Download presentation
Presentation is loading. Please wait.

3
By the end of this lecture the students are expected to: Understand the concept of preload and afterload. Determine factors affecting the end-diastolic volume. Explains how cardiac contractility affects SV,

6
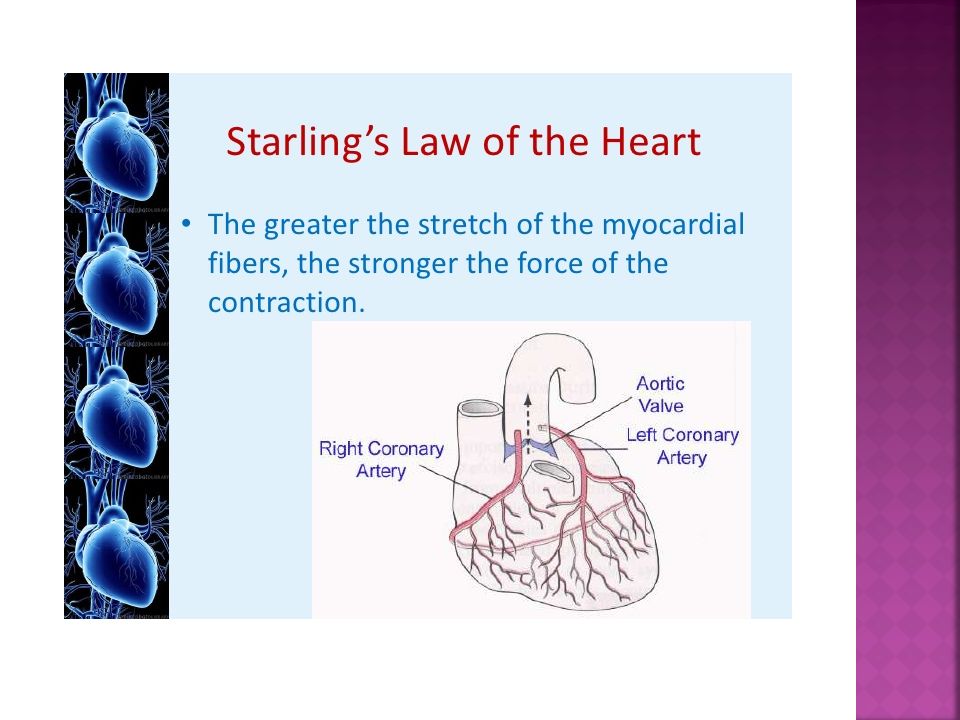
Ability of the heart to change its force of contraction and therefore stroke volume in response to changes in venous return. Also defined as the ability of the heart to pump all blood coming to it without allowing systemic stasis, within limits.

7
Mechanism of Starling Law: An increase in preload lead to an increase in the sarcomere length and increases troponin C calcium sensitivity, which increases the rate of cross-bridge attachment and detachment, and the amount of tension developed by the muscle fiber. This increases SV.

9
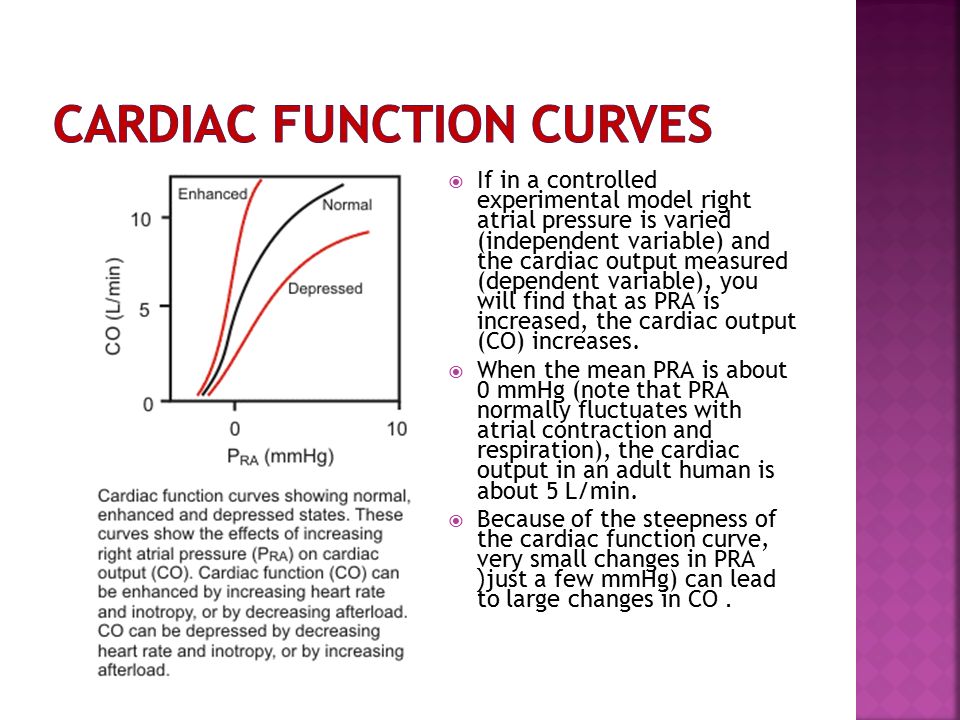
If in a controlled experimental model right atrial pressure is varied (independent variable) and the cardiac output measured (dependent variable), you will find that as PRA is increased, the cardiac output (CO) increases. When the mean PRA is about 0 mmHg (note that PRA normally fluctuates with atrial contraction and respiration), the cardiac output in an adult human is about 5 L/min. Because of the steepness of the cardiac function curve, very small changes in PRA (just a few mmHg) can lead to large changes in CO.
, the cardiac output in an adult human is about 5 L/min. Because of the steepness of the cardiac function curve, very small changes in PRA (just a few mmHg) can lead to large changes in CO..")
10
Increase: - Stronger atrial contraction. -Increased total blood volume -Increased venous tone. -Increased sk m pump. -Increased negative intrathoracic pressure. Decrease: Standing Increased intrapericardial pressure. Decreased ventricular compliance

11
Afterload can be defined as the "load" that the heart must eject blood against. The afterload is closely related to the aortic pressure.

12
When arterial pressure is reduced, the ventricle can eject blood more rapidly, which increases the stroke volume and thereby decreases the end- systolic volume.

13
An increase in afterload, lead to an increase in end-systolic volume and a decrease in stroke volume. An increase in afterload shifts the Frank- Starling curve down and to the right (from A to B). Explanation:, an increase in afterload decreases the velocity of fiber shortening. This reduces the rate of volume ejection so that more blood is left within the ventricle at the end of systole (increase end-systolic volume).A decrease in afterload shifts the Frank-Starling curve up and to the left (A to C).
. Explanation:, an increase in afterload decreases the velocity of fiber shortening. This reduces the rate of volume ejection so that more blood is left within the ventricle at the end of systole (increase end-systolic volume).A decrease in afterload shifts the Frank-Starling curve up and to the left (A to C)..")
14
Vascular tone (and therefore blood pressure) Aortic stiffness Myocardial tension (affected by hypoxia, volume overload) Preload Valvular regurgitation
 Aortic stiffness Myocardial tension (affected by hypoxia, volume overload) Preload Valvular regurgitation")
15
Aortic stenosis. Arterial hypertension

16
1. Nervous: -Sympathetic: HR & SV. - -Parasympathetic: HR 2. Chemical -Potassium -Calcium. -Thyroxin. -Catecholamine.

18
Intrinsic diseases: i.e. originating within the heart include: 1. dilated cardiomyopathy. 2. hypertrophic cardiomyopathy. External factors: These place excessive demands upon the heart: 1.long-term, uncontrolled hypertension, 2.increased stroke volume(volume load; arterial- venous shunts), 3.hormonal disorders such as hyperthyroidism, and pregnancy.
, 3.hormonal disorders such as hyperthyroidism, and pregnancy..")
19
Myocardial infarction Coronary artery disease Valve disease Idiopathic cardiomyopathy Viral or bacterial cardiomyopathy Myocarditis Pericarditis Arrhythmias Chronic hypertension Thyroid disease Septic shock

20
Acute heart failure develops rapidly and can be immediately life threatening because the heart does not have time to undergo compensatory adaptations. Acute failure (hours/days) may result from: 1. cardiopulmonary by-pass surgery, 2. acute infection (sepsis), 3. acute myocardial infarction, 4. severe arrhythmias, etc.
 may result from: 1. cardiopulmonary by-pass surgery, 2. acute infection (sepsis), 3. acute myocardial infarction, 4. severe arrhythmias, etc..")
21
Chronic heart failure is a long-term condition (months/years) that is associated with the heart undergoing adaptive responses (e.g., dilation, hypertrophy) to a precipitating cause. These adaptive responses, however, can be deleterious

22
Neurohormonal mechanisms and compensatory mechanisms in heart failure, BMJ 2000; 320:167-170

23
Renin- angiotensin aldosterone system in HF

24
Effect of natriuretic peptide

25
Common respiratory signs : Tachypnea (increased rate of breathing) and increased work of breathing (non-specific signs of respiratory distress). Rales or crackles, heard initially in the lung bases, and when severe, throughout the lung fields suggest the development of pulmonary edema (fluid in the alveoli). Cyanosis which suggests severe hypoxemia, is a late sign of extremely severe pulmonary edema.
. Cyanosis which suggests severe hypoxemia, is a late sign of extremely severe pulmonary edema..")
26
Additional signs indicating left ventricular failure include: lateral displacement of apex beat (which occurs if the heart is enlarged) gallop rhythm (additional heart sounds) may be heard as a marker of increased blood flow, or increased intra-cardiac pressure.
 gallop rhythm (additional heart sounds) may be heard as a marker of increased blood flow, or increased intra-cardiac pressure.")
28
Pitting peripheral edema, ascites, Hepatomegaly Increased Jugular venous pressure.

31
The control of congestive heart failure symptoms, can be divided into three categories: (1) reduction of cardiac workload, including both preload and afterload; (2) control of excessive retention of salt and water; and (3) enhancement of myocardial contractility.
 reduction of cardiac workload, including both preload and afterload; (2) control of excessive retention of salt and water; and (3) enhancement of myocardial contractility.")
Similar presentations










: Amount of blood pumped by each ventricle per minute. Stroke volume (SV):>")














