Assessments: Monitor blood studies, Hct, Hgb, total Fe, monthly. Assess bowel elimination for constipation
 Replaces iron stores need for RBC development. Adult dose: mg tid. Iron sucrose (Venofer) Used to treat iron deficiency dute to chronic hemodialysis. Adult dose: IV 5ml (100mg of elemental iron) given during dialysis, most will need 1000mg of elemental iron over 10 dialysis. Nursing Assessments: Monitor blood studies, Hct, Hgb, total Fe, monthly. Assess bowel elimination for constipation.")
116
Tia’s kidney function continues to decline and she is forced to begin dialysis

117
Dialysis

118
What is Dialysis? Dialysis is a type of renal replacement therapy which is used to provide artificial replacement for lost kidney function due to acute or chronic kidney failure It is a life support treatment, it does not cure acute or chronic renal failure May be used for very sick clients who have suddenly lost kidney function May be used for stable clients who have permanently lost kidney function Healthy kidneys remove waste products (potassium, acid, urea) from the blood and they also remove excess fluid in the form of urine Dialysis has to duplicate both of these functions Dialysis – waste removal Ultrafiltration – fluid removal
 from the blood and they also remove excess fluid in the form of urine. Dialysis has to duplicate both of these functions. Dialysis – waste removal. Ultrafiltration – fluid removal.")
119
Principle of Dialysis Dialysis works on the principle of diffusion of solutes along a concentration gradient across a semipermiable membrane Blood passes on one side of the semipermeable membrane, and a dialysis fluid is passed on the other side By altering the composition of the dialysis fluid, the concentrations of the undesired solutes (potassium, urea) in the fluid are low, but the desired solutes (sodium) are at their natural concentration found in healthy blood
 in the fluid are low, but the desired solutes (sodium) are at their natural concentration found in healthy blood.")
120
Prescription for Dialysis
A prescription for dialysis is given by a physician who specializes in the kidney (nephrologist) The MD will set various parameters for the treatment Time and duration of the dialysis sessions Size of the dialyzer Rate of blood flow
 The MD will set various parameters for the treatment. Time and duration of the dialysis sessions. Size of the dialyzer. Rate of blood flow.")
121
Types of Dialysis 1. Hemodialysis 2. Peritoneal Dialysis

122
Hemodialysis

123
What is Hemodialysis (HD)?
Client’s blood is passed through a system of tubing (dialysis circuit) via a machine to a semipermeable membrane (dialyzer) which has the dialysis fluid running on the other side The cleansed blood is then returned via the circuit back to the body The dialysis process is very efficient (much higher than in the natural kidneys), which allows treatments to take place intermittently (usually 3 times a week), but fairly large volumes of fluid must be removed in a single treatment which can be very demanding on a client
 via a machine to a semipermeable membrane (dialyzer) which has the dialysis fluid running on the other side. The cleansed blood is then returned via the circuit back to the body. The dialysis process is very efficient (much higher than in the natural kidneys), which allows treatments to take place intermittently (usually 3 times a week), but fairly large volumes of fluid must be removed in a single treatment which can be very demanding on a client.")
124
Side Effects of HD The side effects are proportionate to the amount of fluid being removed Decreased blood pressure Fatigue Chest pains Leg cramps Headaches Electrolyte imbalance N&V Reaction to the dialyzer Air embolism

125
Complications of HD Because HD requires access to the circulatory system, clients have a portal of entry for microbes, which could lead to infection The risk of infection depends on the type of access used Bleeding may also occur at the access site Blood clotting was a serious problem in the past, but the incidence of this has decreased with the routine use of anticoagulants (Heparin is the most common) Anticoagulants also come with their own risk of side effects and complications
 Anticoagulants also come with their own risk of side effects and complications.")
126
Rare Complication of HD
On the rare occasion, a client may have a severe anaphylactic reaction Sneezing Wheezing SOB Back pain Chest pain Sudden death This can be caused by the sterilant in the dialyzer or the material in the membrane itself

127
Hemodialysis ~ The “Integra”

128
Three Types of Access for HD
IV catheter Arteriovenous (AV) fistula Synthetic graft The type of access is influenced by factors such as expected time course of the clients renal failure and the condition of the clients vasculature Some clients may have multiple accesses, usually because an AV fistula or a graft is maturing and an IV catheter is still being used
 fistula. Synthetic graft. The type of access is influenced by factors such as expected time course of the clients renal failure and the condition of the clients vasculature. Some clients may have multiple accesses, usually because an AV fistula or a graft is maturing and an IV catheter is still being used.")
129
IV Catheter (Central Venous Catheter)
Consists of a plastic catheter with two lumens which is inserted into a large vein (vena cava via the internal jugular vein) to allow large flows of blood to be withdrawn from the first lumen The blood goes into the dialysis circuit, and is returned to the body via the second lumen Non-tunneled Tunneled This type of access is used for clients who need rapid access for immediate dialysis Clients who are likely to recover from ARF Client with end-stage renal failure Clients waiting for other sites to mature This type of access is very popular for clients because it doesn’t involve needles for each treatment
 to allow large flows of blood to be withdrawn from the first lumen. The blood goes into the dialysis circuit, and is returned to the body via the second lumen. Non-tunneled. Tunneled. This type of access is used for clients who need rapid access for immediate dialysis. Clients who are likely to recover from ARF. Client with end-stage renal failure. Clients waiting for other sites to mature. This type of access is very popular for clients because it doesn’t involve needles for each treatment.")
130
Complications of an IV Catheter
Venous Stenosis This is the abnormal narrowing of the blood vessel Because the catheter is a foreign body in the vessel, it often provokes an inflammatory reaction in the vein wall This results in scarring and narrowing of the vein, often to the point where the vein occludes

131
AV Fistula This access is recognized as the preferred access method
To create a fistula a vascular surgeon joins an artery and a vein together Since this bypasses the capillaries, blood flows at a very high rate through the fistula This can be felt by placing a finger over a mature fistula (thrill) Usually created in the non-dominant hand It can be situated on the hand, forearm or the elbow It will take approximately 4-6 weeks to mature During treatment, 2 needles are inserted, one to draw blood out of the body and the other to return blood to the body
 Usually created in the non-dominant hand. It can be situated on the hand, forearm or the elbow. It will take approximately 4-6 weeks to mature. During treatment, 2 needles are inserted, one to draw blood out of the body and the other to return blood to the body.")
132
Advantages of an AV Fistula
Decreased infection rate Increased blood flow rates, therefore a more effective dialysis treatment Decreased incidence of thrombosis

133
Complications of an AV Fistula
If an AV fistula has a very high flow rate and the vasculature that supplies the rest of the limb is poor, than a ‘steal syndrome’ can occur Blood that enters the limb is drawn into the fistula and returned to the general circulation without entering the capillaries of the limb This results in cool extremities of the limb, cramping pains and possible tissue damage Long term complications can be the development of a bulging in the wall of the vein (aneurysm) The vessel wall is weakened by the repeated insertion of needles over time Can be reduced by careful needling technique
 The vessel wall is weakened by the repeated insertion of needles over time. Can be reduced by careful needling technique.")
134
Hemodialysis ~ fistula

135
AV Graft This is much like a fistula, except an artificial vessel is used to join the artery and the vein Grafts are used when client’s own vasculature does not permit a fistula An AV graft will mature much faster than an AV fistula, and it could be ready to use within days after formation

136
Hemodialysis ~ Graft

137
Complications of an AV Graft
AV grafts are at high risk for narrowing where the graft is sewn to the vein As a result clotting or thrombosis may occur As a foreign material is being placed in the body, there is a greater risk of infection

138
Equipment Needed for HD
The HD machine performs the function of pumping the patient's blood and the dialysate through the dialyzer. The newest dialysis machines on the market are highly computerized and continuously monitor an array of safety-critical parameters, including blood and dialysate flow rates, blood pressure, heart rate, conductivity, pH, etc. If any reading is out of normal range, an audible alarm will sound to alert the patient-care technician who is monitoring the patient.

139
Equipment – Water System
An extensive water purification system is absolutely critical for HD Since dialysis patients are exposed to vast quantities of water, which is mixed with the acid bath to form the dialysate, even trace mineral contaminants or bacterial endotoxins can filter into the patient's blood. Because the damaged kidneys are not able to perform their intended function of removing impurities, ions that are introduced into the blood stream via water can build up to hazardous levels, causing numerous symptoms including death For this reason, water used in HD is purified

140
Equipment – The Dialyzer
The dialyzer, or artificial kidney, is the piece of equipment that actually filters the blood The blood is run through a bundle of very thin capillary-like tubes, and the dialysate is pumped in a chamber bathing the fibers The process mimics the physiology of the glomerulus and the rest of the nephron Dialyzers come in many different sizes. A larger dialyzer will usually translate to an increased membrane area, and an increase in the amount of undesired solutes removed from the patient's blood. The nephrologist will prescribe the dialyzer to be used depending on the patient Dialyzers are not shared between patients in the practice of reuse.

141
Temporary Hemodialysis Catheter
Exit site at surface of the skin Inserted in the jugular vein Tip located at junction of SVC and right Atrium

142
Tunneled Hemodialysis Catheter
Dacron cuff Catheter tunnel Exit site Inserted in the jugular vein Tip located at junction of SVC and right Atrium

144
Peritoneal Dialysis

145
Peritoneal Dialysis

146
Peritoneal Dialysis Catheter

147
What is Peritoneal Dialysis (PD)?
Peritoneal dialysis works by using the body's peritoneal membrane, which is inside the abdomen, as a semi-permeable membrane. A specially formulated dialysis fluid is instilled around the membrane, using an indwelling catheter, then dialysis can occur, by diffusion Excess fluid can also be removed by osmosis, by altering the concentration of glucose in the fluid. Dialysis fluid is instilled via a peritoneal dialysis catheter, which is placed in the patient's abdomen, running from the peritoneum out to the surface, near the navel Peritoneal dialysis is typically done in the patient's home and workplace, but can be done almost anywhere

148
Advantages of PD Can be done at home
Relatively easy for the client to learn Easy to travel with, bags of solution are easy to take on holiday Fluid balance is usually easier when the client is on PD than if the client is on HD

149
Disadvantage of PD Requires a degree of motivation and attention to cleanliness while performing PD There are a number of complications

150
Complications of PD Peritoneal dialysis requires access to the peritoneum. As this access breaks normal skin barriers, and as people with renal failure generally have a slightly suppressed immune system, infection is a relatively common problem Long term peritoneal dialysis can cause changes in the peritoneal membrane, causing it to no longer act as a dialysis membrane as well as it used to. This loss of function can manifest as a loss of dialysis adequacy, or poorer fluid exchange (also known as ultrafiltration failure) Fluid may leak into surrounding soft tissue, often the scrotum in males Hernias are another problem that can occur due to the abdominal fluid load
 Fluid may leak into surrounding soft tissue, often the scrotum in males. Hernias are another problem that can occur due to the abdominal fluid load.")
151
Nursing Assessments Before client is in the unit, look at the nurses notes from the treatment before Any problems, will help nurse plan for the upcoming treatment Look at the client Strength Gait Whether client needs assistance Color Puffiness Could be caused by excess fluid, too much to drink, more fluid should be taken off with each treatment, changes in voiding pattern (are they voiding less than they did last month)
")
152
Assessments Con’t Shortness of breath
Could indicate fluid around the lungs Ask about SOB at night (does client have to sleep in a sitting position?) Ask the client how they are feeling The client is usually the best source of information Clients are in 3 times a week, dialysis nurses really get to know their clients Evaluate access Bruising, swollen, tender Bruit – listen with the stethoscope for a swishing sound of the blood, listen all the way up the arm Thrill – felt with the fingers, tells the nurse if the blood is flowing in the fistula (client’s are told to feel for this at home when a fistula is first initiated)
 Ask the client how they are feeling. The client is usually the best source of information. Clients are in 3 times a week, dialysis nurses really get to know their clients. Evaluate access. Bruising, swollen, tender. Bruit – listen with the stethoscope for a swishing sound of the blood, listen all the way up the arm. Thrill – felt with the fingers, tells the nurse if the blood is flowing in the fistula (client’s are told to feel for this at home when a fistula is first initiated)")
153
Assessments During Treatment
Ask client how he/she feels Dizziness, diaphoretic, The machines automatically take BP and HR every 30 minutes Can program the machines to take it at whatever interval is necessary (every min, 10 min, 15 min) Try to recognize a problem before it starts (ex. Hypovolemic shock) Assess access site Watch trend of BP It usually gradually decreases throughout the course of the treatment, but look for sudden or drastic drops Bleeding, swelling, tenderness
 Try to recognize a problem before it starts (ex. Hypovolemic shock) Assess access site. Watch trend of BP. It usually gradually decreases throughout the course of the treatment, but look for sudden or drastic drops. Bleeding, swelling, tenderness.")
154
Nursing Interventions
If client comes in with shortness of breath, offer O2 which can be kept on for the full treatment if necessary Comfort Client’s are sitting in the same chair for up to four hours Offer extra pillows, some clients have special back pillow they leave in the unit Ensure TV and audio is working properly

155
Nursing Interventions Con’t
If the blood pressure is dropping too quickly: Slow or stop fluid removal for a time period The machines are constantly being adjusted throughout the course of the treatment depending on the BP If the BP drops suddenly cc of normal saline can be given to balance fluid levels Usually, more fluid will be taken off at the beginning of the treatment, this will allow the client to feel better at the end If the client is elderly, fluid removal starts slowly to ease them into the treatment

156
Responsibilities of Nursing Staff Prior to Dialysis
Ensure client is ready to sit for up to four hours Encourage client to use washroom before arriving to the unit Try to avoid laxatives if possible before treatment Ensure client has eaten meal prior to treatment

157
Responsibilities of Nursing Staff After Dialysis
A dialysis nurse will give unit leader or primary nurse a verbal report of treatment Any complications during treatment Check BP standing and sitting Assess access site Encourage client to rest Avoid treatments or physio for a couple of hours if possible Watch fluid intake Be aware if client is on fluid restriction Check thrill and bruit Do not take a BP on access arm Do not take blood from access arm

158
Does everyone understand how important we are? Kidneys Urine

Similar presentations





 Dr. Belal Hijji, RN, PhD April 18 & 23, 2012.>")














