Download presentation
Presentation is loading. Please wait.

1
Causes Myocardial dysfunction eg IHD, CM Volume overload eg AR, MR Obstruction eg AS, HCM Diastolic dysfunction eg Constriction Mechanical problems eg LV aneurysm Rhythm disturbance eg A fib High output eg anaemia, shunts, thyrotox Definition Cardiac output that is insufficient to meet the needs of the body

5
Heart failure symptoms SOBE Orthopnoea, PND Ankle swelling Anorexia, weight loss Cold peripheries Tiredness Heart failure signs Tachycardia, hypotension Raised JVP, S3 May be PSM of MR (or TR) Basal crepitations Ankle oedema Not useful to divide into right and left heart failure
 Basal crepitations Ankle oedema Not useful to divide into right and left heart failure")
7
ECG, CXR, Echo ECG often abnormal –Previous MI, LBBB, Non-specific ST/T abnormalities –If ECG normal unlikely to be systolic dysfunction CXR cardiomegaly –Upper lobe diversion, fluid in horizontal fissure, Kerly B lines, pleural effusions Echocardiography –Confirms / refutes diagnosis of systolic dysfunction –Can assess diastolic dysfunction

9
Treatment – Acute heart failure Sit up High dose oxygen Intravenous loop diuretic Venodilation eg intravenous GTN Possibly intravenous diamorphine (Aminophylline, venesection) Intubation and ventilation Cardiogenic shock Severe hypotension Poor tissue perfusion - Oliguria, Confusion Mortality 80%+ Inotropes eg Dopamine, Dobutamine IABP +/- angioplasty if cardiac ischaemia
 Intubation and ventilation Cardiogenic shock Severe hypotension Poor tissue perfusion - Oliguria, Confusion Mortality 80%+ Inotropes eg Dopamine, Dobutamine IABP +/- angioplasty if cardiac ischaemia")
10
Chronic heart failure - Mortality

11
Treatment – Chronic heart failure Salt restriction Fluid restriction Diuretics –Usually loop diuretics –Occasionally add thiazides May lead to excessive diuresis, electrolyte imbalance Amiloride, triamtarene may prevent low K

12
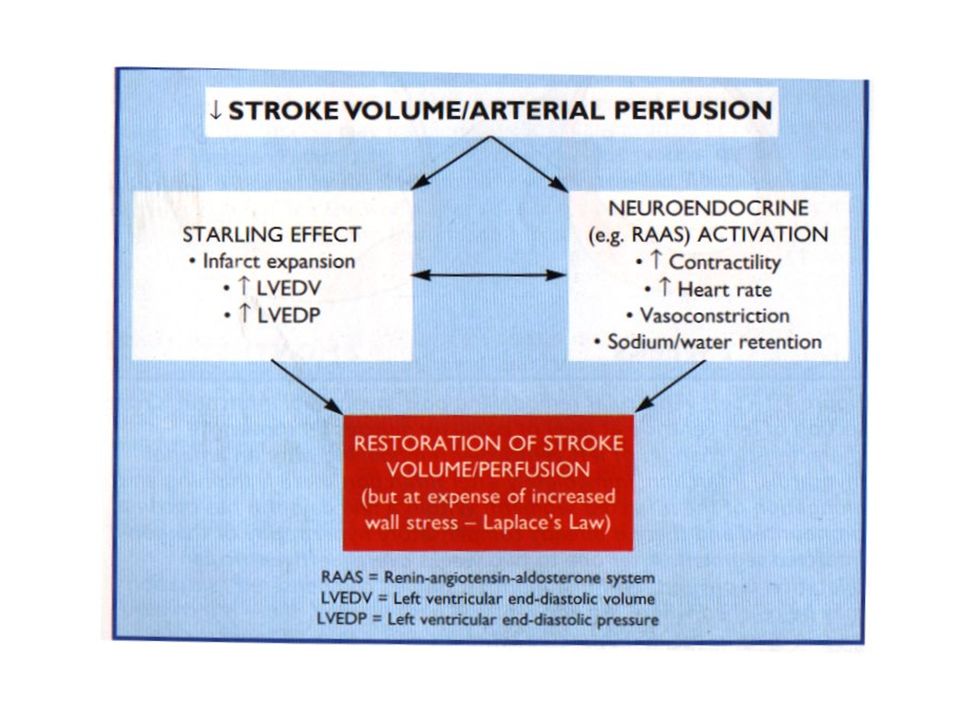
Treatment – vasodilators Reduce preload / afterload –ACEI Reduce morbidity and mortality Interact with RAAS Prevent adverse remodelling post MI May precipitate renal failure Cough in 10-15% (consider AII blockers) –Nitrates and hydralazine Reduce morbidity / mortality but less than ACEI
 –Nitrates and hydralazine Reduce morbidity / mortality but less than ACEI")
13
Treatment - inotropes Digoxin –Reduces hospital admissions –No reduction in mortality –Stopping may precipitate deterioration All other oral positive inotropes to date have caused an increased mortality Treatment – beta blockers Recent studies suggest beta-blockers improve morbidity and mortality Similar degree to ACEI and additive Possibly via reduction in sympathetic activation May precipitate pulmonary oedema –Start low doses and slowly titrate up

14
Treatment - spironolactone Recently shown to improve mortality in severe heart failure Probably via blockage of aldosterone May precipitate hyperkalaemia and renal failure

15
Heart failure rule of halves

16
Diastolic heart failure Up to a third of patients have clinical heart failure with normal LV systolic function Underlying pathophysiology relates to diastolic dysfunction Commonest underlying pathologies –Normal ageing, Hypertension, Myocardial ischaemia Mechanisms of diastolic dysfunction Impaired ventricular relaxation –Energy dependent process –Susceptible to myocardial ischaemia Decreased myocardial compliance –Altered compliance mediated by collagen –Fibrosis related to activation of RAAS

17
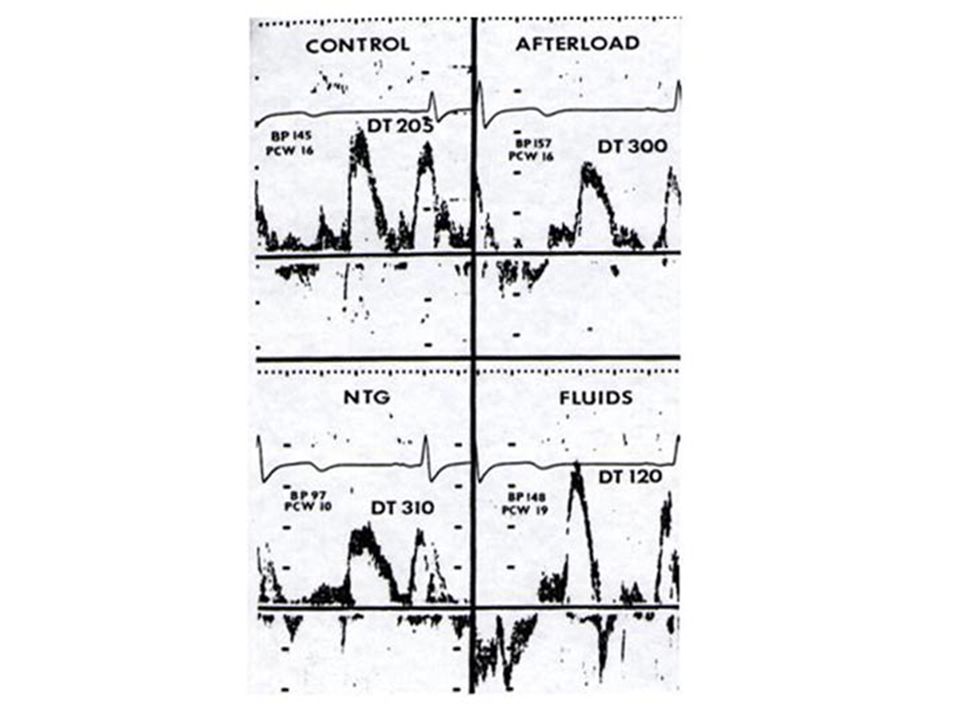
Doppler patterns of diastolic dysfunction Impaired relaxation –Reduced E/A ratio –Increased EDT –Increased IVRT Restriction –LA pressure increases due to myocardial stiffness –High peak E wave velocity –Short EDT –Very short IVRT

20
Treatment of diastolic heart failure Treat underlying cause eg ischaemia Impaired relaxation –Theoretically rate-limiting agents effective Beta-blockers, verapamil Reduce HR and prolong diastole Reduce myocardial oxygen demand Lower BP and reduce LVH Restriction –Drugs which reduce fibrosis and lower LA pressure theoretically should be effective ACEI, AII blockers, Diuretics –If LA pressure lowered too much cardiac output significantly worsened Can cause significant morbidity

Similar presentations





 Heart failure is the pathophysiological state in which an abnormality of cardiac function is responsible for failure of the heart to.>")







 CPP = aortic diastolic.>")








, Dip. Diab.DCA, Dip. Software statistics PhD (physio)>")

