Download presentation
Presentation is loading. Please wait.

1
Post-Surgical Care of the Bariatric Patient
Eve L. Olson, MD Medical Director St. Francis Weight Loss Center Indianapolis, Indiana

2
Obesity Trends* Among U.S. Adults BRFSS, 1990, 1999, 2008
(*BMI 30, or about 30 lbs. overweight for 5’4” person) 1990 1999 2008 No Data <10% %–14% %–19% %–24% %–29% ≥30%
 No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%")
3
↑ 1000% ↑ 500% ↑ 300%

6
Number of Bariatric Operations performed in the US from 1992-2006
NEJM, R. Steinbrook, 2004/ ASBS

7
Who Qualifies for Weight-Loss Surgery?
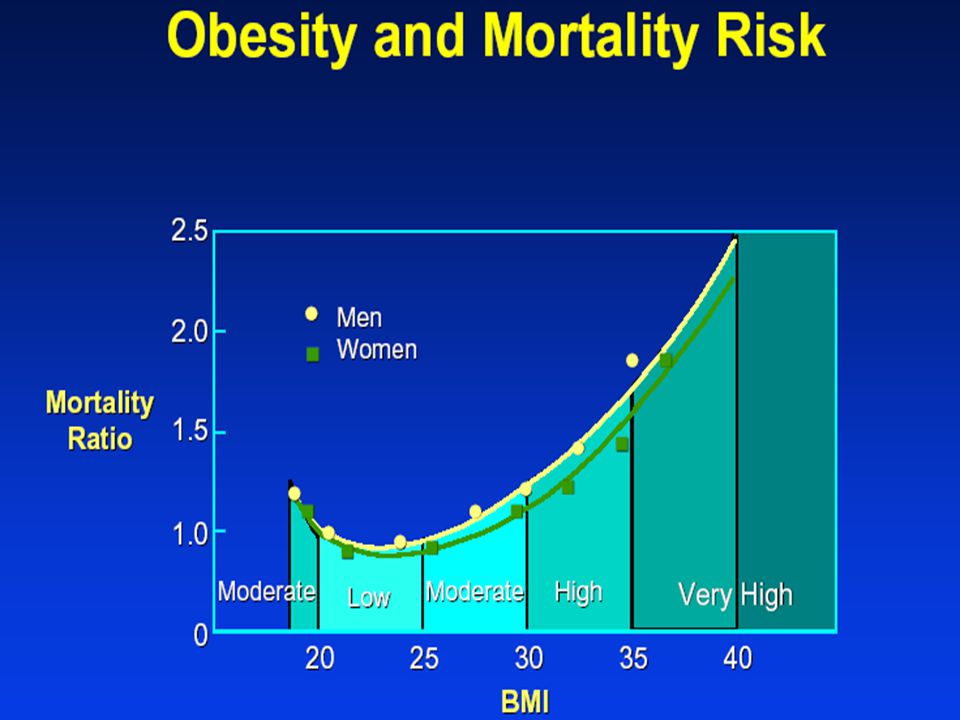
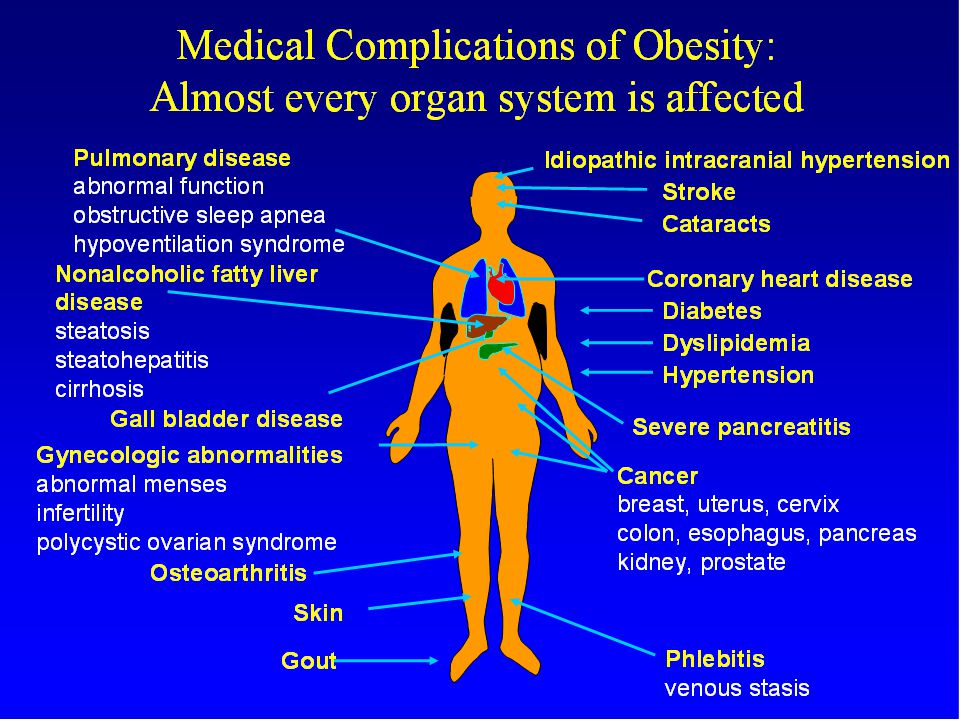
Clinical Terms Used to Describe Various Levels of Body Fat Normal Weight (BMI 18.5 to 24.9) Overweight (BMI 25 to 29.9) Obese (BMI 30 to 34.9) Severely Obese (BMI 35 to 39.9 ) Morbidly Obese (BMI 40 or more) There are clinical terms used to describe people’s levels of body fat to see if they are candidates for weight-loss surgery. The ideal BMI ranges from 19 to 25. If your BMI is between 25 and 29.9, you are thought to be overweight. If it is between 30 and 39.9, you are obese. If your BMI is 40 or more, you are said to have morbid obesity. The term “morbid” obesity is used because this degree of excess weight may considerably reduce life expectancy and is associated with an increased risk of developing conditions or diseases such as diabetes, high blood pressure, joint problems, gallstones, stroke, heart disease, and psychosocial problems. Severely and morbidly obese patients are considered candidates for weight-loss surgery. BMI>40 BMI BMI BMI BMI 7
 Overweight (BMI 25 to 29.9) Obese (BMI 30 to 34.9) Severely Obese (BMI 35 to 39.9 ) Morbidly Obese (BMI 40 or more) There are clinical terms used to describe people’s levels of body fat to see if they are candidates for weight-loss surgery. The ideal BMI ranges from 19 to 25. If your BMI is between 25 and 29.9, you are thought to be overweight. If it is between 30 and 39.9, you are obese. If your BMI is 40 or more, you are said to have morbid obesity. The term morbid obesity is used because this degree of excess weight may considerably reduce life expectancy and is associated with an increased risk of developing conditions or diseases such as diabetes, high blood pressure, joint problems, gallstones, stroke, heart disease, and psychosocial problems. Severely and morbidly obese patients are considered candidates for weight-loss surgery. BMI>40. BMI BMI BMI BMI")
8
Bariatric Surgery Indications NIH Criteria
BMI > 40 BMI > 35 with Co-morbidities Type II Diabetes Obstructive Sleep Apnea Coronary Artery Disease Cardiomyopathy Hypertension Dyslipidemia

9
Restrictive Procedures
Gastric Banding Sleeve Gastrectomy

10
Restrictive + Malabsorptive Procedures
Roux-en-Y Gastric Bypass Biliopancreatic Diversion with Duodenal Switch

11
Efficacy of Bariatric Surgery for Weight Loss
Mean percentage excess weight loss: 61.2% - All Patients 47.5% - Gastric Banding 61.6% - Gastric Bypass 70.1% - BPD or duodenal switch *Buchwald H, et al. Bariatric Surgery: A Systematic Review and Meta-analysis. JAMA, 14: , 2004

12
Weight Maintenance after Bariatric Surgery
Sjöström L, Lindroos AK, Peltonen M et al. N Engl J Med. 2004;351:26

13
Comparing Weight-Loss Results
Gastric Bypass LAP-BAND Although initial weight loss with Gastric Bypass is typically very rapid, surgeons report that at 5 years many LAP-BAND and Gastric Bypass patients achieve comparable weight loss results. 55% of excess weight for the LAP-BAND versus 59% with Gastric Bypass. Source: O’Brien et al. Obesity is a Surgical Disease: Overview of Obesity and Bariatric Surgery, ANZ J Surg, 2004; 74: 13

16
Long-term Survival with Bariatric Surgery
Rel. Risk = 0.11 ( ) 89% reduction in risk of death over 5 years % Mortality Long-term survival: Canada In addition to this study by Christou et al.,1 there have been a number of other published studies or abstracts documenting a decreased mortality after bariatric surgery when compared to matched cohorts.2-7 Most of the improvement is due to decreased diabetes, myocardial infarction, and cancer-related deaths. References: Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240: MacDonald KG Jr, Long SD, Swanson MS, et al. The gastric bypass operation reduces the progression and mortality of non-insulin-dependent diabetes mellitus. J Gastrointest Surg. 1997;1: Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199: Sjostrom L. Soft and hard endpoints over 5 to 18 years in the intervention trial Swedish obese subjects (abstract). Obesity Reviews. 2006;7 S2:27. Peeters A, O'Brien P, Laurie C, et al. Does weight loss improve survival? Comparison of a bariatric surgical cohort with a community based control group (abstract). Obesity Reviews. 2006;7 S2:95. Adams T, Gress R, Smith S, et al. Long-term mortality following gastric bypass surgery (abstract). Obesity Reviews. 2006;7 S2:94. Busetto L, Mazza M, Miribelli D, et al. Total mortality in morbid obese patients treated with laparoscopic adjustable gastric banding: A case-control study (abstract). Obesity Reviews. 2006;7 S2:95. Christou et al. Ann Surg 2004;240: 16
 89% reduction in risk of death over 5 years. % Mortality. Long-term survival: Canada In addition to this study by Christou et al.,1 there have been a number of other published studies or abstracts documenting a decreased mortality after bariatric surgery when compared to matched cohorts.2-7 Most of the improvement is due to decreased diabetes, myocardial infarction, and cancer-related deaths. References: Christou NV, Sampalis JS, Liberman M, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg. 2004;240: MacDonald KG Jr, Long SD, Swanson MS, et al. The gastric bypass operation reduces the progression and mortality of non-insulin-dependent diabetes mellitus. J Gastrointest Surg. 1997;1: Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199: Sjostrom L. Soft and hard endpoints over 5 to 18 years in the intervention trial Swedish obese subjects (abstract). Obesity Reviews. 2006;7 S2:27. Peeters A, O Brien P, Laurie C, et al. Does weight loss improve survival Comparison of a bariatric surgical cohort with a community based control group (abstract). Obesity Reviews. 2006;7 S2:95. Adams T, Gress R, Smith S, et al. Long-term mortality following gastric bypass surgery (abstract). Obesity Reviews. 2006;7 S2:94. Busetto L, Mazza M, Miribelli D, et al. Total mortality in morbid obese patients treated with laparoscopic adjustable gastric banding: A case-control study (abstract). Obesity Reviews. 2006;7 S2:95. Christou et al. Ann Surg 2004;240:")
17
Chronological case order per surgeon
Relationship Between Surgical Experience and Perioperative Mortality in Gastric Bypass Surgery 7% 6% 5% 4% 3% 2% 1% 0% 125 case lifetime bariatric surgery experience Thirty Day Mortality Relationship between surgical experience and perioperative mortality in gastric bypass surgery Because of the increased mortality with decreased experience, as well as the lack of quality in some programs, accreditation of bariatric surgery programs has been developed with the Surgical Review Corporation (SRC) founded by the American Society for Bariatric Surgery and the American College of Surgeons. Medicare patients must be referred to one of these approved programs. Mandatory outcomes data reporting will permit further quality assurance and improvements in the surgical care of the severely obese patient. The SRC centers who have achieved full approval have a very low mortality rate, 0.35% at 90 days after surgery, as compared to much higher rates in other studies.1-3 References: Pratt GM, McLees B, Pories WJ. The ASBS Bariatric Surgery Centers of Excellence program: a blueprint for quality improvement. Surg Obes Relat Dis. 2006;2: Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199: Flum DR, Salem L, Elrod JA, Delliniger EP, Cheadle A, Chan L. Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures. JAMA. 2005;294: 50 100 150 200 250 300 350 400 450 500 550 600 650 Chronological case order per surgeon D Flum et al. J Am Coll Surg 199:543, 2004 17
 founded by the American Society for Bariatric Surgery and the American College of Surgeons. Medicare patients must be referred to one of these approved programs. Mandatory outcomes data reporting will permit further quality assurance and improvements in the surgical care of the severely obese patient. The SRC centers who have achieved full approval have a very low mortality rate, 0.35% at 90 days after surgery, as compared to much higher rates in other studies.1-3. References: Pratt GM, McLees B, Pories WJ. The ASBS Bariatric Surgery Centers of Excellence program: a blueprint for quality improvement. Surg Obes Relat Dis. 2006;2: Flum DR, Dellinger EP. Impact of gastric bypass operation on survival: a population-based analysis. J Am Coll Surg. 2004;199: Flum DR, Salem L, Elrod JA, Delliniger EP, Cheadle A, Chan L. Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures. JAMA. 2005;294: Chronological case order per surgeon. D Flum et al. J Am Coll Surg 199:543,")
18
Is Bariatric Surgery Safe?
Mortality rates after common operations in U.S. hospitals Variable Repair of CABG Pancreatic Hip Replacement ASMBS BSCOE AAA Surgery surgery surgery bariatric surgery Hospitals operation (n) Avg. mortality rate (%) Average hospital caseload Adapted from Dimick J.B., Welch H.G., Birkmeyer, J.D. Surgical mortality as an indicator of hospital quality. JAMA 2004; 292:
 Avg. mortality rate (%) Average hospital caseload. Adapted from Dimick J.B., Welch H.G., Birkmeyer, J.D. Surgical mortality as an indicator of hospital quality. JAMA 2004; 292:")
19
Patient outcomes for all Bariatric Surgeries at
235 SRC Full Approval BSCOE Hospitals

20
Recognizing Complications
Over-medication Anti-hypertensives Diabetic Medications Under-medication Anti-seizure Dehydration Most common first two weeks post-op No Thirst

21
Postoperative Complications Common to all Procedures
General Complications Pulmonary embolism Incisional hernia Gallstone formation Major wound infection and seroma Abdominal fluid collection Subphrenic abscess Peritonitis

22
Procedure-Specific Complications (RYGB)
Anastomotic or staple-line leak Acute gastric distention Staple-line disruption Stomal stenosis Stomal ulceration Small-bowel obstruction Occlusion of Roux limb Dumping

23
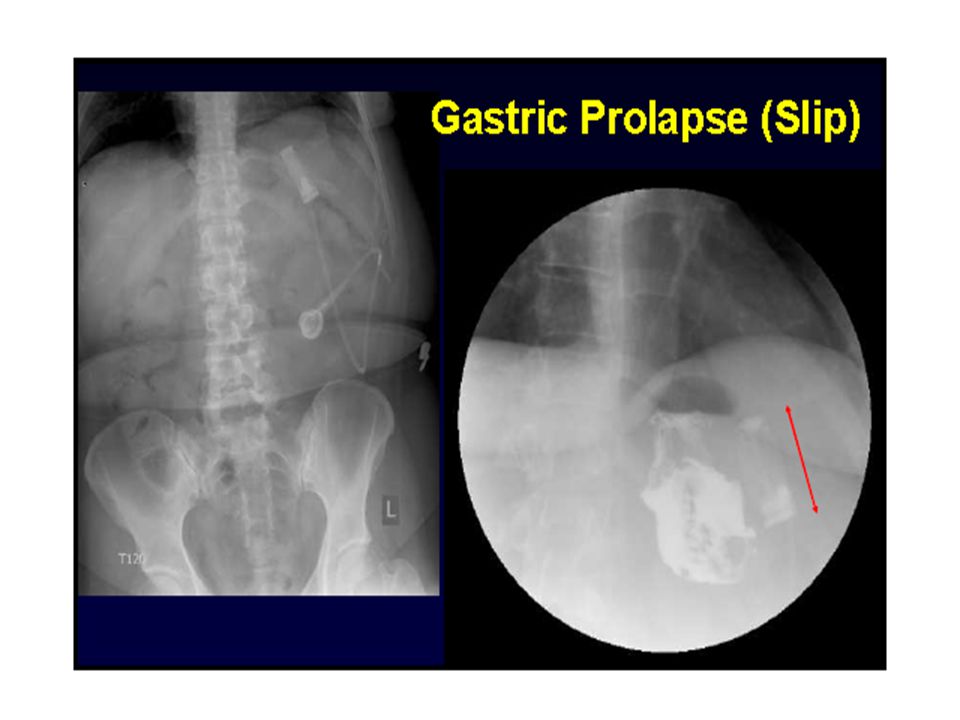
Procedure-Specific Complications ( gastric banding)
band slippage esophageal dilatation erosion of the band into the stomach band or port infections balloon or system leaks that can diminish weight loss

26
Band Erosions Partial Complete

30
Normal Absorption

31
Risk of Vitamin and Mineral Deficiencies Post-op
Calcium and Vitamin D Reduced absorption d/t bypassed duodenum, proximal jejunum (R-en-Y) Life-long supplements mandatory Iron Absorption decreased d/t decreased contact of food with gastric acid; reduced conversion of iron from ferrous to ferric form (MVI) Vitamin B12 Absorption decreased d/t decreased contact with intrinsic factor 60% of patients require long term supplementation of B12 Thiamine Connection to Wernicke’s syndrome Cases not well documented
 Life-long supplements mandatory. Iron. Absorption decreased d/t decreased contact of food with gastric acid; reduced conversion of iron from ferrous to ferric form (MVI) Vitamin B12. Absorption decreased d/t decreased contact with intrinsic factor. 60% of patients require long term supplementation of B12. Thiamine. Connection to Wernicke’s syndrome. Cases not well documented.")
32
Question and Comments

Similar presentations