Download presentation
Presentation is loading. Please wait.

1
Laparoscopic Day Surgery: The American Experience Alfons Pomp, MD, FACS Weill Medical College of Cornell University

2
CHUM Hotel-Dieu Montreal

3
Ambulatory/Day Surgery Same day discharge (< 23 hour stay) Physician office, ambulatory surgical centers (ASC) and hospital based outpatient 1990’s American Hospital Insurance Programs looked at risk/benefit of the economics Standard of care…safe outcomes? Nonetheless 60-70% operations are performed as outpatient procedures

4
Weill Cornell NYP Hospital

5
Mandate: The American Experience Ambulatory Surgery (hernia/cholecystectomy) Reflux surgery Bariatrics -Banding -Gastric bypass Surgery of increasing complexity in more fragile patients
 Reflux surgery Bariatrics -Banding -Gastric bypass Surgery of increasing complexity in more fragile patients")
6
What is the risk of having an operation No one really knows Netherlands (Arbous et al 2001) 800,000 pts 8.8/10,000 mortality (1.4 due to anesthesia) USA (Fleisher et al 2004) 564,267 Medicare procedures; 7 day mortality rates 4.1/10,000;
 800,000 pts 8.8/10,000 mortality (1.4 due to anesthesia) USA (Fleisher et al 2004) 564,267 Medicare procedures; 7 day mortality rates 4.1/10,000;")
7
Operative Risks data taken from inpatient procedures Associated with patient factors Associated with anesthesia Associated with the surgical procedure Associated with doing the procedure as ambulatory/day surgery

8
Patient Factors: Age Age (>65 years) adverse intra-op events/not post-op events hypertension: intra-op cardiovascular events unanticipated readmission rates Age (85 years) co-morbidity, hospitalization < 6 months
 adverse intra-op events/not post-op events hypertension: intra-op cardiovascular events unanticipated readmission rates Age (85 years) co-morbidity, hospitalization < 6 months")
9
Patient Factors Hyper-reactive airway disease (asthma, COPD, smoking) Coronary artery disease(IHD, MI, CHF,BP) Obesity Obstructive sleep apnea Diabetes
 Coronary artery disease(IHD, MI, CHF,BP) Obesity Obstructive sleep apnea Diabetes")
10
Diabetes 80% type II/ 80% are obese: associated with increase in unplanned admissions Poor control associated with increased rate of surgical complications

11
Diabetes Understand disease/ measure BS at home Treatment of hypoglycemia No recurrent admission with complications related to diabetes Hb1Ac >8 unsuitable > 9 not any elective surgery Metformin associated with lactic acidosis

12
American Society of Anesthesia (ASA) Class Class 1 Healthy patient, no medical problems Class 2 Mild systemic disease Class 3 Severe systemic disease, but not incapacitating Class 4 Severe systemic disease that is a constant threat to life Class 5 Moribund, not expected to live 24 hours irrespective of operation An e is added to designate an emergency operation.
 Class Class 1 Healthy patient, no medical problems Class 2 Mild systemic disease Class 3 Severe systemic disease, but not incapacitating Class 4 Severe systemic disease that is a constant threat to life Class 5 Moribund, not expected to live 24 hours irrespective of operation An e is added to designate an emergency operation.")
13
Anesthesia analgesia/amnesia/paralysis Anxiety Pain afferent, inflammation Consciousness Autonomic stimulation Memory Movement

14
PONV (Post-anesthesia nausea/vomiting) Common cause of unplanned admissions Risk factors intra-peritoneal gas bowel manipulation female gender history of motion sickness opiates
 Common cause of unplanned admissions Risk factors intra-peritoneal gas bowel manipulation female gender history of motion sickness opiates")
15
PONV Prevention Pre-induction anti-emetics Short term induction anesthetics Volatile anesthetics (sevoflurane) Short acting muscle relaxants Analgesia portals, intra-peritoneal spray NSAIDS/ketorolac
 Short acting muscle relaxants Analgesia portals, intra-peritoneal spray NSAIDS/ketorolac")
16
Post-anesthesia Discharge Scoring System Vital signs Activity level Nausea and vomiting Pain Surgical care

17
Are ambulatory risks higher than inpatient? 5-8% of procedures are performed in MD’s office w/o federal regulations, moderate rates of “readmission” ASC have lowest adverse outcome Highest rates of readmission and deaths are surgeries performed as outpatient in hospital setting

18
Ambulatory Surgery Risk Factors ASA class Advanced age (> 85 years) Inpatient admission history Surgical procedure complexity (time) Medical causes account for less than 20% of admissions
 Inpatient admission history Surgical procedure complexity (time) Medical causes account for less than 20% of admissions")
19
Ambulatory Surgery Risk Factors Hyper-reactive airway disease (smoking) Coronary artery disease (functional) Diabetes Obesity Obstructive sleep apnea
 Coronary artery disease (functional) Diabetes Obesity Obstructive sleep apnea")
20
Ambulatory Surgery 90 minutes/6 hour recovery time Reflux operations -Nissen Bariatric operations-Banding 90 minutes/23 hour discharge time Bariatric operations-LRYGBP

21
Day Case Laparoscopic Nissen Fundoplication Patient selection Anesthesia protocols Discharge rates and time Postoperative complications/re-admissions Ng et al ANZ J Surg 2005

22
Nissen Fundoplication ASA grade I-II (patient bias selection) 30 minute drive from the hospital Obesity Asthma Age
 30 minute drive from the hospital Obesity Asthma Age")
23
Nissen Fundoplication Pre-emptive analgesia Anti-emetics Propofol as induction, variable maintenance Local anesthesia in the wounds Post-operative reviews

24
Nissen Fundoplication > 90% discharge rate most studies 6-7 hrs cardiovascular stability clear fluids adequate pain control able to ambulate

25
Nissen Fundoplication 1-11% re-admission rate dysphagia/inability to tolerate fluid comparable to hospitalized patients 86% patients have resolution of symptoms 1.5-3 days US $2500-3400/case

26
Bariatric Explosion Epidemic of obesity Laparoscopic approach Publicity / media Patient demand Schirmer, B. Watts, S.H. Laparoscopic Bariatric Surgery Surg Endosc 2003

27
Bariatric Surgery-USA 1994-1999 10-15,000/year 2000 22,000 2001 48,000 2002 75,000 2003 105,000 2004 140,000 (450,000 lap cholecystectomies) Schirmer B., Watts S.H., Surg Endosc 2003
 Schirmer B., Watts S.H., Surg Endosc 2003")
28
Surgery for Obesity WLS today – Restriction – Malabsorption 4 operations - Lap band – Sleeve gastrectomy – Gastric bypass – Duodenal Switch

29
Surgical Procedures: Laparoscopic Adjustable Gastric Banding Inflatable gastric band just distal to G-E junction Purely restrictive procedure “Reversible” Technically “simple”

30
Gastric Banding 343 patients 4/2003-1/2005 Contra-indications cardiac co-morbidity pulmonary co-morbidity poorly controlled diabetes ( + all > 60) anticoagulation impaired mobility Watkins B. M. et al Obesity Surgery 2005

31
Gastric banding 4.5 –13.5kg pre-op weight loss DVT prophylaxis Anesthesia scopolamine/IV rantidine/ondansetron local bupivacaine/ketorolac/dexamethasone liquid hydrocodone/acetaminophen

32
Gastric banding 305 females/38 males 43.5 years/BMI 44.5 OR 53 minutes 8.2 % paid by insurance company 10 complications 5 occlusions treated medically colon perforation 3 transfers to hospital

33
15-30 cc Pouch 100-150 cm Roux limb Roux-en-Y Gastric Bypass

34
Gastric bypass 2000 patients LRYGBP 10/2001-12/2004 Average BMI 49 Female to male ratio 7:1 OR times 54-115 minutes average 1669 (84%) discharged within 23 hours McCarty T.M. et al Annals of Surgery 2005

35
Gastric bypass Early complications (<30 days) stricture, bleeding, leaks, PE (0.8%,0.3%,0.2%,0.1%) Late complications internal hernias, stricture, G-G fistula (2.5%,1.3%,0.2%) 2 mortalities: hemorrhage /sepsis
 stricture, bleeding, leaks, PE (0.8%,0.3%,0.2%,0.1%) Late complications internal hernias, stricture, G-G fistula (2.5%,1.3%,0.2%) 2 mortalities: hemorrhage /sepsis")
36
Gastric bypass Predictive of discharge surgeon experience (>50 cases) patient age (<56) BMI <60 weight < 400 lbs (180 kg) co-morbidities < 4 intra-operative steroid bolus
 patient age (<56) BMI <60 weight < 400 lbs (180 kg) co-morbidities < 4 intra-operative steroid bolus")
37
Gastric bypass Lessons learned KEEP RATE OF COMPLICATIONS LOW Circular stapler 25mm/ Linear Stapler Staple buttress Internal hernias less with ante-colic approach Intra-operative steroids

39
Gastric bypass National Hospital Discharge Survey 10% complication rate LOS 7 days Variability: open procedure, clinical care pathways to reduce pain, nausea, narcotic requirements and complications Livingston E.H. Am J Surg 2004

40
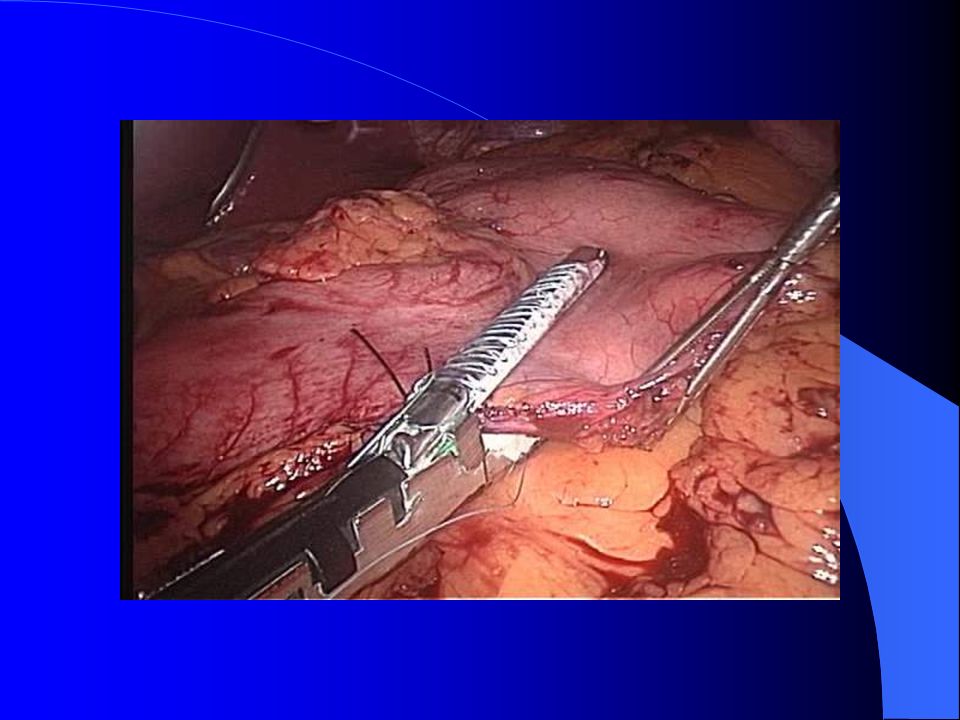
Laparoscopic Day surgery for Liver Resection 17 patients, no conversions 2002-2004 Anterior and medial segments of the liver Tissuelink, GIA stapler, intra-op U/S 11 patients averaged 14 hours stay 5 segmentectomies OP time 174 minutes

41
Decreased pain and wound related morbidity Short hospital stay in appropriate patients (lower ASA scores) Learn P. et al J Gastrointestinal Surgery 2006

42
Successful discharge meticulous surgery, low complication rate Post-operative pain and nausea Pre-operative analgesia Anti-emetics Standardized anesthesia protocols short acting agents

43
Successful Discharge Information prior to the procedure Written instructions on discharge Home contact monitor progress, reassure detect early problems Self referral to surgical team-minimal delay

44
Conclusions Attractive to the surgeon reduce waiting times decreases cancellations due to bed shortage COST-EFFECTIVE Attractive to the patient? PONV, pain, anxiety (help) addressed
 addressed.")
45
Un grazie (di cuore) Alfons Pomp, MD, FACS
 Alfons Pomp, MD, FACS")
Similar presentations


, A Soprani(1,2), Tabbara M (2), J Cady (1) 1- Clinique Geoffroy Saint Hilaire (Paris), 2- Service de Chirurgie Digestive et Hépato-Bilio-Pancréatique,>")
















