Download presentation
Presentation is loading. Please wait.

1
Health Determinants, Measurements, and Trends
Chapter 2 Health Determinants, Measurements, and Trends Richard Skolnik

2
The Importance of Measuring Health Status
In order to address global health issues, we must understand: The factors that most influence health status The indicators used to measure health status The trends that have occurred historically

3
Figure 2.1: Key Determinants of Health
Data from: The Public Health Agency of Canada. What Determines Health. Available at: Accessed November 19, 2010.

4
Key Health Status Indicators
Health status indicators are useful for: Finding which diseases people suffer from Determining the extent to which the disease causes death or disability Practicing disease prevention/interventions To perform these functions, it is important to use a consistent set of indicators and have accurate data

5
Key is a Vital Registration System
Vital registration systems record births, deaths, and causes of death An accurate system is key to having quality data on a population Many low- and middle-income countries lack a vital registration system Developing a system is progress towards understanding and addressing health problems – skip to slide 29

6
Key Health Status Indicators
Neonatal mortality rate # deaths of infants under 28 days of age per 1000 births in a year

7
Figure 2.4: Neonatal Mortality Rate, by WHO Region, 2004 Trends in neonatal mortality – more recent data Data from World Health Organization. Neonatal and Perinatal Mortality: Country, Regional, and Global Estimates Geneva: WHO; 2007: Table 2.

8
Neonatal Mortality One quarter to one half of all deaths occur within the first 24 hours of life 75% of deaths occur in the first week The 48 hours immediately following birth is the most crucial period for newborn survival A baby's chance of survival increases significantly with the presence of a skilled birth attendant at the birth WHO

9
Neonatal (<28 days) Mortality Data
Population Neonatal mortality rate, deaths/1000 live births Year U.S. overall 4.19 2009 Maine 4.2 2006 Black infants 8.2 White infants 3.43

10
Key Health Status Indicators
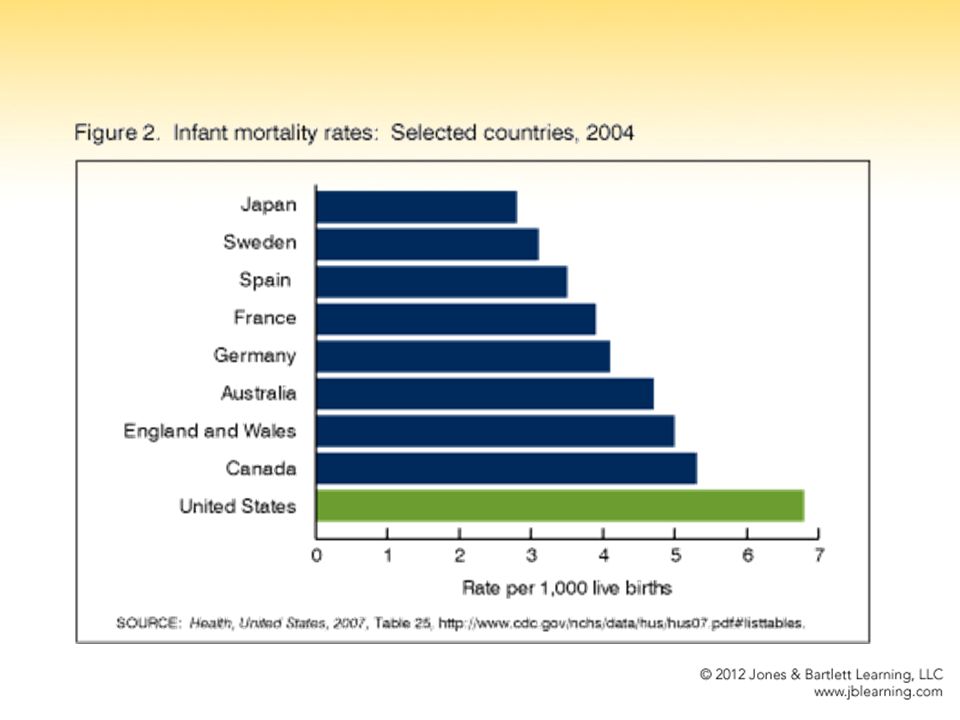
Infant mortality rate # deaths of infants in the first year of life per 1000 births in a year

11
Figure 2.3: Infant Mortality Rate, by World Bank Region, 2008
Data from The World Bank. World Development Indicators, Data Query. Available at: Accessed June 29, 2010.

13
Infant (<1 yr) Mortality Data
Population Infant mortality rate, deaths/1000 live births Year U.S. overall 6.8 5.7 6.7 6.42 2001 2004 2008 2009 Black 12.71

14
Key Health Status Indicators
Under 5 mortality rate aka child mortality rate the probability that a newborn infant will die before reaching the age of 5, # per 1000 live births

15
Figure 2.5: Under-five Child Mortality Rate, by World Bank Region, 2008
Data from The World Bank. World Development Indicators, Data Query. Available at: Accessed June 29, 2010.

16
Under 5 Mortality - WHO 6.9 million children under the age of five died in 2011. More than half of these early child deaths are due to conditions that could be prevented or treated with access to simple, affordable interventions.

17
Under 5 Mortality - WHO Leading causes of death:
pneumonia, preterm birth complications, diarrhea, birth asphyxia and malaria ~ one third of all child deaths are linked to malnutrition. Children in sub-Saharan Africa are about 16.5 times more likely to die before the age of five than children in developed regions.

18
Key Health Status Indicators
Neonatal mortality rate - # deaths of infants under 28 days of age per 1000 births in a year Infant mortality rate - # deaths of infants in the first year of life per 1000 births in a year Under 5 mortality rate (aka Child mortality rate) – the probability that a newborn infant will die before reaching the age of 5, # per 1000 live births
 – the probability that a newborn infant will die before reaching the age of 5, # per 1000 live births.")
19
Key Health Status Indicators
Maternal mortality rate # women who die as a result of pregnancy or childbirth complications per 100,000 live births in a year

20
Figure 2.6: Maternal Mortality Ratio, by World Bank Region, 2005
Data from The World Bank. World Development Indicators, Data Query. Available at: Accessed June 29,

21
Worldwide Data – Maternal Mortality
87% deaths in Sub-Saharan Africa and South Asia 50 percent of all deaths occurred in six nations: India, Nigeria, Pakistan, Afghanistan, Ethiopia, and the Democratic Republic of Congo

22
Key Health Status Indicators
Life expectancy at birth average # of years a newborn could expect to live if current mortality rates were to continue for the rest of the infant’s life

23
Figure 2.2: Life Expectancy at Birth, by World Bank Region, 2008
Data from the World Bank. World Development Indicators, Data Query. Available at: Accessed June 29, 2010.

24
Historical Trends based on Health Status Indicators
Table 2.11: Life Expectancy and Percentage Gain in Life Expectancy, , by World Bank Region Data from the World Bank. World Development Indicators, Data Query. Available at: Accessed July 6, 2010.

25
Worst country for women & children – Afghanistan
14% of births are attended by a health professional Lifetime risk of woman dying as a result of pregnancy or childbirth: 1 in 11 Life expectancy girl born today = 45

26
Afghanistan Under 5 mortality rate: 1 in 5 children die before the age of 5 Every woman is likely to suffer the loss of a child in her lifetime 39% of children moderately or severely underweight 52% Do not have access to clean water

27
Key Terms Morbidity – sickness/illness Mortality – death
physiological and/or psychological Mortality – death Mortality/Death rate expressed as # deaths per 1000 in a population in a year Disability – “temporary or long-term reduction in a person’s capacity to function”

28
Key Terms Prevalence - # of people suffering from a particular health condition over a period of time Generally consider at a given point in time (cross-sectional) – point prevalence Measure of existing cases at a given time Incidence rate - # of people contracting a disease per 1000 at risk in a year Measure of new cases per year
 – point prevalence. Measure of existing cases at a given time. Incidence rate - # of people contracting a disease per 1000 at risk in a year. Measure of new cases per year.")
32
Classification of Diseases
Communicable diseases – spread by an infectious agent Influenza, HIV/AIDS, measles, malaria, cholera Non-communicable diseases – diseases not spread by an infectious agent Hypertension, diabetes, lung cancer, CVD Injuries Accidents, violence, burns, cuts

33
Figure 2.10: The Burden of Disease by Group of Cause, Percent of Deaths, 2001
Data from Lopez AD, et al Global Burden of Disease and Risk Factors. Washington, DC and New York: The World Bank and Oxford University Press; 2006:8.

34
Table 2.10: The "Demographic Divide:" The Example of Nigeria and Japan
Data from PRB World Population Data Sheet. Available at Accessed November 24, 2010.

35
The Global Burden of Disease
Causes of Death by Region Higher income countries tend to have a greater burden of non-communicable disease Lower income countries to have a greater burden of communicable disease

36
Low and Middle Income Countries
% Deaths Rank. Cause of death, % of deaths 54 % Non-Communicable Diseases 1. Heart disease 11.8% 2. Strokes 9.5% 5. Perinatal conditions 5.1% 6. COPD 4.9% 36 % Communicable Diseases 3. respiratory infections 7.0% 4. HIV/AIDS 5.3% 7. Diarrheal disease 3.7% 8. TB 3.3% 9. Malaria 2.5% 10 % Injuries 10. road accidents 2.2%

37
High Income Countries % Deaths
Rank. Cause of death, % of deaths 87 % Non-Communicable Diseases 1. Heart disease 17.3% 2. Strokes 9.9% 3. Trachea, lung cancers 5.8% 5. COPD 3.8% 6. Colon and rectal cancers 3.3% 7. Alzheimer’s/dementia 2.6% 8. Diabetes 2.6% 9. Breast cancer 2.0% 10. Stomach cancer 1.9% 5.7 % Communicable Diseases 4. Respiratory infections 4.4% 7.5 % Injuries

38
The Global Burden of Disease
Causes of Death by Age Children in low- and middle-income countries often die of communicable disease HIV/AIDS and TB are among the leading causes of death among adults in low and middle-income countries

39
Table 2.5: The 10 Leading Causes of Death in Children Ages 0-14, by Broad Income Group, 2001

40
Table 2.6: The 10 Leading Causes of Death in Adults 15-59, by Broad Income Group, 2001

41
The Global Burden of Disease
In most low- and middle-income countries: Rural people will be less healthy Disadvantaged ethnic minorities will be less healthy Women will suffer as a result of their social positions Poor people will be less healthy Uneducated people will be less healthy

42
Measuring the Burden of Disease
Two indicators used to compare how far countries are from a state of good health Health-Adjusted Life Expectancy (HALE)- summarizes expected number of years to be lived in what might be termed the equivalent of good health Disability-Adjusted Life Year (DALY)- a unit for measuring the amount of health lost because of a particular disease or injury
- summarizes expected number of years to be lived in what might be termed the equivalent of good health. Disability-Adjusted Life Year (DALY)- a unit for measuring the amount of health lost because of a particular disease or injury.")
43
Measuring the Burden of Disease
HALE – Health-Adjusted Life Expectancy Calculated by a standard methodology by World Health Organization (WHO) Years of ill health are weighted according to severity and subtracted from overall life-expectancy
 Years of ill health are weighted according to severity and subtracted from overall life-expectancy.")
44
Table 2.2: Life Expectancy at Birth and Health-Adjusted Life Expectancy,, 2004
Data from WHO. Core Health Indicators. Available at: Accessed: September 24, 2006.

45
DALY – Disability Adjusted Life Year
First measured by World Bank as a “health gap measure” Used by World Bank and WHO – controversial measure DALYs are thought to be a better indicator of the health of a population than mortality rates DALY takes into account that many conditions associated with poor health are not fatal A higher DALY value indicates a greater health burden

46
DALYs “This time-based measure combines years of life lost due to premature mortality and years of life lost due to time lived in states of less than full health. The DALY metric was developed in the original Global Burden of Disease 1990 study to assess the burden of disease consistently across diseases, risk factors and regions.”

47
DALYs A DALY is a measure of years of fully healthy life lost due to disease, death, …….disability….. The higher the DALY value the more years lost due this “condition” – or the more years living with compromised health

48
DALYs DALYs are intended to provide a comparable measure of the burden of disease Used to: Aid in setting health care priorities Treatment and prevention Aid in setting research priorities Identify high need populations and target health interventions Measure success/effectiveness of interventions

49
DALYs…put another way Measures how many healthy years of life are lost between the population being studied and the healthiest possible populations Consider Communicable diseases Maternal, perinatal (1st weeks after birth) Nutritional disorders Non-communicable disorders Injuries/accidents Grouped together
 Nutritional disorders. Non-communicable disorders. Injuries/accidents. Grouped together.")
50
Table 2.3: The 10 Leading DALYs
Low and Middle-Income High-Income Countries Table 2-4 on page 30 shows DALYs in low and middle-income countries by regions

51
Calculating DALYs Disabilities/health conditions are weighted by one of 6 values based on the limitations or reduction in years of life associated with the “condition” The more serious the “condition” the higher the weighting Deaf, weighting = .33 Dead, weighting = 1 (most serious!) Calculating DALYs
 Calculating DALYs.")
52
WEIGHTING of DISABILITIES
Weightings quantify societal preferences for health states in relation to the societal ideal of good health. On average, society judges a year with blindness (weight 0.43) to be preferable to a year with paraplegia (weight 0.57), and a year with paraplegia to be preferable to a year with unremitting unipolar major depression (weight 0.76). Source this slide and next
 to be preferable to a year with paraplegia (weight 0.57), and a year with paraplegia to be preferable to a year with unremitting unipolar major depression (weight 0.76). Source this slide and next")
53
WEIGHTING of DISABILITIES
On average, society would prefer a person to have a year in good health followed by death, than a year with paraplegia followed by death. Society would prefer a person to live three years with paraplegia followed by death (3 years x 0.57 = 1.7 lost “healthy” years), than have one year of good health followed by death (2 lost years of good health).
, than have one year of good health followed by death (2 lost years of good health).")
54
Calculation of DALYs (without age-weighting and discounting)
The calculation of DALYs of a woman who has been deaf since she was 5 and dies when she is 50: (deafness is set at 0.33; life expectancy 80) : Number of healthy life years × the disability weight of full health (0) + life years with disability (50) × disability weight for deafness (0.33) + life years lost (30) × the weighting of death (1) (5 × 0)+ (45 × 0.33) + (30 × 1) = DALYs This example is, for didactic reasons, a simplified way of calculating DALY loss, omitting age-weighitng and discounting.
 : Number of healthy life years × the disability weight of full health (0) + life years with disability (50) × disability weight for deafness (0.33) + life years lost (30) × the weighting of death (1) (5 × 0)+ (45 × 0.33) + (30 × 1) = DALYs. This example is, for didactic reasons, a simplified way of calculating DALY loss, omitting age-weighitng and discounting.")
55
Other choices behind DALY
In addition to adjusting the value of life years with disability weights, and choosing a particular life expectancy, the value of a life year is modified by Age weighting life years of children and old people are counted less Discounting the value of a life year now is set higher than the value of future life years In the Global Burden of Disease approach, future burdens are discounted at a rate of 3% per year, and the value of the lifetime is weighted so that years of life in childhood and old age are counted less. These choices are explained and discussed in (Murray, 1996 ). Discountingmeans that future gains and losses are counted less than if they had occured today. This is common practice when it comes to valuing material goods. For instance, a bank may require 500 dollars in 10 years time to compensate for a loan of 100 dollars today. However, it is controversial whether if it is correct to apply discounting on human values. It has for instance been asked why future generations should be counted as less valuable.
. Discountingmeans that future gains and losses are counted less than if they had occured today. This is common practice when it comes to valuing material goods. For instance, a bank may require 500 dollars in 10 years time to compensate for a loan of 100 dollars today. However, it is controversial whether if it is correct to apply discounting on human values. It has for instance been asked why future generations should be counted as less valuable.")
56
Age-weights Age weighting means that life years in young and old age are counted less. This figure shows the relative value assigned to each year of life in the calculation of disease burden. Source:World Bank, The relative value of a life year is below one for children under 10, and for persons more than about 55 years of age. This implies that in the calculations, a life year lost for children is given less weight than a life year lost for adults below 55. The adjustments made, introduces (explicitly), a bias both against children and the elderly. In a defence of age-weights, Christopher Murray argues that there is a widespread preference for age weighting in most cultures (Murray, 1996), and, that on average, these preferences can be expressed as in the function given.
, a bias both against children and the elderly. In a defence of age-weights, Christopher Murray argues that there is a widespread preference for age weighting in most cultures (Murray, 1996), and, that on average, these preferences can be expressed as in the function given.")
57
Calculating DALY score, with age weighting and discounting.
Girl, 5 years old, with below-knee amputation who lives until she is 82.5: DALYs= life years lived with disease (77.5) × disability weight (0.3) × age- weight (a1)× discounting factor (3%/year) 77.5 × 0.3 × a1 × d2 = 10.5 DALYs Consider a five-year-old girl with a below-knee amputation after an accident with landmines. DALYs measure life years lost multiplied with a disability weight, multiplied with an age weight a1, multiplied with a discounting factor d2 (3 % for each year). The estimated DALY loss would be 77.5 ( ) years multiplied with 0.3 and adjusted with age weights and the discounting factor which give an estimated 10.5 disability adjusted life years lost.
 × disability weight (0.3) × age- weight (a1)× discounting factor (3%/year) 77.5 × 0.3 × a1 × d2 = 10.5 DALYs. Consider a five-year-old girl with a below-knee amputation after an accident with landmines. DALYs measure life years lost multiplied with a disability weight, multiplied with an age weight a1, multiplied with a discounting factor d2 (3 % for each year). The estimated DALY loss would be 77.5 ( ) years multiplied with 0.3 and adjusted with age weights and the discounting factor which give an estimated 10.5 disability adjusted life years lost.")
58
The Young The 5-year-old girl in the prior example yielded 10.5 DALYs.
However, the DALY score without age-weight and discounting would be 77.5 × 0.3 = 23.3 DALYs This result is twice as high, and would give her a higher priority. The burden of disease (and effect of interventions) for young people, is given less importance by the combined effect of age weighing and discounting. The principle of equal worth of people would require the same age weight for all. It remains an open questions whether the reasons given for departing from equal age weights for all are acceptable. Considering the consequences (children might be given less priority when calculating burden or effect of interventions), it could be seen as an unreasonable (and unnecessary) value judgment.
 for young people, is given less importance by the combined effect of age weighing and discounting. The principle of equal worth of people would require the same age weight for all. It remains an open questions whether the reasons given for departing from equal age weights for all are acceptable. Considering the consequences (children might be given less priority when calculating burden or effect of interventions), it could be seen as an unreasonable (and unnecessary) value judgment.")
59
DALYs - Justice Issues? The DALY approach has been criticised for discriminating the young the elderly the disabled women The approach has been criticized for violating the principle of treating people as equals. In the following these concerns are examined.

60
Finding Health Statistics
WHO - WHO Health Statistics and Health Information Systems website is a rich source of data Data is available by country and by region of the world Could spend the entire semester just mining this data! World Bank Gapminder – World Data MDG related data Gapminder MDG data

61
Figure 2.11: Gross Domestic Product Per Capita and Female Life Expectancy at Birth, Selected Countries, 2004 Data from WHO. Core Health Indicators. Available at: Accessed: September 24, 2006.

62
Hans Rosling Hans Rosling on Health Statistics and Child Mortality
64
Figure 2.9: The Demographic Transition: (A) High Fertility/High Mortality, (B) Declining Mortality/High Fertility, (C) Reduced Fertility/Reduced Mortality Reprinted from U.S. Census Bureau, International Population Reports WP/02, Global Population Profile: Washington, DC: U.S. Government Printing Office; 2004, p. 35.

65
Figure 2.7: Percentage of Children 0 -5 Whose Births Have been Registered, by Income Quintile
Data from UNICEF. Progress for Children: Achieving the MDGs with Equity. Available at: Accessed September 17,

66
Figure 2.8: World Population - 1950 to 2050
Adapted from: Haub, Carl and PRB. Data from United Nations Population Division. World Population Prospects, The 2008 Revision. Available at: Accessed December 4, 2010.

67
Table 2.1: Key Health Status Indicators
Adapted from: Haupt A, Kane TT. Population Handbook. Washington, DC: Population Reference Bureau; 2004; World Bank. Beyond Economic Growth Student Book: Glossary. Accessed April 15, 2007.

68
Table 2.3: The 10 Leading Causes of Death and DALYs 2001
Adapted with permission from Lopez AD, Mathers CD, Murray CJL. The Burden of Disease and Mortality by Condition: Data, Methods, and Results for In: Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL, eds. Global burden of disease and risk factors. Washington, DC and New York: The World Bank and Oxford University Press; 2006.

69
Table 2.4: The Ten Leading Causes of the Burden of Disease in Low- and Middle-income Countries, by Region, 2001 Reprinted with permission from Lopez AD, Mathers CD, Murray CJL. The Burden of Disease and Mortality by Condition: Data, Methods, and Results for In: Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL, eds. Global Burden of Disease and Risk Factors. New York: Oxford University Press 2006:91. Washington, DC and New York: The World Bank and Oxford University Press

70
Table 2.5: The Ten Leading Causes of Death in Children Ages 0-14, by Broad Income Group, 2001
Adapted with permission from: Lopez A, Begg S, Bos E. Demographic and Epidemiological Characteristics of Major Regions, In: Lopez A, Mathers C, Ezzati M, Jamison D, Murray C, eds. Global Burden of Disease and Risk Factors. Washington, DC and New York: The World Bank and Oxford University Press; 2006:70.

71
Table 2.6: The Ten Leading Causes of Death in Adults 15-59, by Broad Income Group, 2001
Adapted with permission from: Lopez A, Begg S, Bos E. Demographic and Epidemiological Characteristics of Major Regions, In: Lopez A, Mathers C, Ezzati M, Jamison D, Murray C, eds. Global Burden of Disease and Risk Factors. Washington, DC and New York: The World Bank and Oxford University Press; 2006:70.

72
Table 2.7: The Ten Leading Causes of Death by Sex, in Low- and Middle-Income Countries, 2001
Data from Lopez A, Begg S, Bos E. Demographic and Epidemiological Characteristics of Major Regions, In: Lopez A, Mathers C, Ezzati M, Jamison D, Murray C, eds. Global Burden of Disease and Risk Factors. Washington, DC and New York: The World Bank and Oxford University Press; 2006:70.

73
Table 2.9: Percentage of the Population Projected to be Over 65 Years of Age
Based on Haub, Carl and PRB. Data from United Nations Population Division. World Population Prospects, The 2008 Revision. Available at: Accessed December 4, 2010.

74
Table 2.12 (cont.): Trends in the Ten Leading Causes of the Burden of Disease, by Income Group, continued Data from World Health Organization. Global Burden of Disease (GBD). Available at: Accessed September 14, 2010.
. Available at: Accessed September 14,")
Similar presentations