Download presentation
Presentation is loading. Please wait.

1
LABORATORIES and DIAGNOSIS of TUBERCULOSIS Assoc. Prof. Alpaslan Alp Hacettepe University Faculty of Medicine Department of Medical Microbiology

3
Tuberculosis Control Program in Turkey: What have been changed in last five years? The Role of Laboratories in National Tuberculosis Control Program New Insights and Developments in Laboratory Procedures

4
Tuberculosis Laboratory Study Group Point of Start: “Global Plan to Stop TB 2006-2015” that had been prepared by Stop-TB partnership and executed by WHO.

5
Tuberculosis Laboratory Study Group Primary Goal: Increase the partnership of public and civilian organizations in order to apply stop TB strategy with all components and create a Turkey without tuberculosis.

6
Tuberculosis Laboratory Study Group Priority Goals of the Study Group: 1.Organization of national tuberculosis laboratory network and standardization of tuberculosis laboratories. 2.Preparation of Diagnosis Handbook for the tuberculosis laboratories within National Control Program. 3.Preparation of Tuberculosis Infection Control Handbook.

7
Goal-1: Organization of national tuberculosis laboratory network and standardization of tuberculosis laboratories. Regulations on Principals of Diagnostic Tuberculosis Laboratories

8
Identification of tests that have to be performed in Level-I, II ve III Diagnostic Tuberculosis Laboratories. Clarification of the duties of National Tuberculosis Reference Laboratory.

9
Regulations on Principals of Diagnostic Tuberculosis Laboratories Level-I Diagnostic Tuberculosis Laboratories: –Acceptance of samples –Direct microscopic examination (AFB staining) –Transport of samples to level-II laboratories.
 –Transport of samples to level-II laboratories.")
10
Regulations on Principals of Diagnostic Tuberculosis Laboratories Level-II Diagnostic Tuberculosis Laboratories: –Processing of samples –Microscopic examination (AFB staining) –Culture –Identification of M. tuberculosis complex and NTM –Susceptibility testing of first line anti- tuberculosis drugs

11
Regulations on Principals of Diagnostic Tuberculosis Laboratories Level-III Diagnostic Tuberculosis Laboratories: –Identification of mycobacteria at species level. –Susceptibility testing of second line anti- tuberculosis drugs –Molecular genotyping

12
Regulations on Principals of Diagnostic Tuberculosis Laboratories National Tuberculosis Reference Laboratory: –Application, control, improvement and quality control of the tests related with diagnosis and treatment of tuberculosis. –Organization of periodical educational programs. –Coordinaion of National Tuberculosis Laboratory Network.

13
Regulations on Principals of Diagnostic Tuberculosis Laboratories Collection of specimens Direct microscopic examination Processing of clinical specimens Culture and identification of M. tuberculosis complex Susceptibility testing of first line anti- tuberculosis drugs Susceptibility testing of second line anti- tuberculosis drugs Susceptibility testing of NTM

14
Regulations on Principals of Diagnostic Tuberculosis Laboratories Molecular methods: –Diagnosis: can be used in smear or culture-negative pulmonary and extra-pulmonary cases in which tuberculosis is highly suspected clinically (specimens such as CSF, bone biopsy, joint fluid). –Identification: can be used as an alternative method to other identification methods in culture-positive specimens for the identification of M. tuberculosis complex and NTM.

15
Regulations on Principals of Diagnostic Tuberculosis Laboratories Molecular methods: –Detection of drug resistance: RIF resistance can be tested in smear-positive specimens in which M. tuberculosis complex detected by molecular methods. –The results of molecular diagnostic or resistance detection tests should be reported to clinician/institution and NTRL in 3 days.

16
Regulations on Principals of Diagnostic Tuberculosis Laboratories Physical Conditions of Laboratories: –Establisment of minimal physical requirements of Diagnostic Tuberculosis Laboratories on the basis of their level to be able to be found and work up.

17
Regulations on Principals of Diagnostic Tuberculosis Laboratories Instruments and Equipments of Laboratories: –Determination of minimal list of instruments and equipment of Diagnostic Tuberculosis Laboratories on the basis of their level to be able to be found and work up.

18
Regulations on Principals of Diagnostic Tuberculosis Laboratories Determination of responsiblities, duties, employment and education of laboratory personnel.

19
Regulations on Principals of Diagnostic Tuberculosis Laboratories Determination of biosafety precautions in tuberculosis laboratories.

20
Regulations on Principals of Diagnostic Tuberculosis Laboratories-2012

21
Goal-2: “Preparation of Tuberculosis Infection Control Handbook” Main Topics: –Administritative controls –Environmental controls Ventilation Filters Ultraviolet radiation –Respiratory protection

22
Goal-3: “Preparation of Diagnosis Handbook for Tuberculosis Laboratory” Main topics will be determined on the basis of Regulations on Principals of Diagnostic Tuberculosis Laboratories.

23
World Health Organization 2009 Report Number of patients who have active tuberculosis: 13.7 million Number of new cases: 9.27 million Number of patients who died because of tuberculosis: 1.76 million

24
These numbers do not tend to decrease in spite of all actions against tuberculosis ! WHY?

25
Routine Laboratory Diagnosis of Tuberculosis Microscopic examination Culture methods –Liquid –Solid

26
Problem…? How can we increase the sensitivity of microscopic examination in a cost-effective manner for the diagnosis of tuberculosis?

27
Smear Microscopy The indispensable of laboratory dşagnosis of tuberculosis: Microscopic examination Fluorescent microscopy, is more sensitive than Ziehl-Neelsen microscopy (%10) and provides faster examination. But it is more expensive and hard to provide continious supply.

29
The Use of LED Microscopy LED: Light-emitting diodes More sensitive than Ziehl-Neelsen microscopy More cost effective and easier than fluorescent microscopy WHO advise the use of LED microscopy instead of fluorescent microscopy.

30
The Use of LED Microscopy Cheaper Consumes less energy (can work with batteries). Bulbs are long-lasting and do not spread toxic materials when broken. Works well in the presence of light.

31
Routine Laboratory Diagnosis of Tuberculosis Microscopic examination Culture methods –Liquid –Solid Molecular methods???

32
Tuberculosis and Molecular Methods Diagnosis of tuberculosis Identification of mycobacteria at species level Detection of drug resistance in M. tuberculosis Genotyping of M. tuberculosis

33
Problem…? What is the value of molecular methods in diagnosis of tuberculosis?

34
Evidence… Examination of scientific literature Experiences

35
Evidence…

36
Ling DI, Flores LL, Riley DW, Pai M. Commercial nucleic acid amplification tests for diagnosis of pulmonary tuberculosis in respiratory specimens: Meta-analysis and meta- regression. PLoS One 2008; 3(2): e1536 Criteria for the examination of papers: NAAT should had been used for the diagnosis of pulmonary tuberculosis; Comparison should had ben done with gold standard culture method; Sensitivity and specificity should had been given; At least 50 specimens should had been involved in the study.
: e1536 Criteria for the examination of papers: NAAT should had been used for the diagnosis of pulmonary tuberculosis; Comparison should had ben done with gold standard culture method; Sensitivity and specificity should had been given; At least 50 specimens should had been involved in the study..")
37
Ling DI, Flores LL, Riley DW, Pai M. Commercial nucleic acid amplification tests for diagnosis of pulmonary tuberculosis in respiratory specimens: Meta-analysis and meta- regression. PLoS One 2008; 3(2): e1536 Number of papers found after initial investigation: 2948 Number of papers that met the criteria and involved for further analysis: 125 Average specimen number: 715 (57-7539)
: e1536 Number of papers found after initial investigation: 2948 Number of papers that met the criteria and involved for further analysis: 125 Average specimen number: 715 ( ).")
38
Ling DI, Flores LL, Riley DW, Pai M. Commercial nucleic acid amplification tests for diagnosis of pulmonary tuberculosis in respiratory specimens: Meta-analysis and meta- regression. PLoS One 2008; 3(2): e1536 RESULTS: Sensitivity and specificities are very variable. Sensitivity: 85% Specificity: 96% There is no meaningful clinical diagnostic linearity.
: e1536 RESULTS: Sensitivity and specificities are very variable. Sensitivity: 85% Specificity: 96% There is no meaningful clinical diagnostic linearity..")
40
Ling DI, Flores LL, Riley DW, Pai M. Commercial nucleic acid amplification tests for diagnosis of pulmonary tuberculosis in respiratory specimens: Meta-analysis and meta- regression. PLoS One 2008; 3(2): e1536 COMMENT: A test grup with such sensitivities can not be used in routine diagnostic applications without any other conventional tests. This test group can only be used as a supportive test to gold standard method.
: e1536 COMMENT: A test grup with such sensitivities can not be used in routine diagnostic applications without any other conventional tests. This test group can only be used as a supportive test to gold standard method..")
41
What kind of PCR Method? Laboratory-made (in house) methods –Optimizable –Cheap Commercial kits –Provide standardization –Optimized for respiratory specimens
 methods –Optimizable –Cheap Commercial kits –Provide standardization –Optimized for respiratory specimens.")
42
What kind of PCR Method? –There is no significant difference between in house methods and commercial kits: Huang TS et al: Comparison of the Amplicor assay and Digene system with in house PCR... J Clin Microbiol 1996, 34:3092- 3096. Yuen KY et al: Comparison of two automated DNA amplification systems with a manual one-tube nested PCR... J Clin Microbiol 1997, 35:1385-1389. Cohen RA et al: Diagnosis of pulmonary tuberculosis using PCR assays on sputum... Am J Respir Crit Care Med 1998, 157:156-161.

44
Flores LL, Pai M, Colford JM, Riley LW. In-house nucleic acid amplification tests for the detection of M. tuberculosis in sputum specimens: Meta-analysis and meta-regression. BMC Microbiol 2005; 5:55. Number of papers found after initial investigation: 2520 Number of papers that met the criteria and involved for further analysis: 84 Average specimen number: 149 (14-727)
.")
45
Flores LL, Pai M, Colford JM, Riley LW. In-house nucleic acid amplification tests for the detection of M. tuberculosis in sputum specimens: Meta-analysis and meta-regression. BMC Microbiol 2005; 5:55. RESULTS: Sensitivity and specificities are very variable. Sensitivity: 9.4% - 100% Specificity: 5.6% - 100% There is no meaningful clinical diagnostic linearity. Clinical diagnostic linearity is higher in studies that used IS6110 region as target region.

47
Flores LL, Pai M, Colford JM, Riley LW. In-house nucleic acid amplification tests for the detection of M. tuberculosis in sputum specimens: Meta-analysis and meta-regression. BMC Microbiol 2005; 5:55. COMMENT: A test grup with such sensitivities can not be used in routine diagnostic applications without any other conventional tests. This test group can only be used as a supportive test to gold standard method.

48
“Evaluation of the value of PCR method in diagnosis of tuberculosis” Alp A, Hasçelik G, Özkara Ş 40th Union World Conference on Lung Health, 2009 Microscopic examination, culture and PCR were performed on the specimens sent to laboratory in a period of two years. Sensitivity of PCR: 80.7% (46/57) Clinical evaluation of 13 specimens that were found as positive by PCR only.
 Clinical evaluation of 13 specimens that were found as positive by PCR only..")
49
“Evaluation of the value of PCR method in diagnosis of tuberculosis” Alp A, Hasçelik G, Özkara Ş 40th Union World Conference on Lung Health, 2009 Tuberculosis treatment was initiated to seven of these patients, on the basis of PCR positivity. All of these 7 specimens were extra-pulmonary specimens. Result: –PCR can be only a supportive test for the diagnosis of tuberculosis in pulmonary specimens. –The use of PCR can be more helpful for the diagnosis of tuberculosis in extra-pulmonary specimens.

50
“Is PCR an essential method for the diagnosis of tuberculosis in a routin laboratory” Alp A, Hasçelik G, ASM 110th General Meeting, 2010 Microscopic examination, culture and PCR were performed on the specimens sent to laboratory in a period of three years. Sensitivity of PCR in respiratory specimens: 72% Sensitivity of PCR in extra-pulmoray specimens: 76% Comment: PCR, with these sensitivity levels, is far from being a helpful diagnostic tool in routine laboratories.

51
Isn’t there any promising new method? Xpert MTB/RIF Assay LAMP (Loop Mediated Isothermal Amplification Test) Microarray designs Discovery of regulatory RNAs (siRNA)
 Microarray designs Discovery of regulatory RNAs (siRNA).")
52
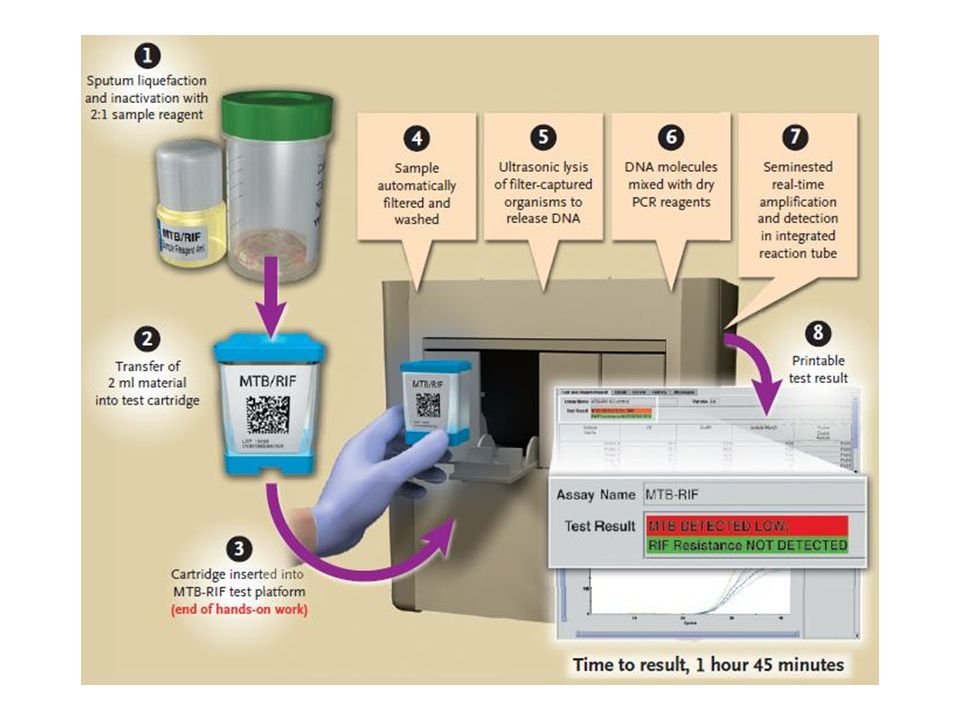
Xpert MTB/RIF Assay Product of a collaborative study: –FIND (Foundation for Innovative New Diagnostics) –Cepheid (USA) –University of Medicine and Dentistry of New Jersey Detection of M. tuberculosis and rifampicin resistance in two hours. A “hemi-nested real-time PCR” that uses three primers and five probes.

54
Xpert MTB/RIF Assay Satisfactory results were obtained in the studies that were performed in 2010: Sensitivity in smear-positive culture-positive specimens: 99% Sensitivity in smear-negative culture-positive specimens: 90%

56
Xpert MTB/RIF Assay Meta-Analysis Study Eighteen study had been chosen among 90 studies. A total of 10.224 specimen –2983 bacteriological TB diagnosis –6183 smear and culture-negative Average sensitivity for diagnosis of TB: 90.4% Average specificity for diagnosis of TB : 98.4%

57
Xpert MTB/RIF Assay Meta-Analysis Study Average sensitivity for detection of rifampicin resistance: 94.1% Average specificity for detection of rifampicin resistance: 97.0% Average sensitivity in extra-pulmonary specimens: 80.4% Average specificity in extra-pulmonary specimens : 86.1%

58
Xpert MTB/RIF Assay Meta-Analysis Study COMMENT: Xpert MTB/RIF assay fulfills the requirements of rapidly and effectively diagnosing TB and RIF resistance. Since the mutation points in 5% RIF-resistant Mtb isolates occur outside core gene region, they would not be identified by Xpert MTB/RIF assay.

59
WHO Evaluation on Xpert MTB/RIF Assay-2011 Xpert MTB/RIF assay: –Analytical sensitivity: 5 genome copies/purified DNA or 131 cfu/ml sputum (10-100 cfu/ml sputum for culture)
")
60
WHO Evaluation on Xpert MTB/RIF Assay-2011 Average detection time: –Solid culture: >30 days –Liquid culture: 17 days –Microscopy: 1 day –Xpert MTB/RIF: <1 day

61
WHO Evaluation on Xpert MTB/RIF Assay-2011 Recommendations: Xpert MTB/RIF should be used as the initial diagnostic test in individulas suspected of MDR- TB or HIV-associated TB. Xpert MTB/RIF may be used as a follow-on test to microscopy in settings where MDR and/or HIV is of lesser concern, especially in smear- negative specimens.

62
WHO Evaluation on Xpert MTB/RIF Assay-2011 Recommendations: Xpert MTB/RIF assay does not eliminate the need for conventional microscopy, culture and drug susceptibility testing.

63
Xpert MTB/RIF Assay Disadvantages when evaluated on the basis of the standards determined by WHO: –Shelf-life of kits is not more than14 months –Instrument needs annual maintenance –Instrument does not work with batteries –The test is simple but there is a high level technology –Not cheap

Similar presentations