Download presentation
Presentation is loading. Please wait.

1
HERSHEY MEDICAL CENTER EXPERIENCE WITH TIGHT GLYCEMIC CONTROL
Robert Gabbay, M.D., Ph.D. Associate Professor of Medicine Co-Director, Penn State Diabetes Center

2
Diabetes in Hospitalized Patients
Fourth most common co-morbid condition among hospitalized patients 10–12% of all hospital discharges 29% of all cardiac surgery patients 1–3 days longer hospital stay Diabetes in Hospitalized Patients Diabetes is the fourth most common comorbid condition complicating all hospital discharges. In 1997, diabetes was present in 9.5% of all hospital discharges and in 29% of patients undergoing cardiac surgery. Diabetes causes a 2- to 4-fold increase in rates of hospitalizations and increases hospital stay by 1–3 days, depending on the diagnosis on admission. Direct medical and indirect expenditures attributable to diabetes in 2002 were estimated at $132 billion. Direct medical expenditures alone totaled $91.8 billion and comprised $23.2 billion for diabetes care, $24.6 billion for chronic complications attributable to diabetes, and $44.1 billion for excess prevalence of general medical conditions. Inpatient days (43.9%), nursing home care (15.1%), and office visits (10.9%) constituted the major expenditure groups by service settings. 17 million hospital days for patients with diabetes mellitus Inpatient contribution of healthcare expenditures attributable to diabetes $40.3 billion 43% of total direct expenditures in diabetes Annual per capita inpatient costs Diabetes = $6,309 Without diabetes = $1,289 ($2,971 adjusted) Furthermore, recent studies clearly show that hyperglycemia in hospitalized patients complicates numerous illnesses and is an independent risk factor for adverse outcomes. Hogan P, Dall T, Nikolov P. Economic costs of diabetes in the US in Diabetes Care. 2003;26:917–932. American Association of Endocrinologists. Accessed March 17, 2004. Hogan P, et al. Diabetes Care. 2003;26:917–932. American Association of Clinical Endocrinologists. Available at: Accessed March 17, 2004.
, nursing home care (15.1%), and office visits (10.9%) constituted the major expenditure groups by service settings. 17 million hospital days for patients with diabetes mellitus. Inpatient contribution of healthcare expenditures attributable to diabetes. $40.3 billion. 43% of total direct expenditures in diabetes. Annual per capita inpatient costs. Diabetes = $6,309. Without diabetes = $1,289 ($2,971 adjusted) Furthermore, recent studies clearly show that hyperglycemia in hospitalized patients. complicates numerous illnesses and is an independent risk factor for adverse outcomes. Hogan P, Dall T, Nikolov P. Economic costs of diabetes in the US in Diabetes Care. 2003;26:917–932. American Association of Endocrinologists. Accessed March 17, Hogan P, et al. Diabetes Care. 2003;26:917–932. American Association of Clinical Endocrinologists. Available at: Accessed March 17,")
3
The Increasing Rate of Diabetes Among Hospitalized Patients
48% The Increasing Rate of Diabetes Among Hospitalized Patients Data regarding the burden of diabetes among hospitalized patients is somewhat difficult to determine because diabetes is reflected in multiple codes in the International Classification of Diseases, Ninth Revision. In the 1990s the number of hospital discharges with diabetes as the first-listed diagnosis began increasing. Accessed June 15, 2004. Available at: Accessed June 15, 2004.

4
Potential Benefits of Improving Glucose Control in the Hospital
Improving inpatient glycemic control provides an opportunity to Reduce mortality Reduce morbidity Reduce costs of care Length of stay (LOS) Cost of inpatient complications Fewer rehospitalizations Reduced extended care Potential Benefits of Improving Glucose Control in the Hospital Improving inpatient glycemic control provides an opportunity to Reduce mortality Reduce morbidity Reduce costs of care Length of stay (LOS) Cost of inpatient complications Fewer rehospitalizations Reduced extended care
 Cost of inpatient complications. Fewer rehospitalizations. Reduced extended care. Potential Benefits of Improving Glucose Control in the Hospital. Improving inpatient glycemic control provides an opportunity to. Reduce mortality. Reduce morbidity. Reduce costs of care. Length of stay (LOS) Cost of inpatient complications. Fewer rehospitalizations. Reduced extended care.")
6
Intensive Insulin Therapy in Critically Ill Surgical Patients
Setting: surgical intensive care unit in University Hospital, Leuven, Belgium Hypothesis: normalization of blood glucose levels with insulin therapy can improve prognosis of patients with hyperglycemia or insulin resistance Design: prospective, randomized, controlled study Conventional: insulin when blood glucose > 215 mg/dL Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL Intensive Insulin Therapy in Critically Ill Surgical Patients Recently, the concept that stress hyperglycemia was beneficial to critically ill patients was challenged by the results of a large, prospective, randomized, controlled trial, which studied the effects if intensive insulin therapy to manage hyperglycemia on morbidity and mortality. This landmark study evaluated whether the normalization of blood glucose levels with insulin therapy improves the prognosis for patients with hyperglycemia or insulin resistance. On admission to the intensive care unit, patients were randomly assigned to receive intensive insulin therapy (maintenance of blood glucose at a level between 80 and 110 mg/dL [4.4 and 6.1 mmol/L]) or conventional treatment (infusion of insulin only if the blood glucose level exceeded 215 mg/dL [11.9 mmol/L] and maintenance of glucose at a level between 180 and 200 mg/dL [10.0 and 11.1 mmol/L]). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
 or conventional treatment (infusion of insulin only if the blood glucose level exceeded 215 mg/dL [11.9 mmol/L] and maintenance of glucose at a level between 180 and 200 mg/dL [10.0 and 11.1 mmol/L]). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.")
7
Intensive Insulin Therapy in Critically Ill Surgical Patients
Conventional Intensive Mean AM blood glucose achieved (mg/dL) 153 103 % receiving insulin 39% 100% % BG < 40 mg/dL 6 39 Intensive Insulin Therapy in Critically Ill Surgical Patients It was feasible to achieve and maintain blood glucose levels at < 110 mg/dL by using a titration algorithm in all patients in the intensively treated group. Insulin requirements were highest and most variable during the first 6 hours of intensive care (mean, 7 IU/h; 10% of patients required > 20 IU/h). Between days 7 and 12, insulin requirements decreased by 40% on stable caloric intake (data not shown). With nutritional intake increasing from a mean of 550 to 1,600 calories/day during the first 7 days of intensive care, normoglycemia was reached within 24 hours, with a mean daily insulin dose of 77 IU and maintained with 94 IU on day 7 (data not shown). No serious hypoglycemic events were reported. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. No serious hypoglycemic events. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
 % receiving insulin. 39% 100% % BG < 40 mg/dL Intensive Insulin Therapy in Critically Ill Surgical Patients. It was feasible to achieve and maintain blood glucose levels at < 110 mg/dL by using a titration algorithm in all patients in the intensively treated group. Insulin requirements were highest and most variable during the first 6 hours of intensive care (mean, 7 IU/h; 10% of patients required > 20 IU/h). Between days 7 and 12, insulin requirements decreased by 40% on stable caloric intake (data not shown). With nutritional intake increasing from a mean of 550 to 1,600 calories/day during the first 7 days of intensive care, normoglycemia was reached within 24 hours, with a mean daily insulin dose of 77 IU and maintained with 94 IU on day 7 (data not shown). No serious hypoglycemic events were reported. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. No serious hypoglycemic events. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.")
8
Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival
100 Intensive treatment 96 92 Survival in ICU (%) Conventional treatment 88 84 Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival At 12 months, with a total of 1,548 patients enrolled, mortality during intensive care was reduced from 8.0% with conventional treatment to 4.6% with intensive insulin therapy (P < 0.04, with adjustment for sequential analyses). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. 80 20 40 60 80 100 120 140 160 Days After Admission Conventional: insulin when blood glucose > 215 mg/dL. Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367. Copyright ©2001 Massachusetts Medical Society. All rights reserved.
 Conventional treatment Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival. At 12 months, with a total of 1,548 patients enrolled, mortality during intensive care was reduced from 8.0% with conventional treatment to 4.6% with intensive insulin therapy (P < 0.04, with adjustment for sequential analyses). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359– Days After Admission. Conventional: insulin when blood glucose > 215 mg/dL. Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367. Copyright ©2001 Massachusetts Medical Society. All rights reserved.")
9
Intensive Insulin Therapy in Critically Ill Surgical Patients: Morbidity and Mortality Benefits
Sepsis Dialysis Blood Transfusion Polyneuropathy N = 1,548 Reduction (%) Intensive Insulin Therapy in Critically Ill Surgical Patients: Morbidity and Mortality Benefits Intensive insulin therapy also reduced overall in-hospital mortality by 34%, bloodstream infections by 46%, acute renal failure requiring dialysis or hemofiltration by 41%, the median number of red-cell transfusions by 50%, and critical-illness polyneuropathy by 44%. Patients receiving intensive therapy were less likely to require prolonged mechanical ventilation and intensive care. The benefit of intensive insulin therapy was attributable to its effect on mortality among patients who remained in the intensive care unit for more than 5 days (20.2% with conventional treatment vs. 10.6% with intensive insulin therapy, P = 0.005). The greatest reduction in mortality involved deaths due to multiple-organ failure with a proven septic focus. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. 34% 41% 44% 46% 50% van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
 Intensive Insulin Therapy in Critically Ill Surgical Patients: Morbidity and. Mortality Benefits. Intensive insulin therapy also reduced overall in-hospital mortality by 34%, bloodstream infections by 46%, acute renal failure requiring dialysis or hemofiltration by 41%, the median number of red-cell transfusions by 50%, and critical-illness polyneuropathy by 44%. Patients receiving intensive therapy were less likely to require prolonged mechanical ventilation and intensive care. The benefit of intensive insulin therapy was attributable to its effect on mortality among patients who remained in the intensive care unit for more than 5 days (20.2% with conventional treatment vs. 10.6% with intensive insulin therapy, P = 0.005). The greatest reduction in mortality involved deaths due to multiple-organ failure with a proven septic focus. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359– % 41% 44% 46% 50% van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.")
10
IV Insulin Therapy in Critically Ill Surgical Patients: Safety
A titration algorithm achieved and maintained blood glucose levels at < 110 mg/dL Insulin requirements were highest and most variable during first 6 hours of intensive care Normoglycemia was reached within 24 hours with a mean daily insulin dose of 77 IU; maintained with 94 IU on day 7 Blood glucose was monitored every 4 hours by ABG Statistically significant, but clinically harmless, hypoglycemia was observed briefly IV Insulin Therapy in Critically Ill Surgical Patients: Safety It was feasible and safe to achieve and maintain blood glucose levels at < 110 mg/dL by using a titration algorithm. Stepwise linear regression analysis identified body mass index, history of diabetes, reason for intensive care unit admission, at-admission hyperglycemia, caloric intake, and time in intensive care unit as independent determinants of insulin requirements. Insulin requirements were highest and most variable during the first 6 hours of intensive care (mean, 7 IU/h; 10% of patients required > 20 IU/h). Between days 7 and 12, insulin requirements decreased by 40% on stable caloric intake. With nutritional intake increasing from a mean of 550 to 1,600 calories/day during the first 7 days of intensive care, normoglycemia was reached within 24 hours, with a mean daily insulin dose of 77 IU and maintained with 94 IU on day 7. Brief, clinically harmless hypoglycemia occurred in 5.2% of intensive insulin-treated patients on median day 6 (2–14) vs. 0.8% of conventionally treated patients on day 11 (2–10). It is Important to decrease insulin infusion when patients begin enteral feeding. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
. Between days 7 and 12, insulin requirements decreased by 40% on stable caloric intake. With nutritional intake increasing from a mean of 550 to 1,600 calories/day during the first 7 days of intensive care, normoglycemia was reached within 24 hours, with a mean daily insulin dose of 77 IU and maintained with 94 IU on day 7. Brief, clinically harmless hypoglycemia occurred in 5.2% of intensive insulin-treated patients on median day 6 (2–14) vs. 0.8% of conventionally treated patients on day 11 (2–10). It is Important to decrease insulin infusion when patients begin enteral feeding. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.")
11
Keys to Van den Berghe succcess
1 nurse to 2 pts Need IV glucose Benefit most for > 5 days in ICU (1/3) Number needed to treat = 29 Karnofsky scores better after 6 and 12 months Studies in Europe in NICU, PICU, MICU
 Number needed to treat = 29. Karnofsky scores better after 6 and 12 months. Studies in Europe in NICU, PICU, MICU.")
12
Indications for Intravenous Insulin Therapy: Summary
Diabetic ketoacidosis Nonketotic hyperosmolar state Critical care illness (surgical, medical) Postcardiac surgery Myocardial infarction or cardiogenic shock NPO status in Type 1 diabetes Labor and delivery Glucose exacerbated by high-dose glucocorticoid therapy Perioperative period After organ transplant Total parenteral nutrition therapy Indications for Intravenous Insulin Therapy: Summary American Association of Clinical Endocrinologists. Available at: Accessed March 17, 2004.
 Postcardiac surgery. Myocardial infarction or cardiogenic shock. NPO status in Type 1 diabetes. Labor and delivery. Glucose exacerbated by high-dose glucocorticoid therapy. Perioperative period. After organ transplant. Total parenteral nutrition therapy. Indications for Intravenous Insulin Therapy: Summary. American Association of Clinical Endocrinologists. Available at: Accessed March 17,")
13
GETTING STARTED (1998) Define the problem Evaluate the evidence—CABG
Evaluate Current Care Identify the Stakeholders Identify Barriers

14
Portland Diabetes Project: Mortality
10 CII 8 6 Patients with diabetes Mortality (%) Patients without 4 diabetes Portland Diabetic Project: Mortality All patients with diabetes undergoing CABG (N = 3,554) were treated aggressively with either subcutaneous insulin (1987–1991) or continuous insulin infusion (1992–2001) for hyperglycemia in this nonrandomized, prospective study. Observed mortality and glucose control were both significantly better with continuous insulin infusion than with subcutaneous insulin therapy. Continuous insulin infusion independently reduced perioperative absolute mortality by 57% and risk-adjusted mortality by 50%. Improved survival was attributed to a reduction in cardiac-related deaths. Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007–1021. 2 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 Year Reprinted from Furnary AP, et al. J Thorac Cardiovasc Surg. 2003;125:1007–1021 with permission from American Association for Thoracic Surgery.
 Patients without. 4. diabetes. Portland Diabetic Project: Mortality. All patients with diabetes undergoing CABG (N = 3,554) were treated aggressively with either subcutaneous insulin (1987–1991) or continuous insulin infusion (1992–2001) for hyperglycemia in this nonrandomized, prospective study. Observed mortality and glucose control were both significantly better with continuous insulin infusion than with subcutaneous insulin therapy. Continuous insulin infusion independently reduced perioperative absolute mortality by 57% and risk-adjusted mortality by 50%. Improved survival was attributed to a reduction in cardiac-related deaths. Furnary AP, Gao G, Grunkemeier GL, et al. Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003;125:1007– Year. Reprinted from Furnary AP, et al. J Thorac Cardiovasc Surg. 2003;125:1007–1021 with permission from American Association for Thoracic Surgery.")
15
Rate of DSWI Rates With Different Ins Protocols
2.0% P = 0.01 Deep Wound Infection Rate (%) 0.8% Portland Diabetic Project: Rate of Deep Sternal Wound Infection Rates With Different Insulin Protocols After previously showing that elevated postoperative blood glucose levels are a predictor of deep sternal wound infection in diabetic patients, the investigators hypothesized that aggressive intravenous pharmacologic control of postoperative blood glucose levels would reduce the incidence of deep sternal wound infection. This was a prospective study of 2,467 consecutive patients with diabetes who underwent open heart surgical procedures between 1987 and 1997; perioperative blood glucose levels were recorded every 1 to 2 hours. Patients were classified into 2 sequential groups: The control group included 968 patients treated with sliding-scale–guided intermittent subcutaneous insulin (SQI) injections; the study group included 1,499 patients treated with a continuous intravenous insulin infusion in an attempt to maintain a blood glucose level of less than 200 mg/dL. Compared with subcutaneous insulin injections, continuous intravenous insulin infusion induced a significant reduction in perioperative blood glucose levels, which led to a significant reduction in the incidence of deep sternal wound infection in the continuous intravenous insulin infusion group (0.8% [12 of 1,499]) versus the intermittent subcutaneous insulin injection group (2.0% [19 of 968], p = by the χ2 test). Multivariate logistic regression revealed that continuous intravenous insulin infusion induced a significant decrease in the risk of deep sternal wound infection (p = 0.005; relative risk, 0.34), whereas obesity (p < 0.03; relative risk, 1.06) and use of an internal thoracic artery pedicle (p = 0.1; relative risk, 2.0) increased the risk of deep sternal wound infection. Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67:352–360; discussion 360–362. SQI = subcutaneous insulin; CII = continuous insulin infusion. Anthony Furnary MD CCNM Furnary AP, et al. Ann Thorac Surg. 1999;67:352–362.
 0.8% Portland Diabetic Project: Rate of Deep Sternal Wound Infection Rates. With Different Insulin Protocols. After previously showing that elevated postoperative blood glucose levels are a predictor of deep sternal wound infection in diabetic patients, the investigators hypothesized that aggressive intravenous pharmacologic control of postoperative blood glucose levels would reduce the incidence of deep sternal wound infection. This was a prospective study of 2,467 consecutive patients with diabetes who underwent open heart surgical procedures between 1987 and 1997; perioperative blood glucose levels were recorded every 1 to 2 hours. Patients were classified into 2 sequential groups: The control group included 968 patients treated with sliding-scale–guided intermittent subcutaneous insulin (SQI) injections; the study group included 1,499 patients treated with a continuous intravenous insulin infusion in an attempt to maintain a blood glucose level of less than 200 mg/dL. Compared with subcutaneous insulin injections, continuous intravenous insulin infusion induced a significant reduction in perioperative blood glucose levels, which led to a significant reduction in the incidence of deep sternal wound infection in the continuous intravenous insulin infusion group (0.8% [12 of 1,499]) versus the intermittent subcutaneous insulin injection group (2.0% [19 of 968], p = 0.01 by the χ2 test). Multivariate logistic regression revealed that continuous intravenous insulin infusion induced a significant decrease in the risk of deep sternal wound infection (p = 0.005; relative risk, 0.34), whereas obesity (p < 0.03; relative risk, 1.06) and use of an internal thoracic artery pedicle (p = 0.1; relative risk, 2.0) increased the risk of deep sternal wound infection. Furnary AP, Zerr KJ, Grunkemeier GL, et al. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67:352–360; discussion 360–362. SQI = subcutaneous insulin; CII = continuous insulin infusion. Anthony Furnary MD 1999 CCNM. Furnary AP, et al. Ann Thorac Surg. 1999;67:352–362.")
16
CURRENT STATE OF CARE The infamous sliding scale Benign neglect
Endocrinology consults on occasion Typical glucose monitoring every 4-6 hours

17
IDENTIFY STAKEHOLDERS
CT Surgery Anesthesia Nursing Team Outcomes Research Team Endocrinology and Diabetes The hospital/payors

18
IDENTIFY BARRIERS Glucose monitoring Who? How?
Understanding the rationale Nursing time and effort

19
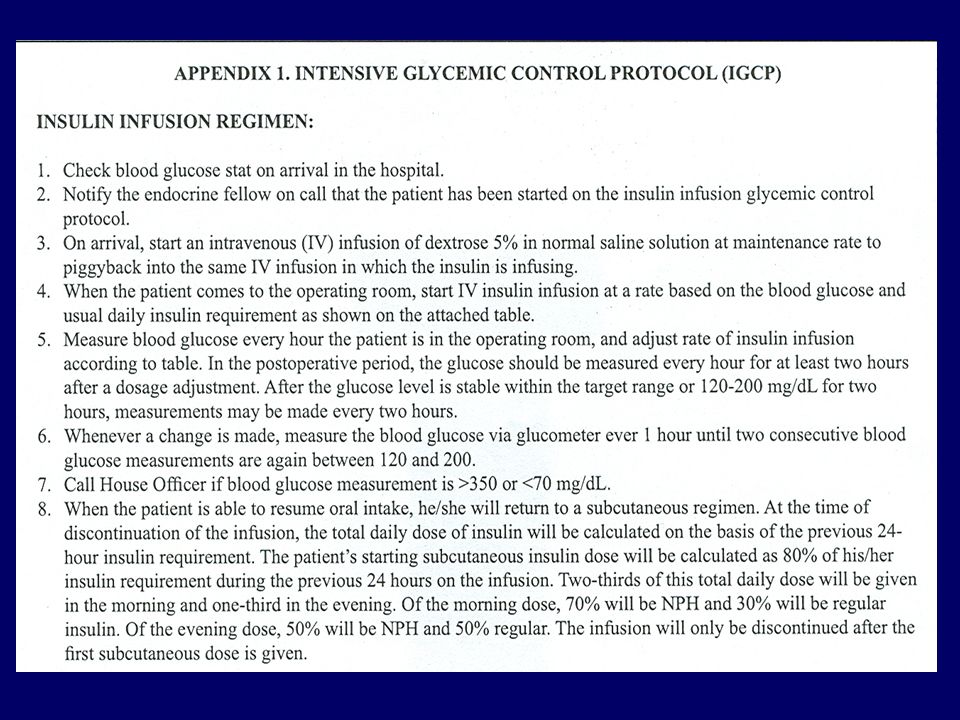
DEVELOPMENT OF THE INSULIN INFUSION GLYCEMIC CONTROL PROTOCOL (IGCP)
Multidisciplinary team led by Endocrinology Glucose meters needed to be available Goal mg/dL Grand rounds and educational programs Evaluate outcomes

20
Endocrine Practice 10:112 (2004)
")
21
HMC IGCP Intervention All pts undergoing CABG
Start IV insulin when present to anesthesia Continue IV insulin by protocol until taking po Endo consult to adjust insulin Multi-disciplinary team- nurses, anesthesia, CT surgery, outcomes research team, endo Endocrine Practice 2004

26
Histogram of all glucose levels in non-drip group and insulin drip protocol

27
Our Analysis Financial data
Costs incurred in 1999 normalized to the year 2000 (3% adjustment) Data collected from hospital’s cost accounting database and included following additional costs of IGCP: More frequent BG monitoring Pharmacy expenditures Routine endocrine consultation
 Data collected from hospital’s cost accounting database and included following additional costs of IGCP: More frequent BG monitoring. Pharmacy expenditures. Routine endocrine consultation.")
28
COSTS Underestimated : Readmission
Indirect costs, i.e., patient satisfaction, negative publicity and reduced referrals Risk of litigation

31
CONCLUSIONS Mean blood glucose improved from 241 to 183 (first 48 hours) Average number glucose determinations was 23.8 vs. 8 Revenue neutral despite endocrine consults, pharmacy costs, pharmacy Cost offset by clinical improvement and overall cost savings Wide acceptance by nursing and docs

32
EVERYTHING CHANGES WITH THE VAN DEN BERGHE STUDY

33
Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival
100 Intensive treatment 96 92 Survival in ICU (%) Conventional treatment 88 84 Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival At 12 months, with a total of 1,548 patients enrolled, mortality during intensive care was reduced from 8.0% with conventional treatment to 4.6% with intensive insulin therapy (P < 0.04, with adjustment for sequential analyses). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367. 80 20 40 60 80 100 120 140 160 Days After Admission Conventional: insulin when blood glucose > 215 mg/dL. Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367. Copyright ©2001 Massachusetts Medical Society. All rights reserved.
 Conventional treatment Intensive Insulin Therapy in Critically Ill Surgical Patients Improves Survival. At 12 months, with a total of 1,548 patients enrolled, mortality during intensive care was reduced from 8.0% with conventional treatment to 4.6% with intensive insulin therapy (P < 0.04, with adjustment for sequential analyses). van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359– Days After Admission. Conventional: insulin when blood glucose > 215 mg/dL. Intensive: insulin when glucose > 110 mg/dL and maintained at 80–110 mg/dL. van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367. Copyright ©2001 Massachusetts Medical Society. All rights reserved.")
34
Getting to a Lower Goal

35
GETTING LOWER This should be easy? Shortcuts are not always shortcuts
Better evidence Glucose monitoring a problem again Getting back to basics?

36
HMC New insulin drip protocol
Based on evidence based work from Van den Berghe (NEJM) Refined by multi-disciplinary team
 Refined by multi-disciplinary team.")
37
Key changes of new protocol
Target BG range (80-120mg/dl) D10 NS at maintenance rate 50 ml/hour No automatic endo consult
 D10 NS at maintenance rate 50 ml/hour. No automatic endo consult.")
38
Blood Glucose (BG) mg/dl
Regimen #1 For BG mg/dl Usual insulin dose <30 units/day or patients using only oral agents whose glycohemoglobin is <8 or current blood glucose mg/dl or non-diabetics Regimen #2 For BG >220 mg/dl Usual insulin dose >30 units/day or patients using only oral agents whose glycohemoglobin is >8 or unknown or current blood glucose > 220 mg/dl Starting dose 2 units/hour 4 units/hour If Initial BG decreases by >50% Decrease to 1 unit/hour Decrease to 2 units/hour >140 Increase by 1unit/hour Increase by 2units/hour 121‑140 Increase by 0.5 unit/hour Increase by 1 unit/hour 80-120 Unchanged 65-79 Reduce rate by 1 unit/hour 40-64 Administer 12.5 ml of D50 IV, stop infusion, call physician, and re‑check BG in 15‑30 minutes. When BG >64 mg/dl, re‑start infusion at 50% lower rate. <40 Administer 25 ml of D50 IV, stop infusion, call physician, and re‑check BG in 15‑30 minutes. When BG >64 mg/dl, re‑start infusion at 50% lower rate.

39
Coming to an ICU near you!

40
Key things to think about before you try this at home!
Lessons Learned: Key things to think about before you try this at home!

41
The Ideal IV Insulin Protocol
Easily ordered (signature only) Effective (gets to goal quickly) Safe (minimal risk of hypoglycemia) Easily implemented The Ideal IV Insulin Protocol In addition to specifying insulin dose, protocols should include specific guidelines for identifying patients at risk for hypoglycemia and actions to be taken to prevent and treat hypoglycemia.
 Effective (gets to goal quickly) Safe (minimal risk of hypoglycemia) Easily implemented. The Ideal IV Insulin Protocol. In addition to specifying insulin dose, protocols should include specific guidelines for identifying patients at risk for hypoglycemia and actions to be taken to prevent and treat hypoglycemia.")
42
Protocol Implementation
Multidisciplinary team Administration support Pharmacy & Therapeutics Committee approval Forms (orders, flowsheet, med kardex) Education: nursing, pharmacy, physicians & NP/PA Monitoring/QA Protocol Implementation Utilizing the team approach to inpatient care has been shown to reduce length of stay and improve clinical outcomes in patients with diabetes.
 Education: nursing, pharmacy, physicians & NP/PA. Monitoring/QA. Protocol Implementation. Utilizing the team approach to inpatient care has been shown to reduce length of stay and improve clinical outcomes in patients with diabetes.")
43
Bedside Glucose Monitoring
Strong quality-control program essential! Specific situations rendering capillary tests inaccurate Shock, hypoxia, dehydration Extremes in hematocrit Elevated bilirubin, triglycerides Drugs (acetaminophen, dopamine, salicylates) Bedside Glucose Monitoring Implementing intensive glycemic control in the hospital setting requires frequent and accurate blood glucose data. Capillary tests have the advantage over laboratory tests of providing rapid “point of care” information. However, there are situations in which these tests are rendered inaccurate and in which laboratory testing of venous glucose testing is required. Clement S, Braithwaite SS, Magee M, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553–591. Clement S, et al. Diabetes Care. 2004;27:553–591.
 Bedside Glucose Monitoring. Implementing intensive glycemic control in the hospital setting requires frequent and accurate blood glucose data. Capillary tests have the advantage over laboratory tests of providing rapid point of care information. However, there are situations in which these tests are rendered inaccurate and in which laboratory testing of venous glucose testing is required. Clement S, Braithwaite SS, Magee M, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:553–591. Clement S, et al. Diabetes Care. 2004;27:553–591.")
44
Limitations of current system
Nurse autonomy? GLUCOSE MONITORING Continuous Likely the first prototypes to be approved Closed loop Strengthening the business case for good glycemic control

Similar presentations








![INSULIN THERAPY IN ICU Dr SANJAY KALRA, D.M. [AIIMS]](/1/259452/big_thumb.jpg "INSULIN THERAPY IN ICU Dr SANJAY KALRA, D.M. [AIIMS]>")






>")



 for severe sepsis and septic shock treatment>")





