Download presentation
Presentation is loading. Please wait.

1
M. Wissmeyer Department of Nuclear Medicine, University of Berne (Inselspital) PET/CT in Radiation Oncology: Current Evidence and Future Perspectives
 PET/CT in Radiation Oncology: Current Evidence and Future Perspectives.")
2
Where is the Target?

3
PET-CT: Technical Changes New Detector Technology Improved spatial resolution Reduced time for acquisition of PET scans Implication of CT Improved correction for attenuation and scatter Correlation of morphology and metabolism Reduced time of acquisition

4
„Conventional“ Planning in Radiotherapy Diagnostic Tools: CT, PET, MRI… Dedicated Planning CT-scan Definition of Target Volumes => Radiotherapy Plan Simulation Radiotherapy

5
„Modified“ Planning in Radiotherapy Diagnostic Tools: CT, PET/CT, MRI… Dedicated Planning CT scan + 3D-Fusion with PET/CT scan Definition of Target Volumes on Fused Scans => Radiotherapy Plan Simulation Radiotherapy

6
Technical Requirements I Dedicated Radiotherapy Table and Supports @ PET/CT Unit Intrinsic Laser for Patient Positioning @ PET/CT DICOM Data Transfer to Radiation Oncology

7
Image-Fusion-Tool in RT Planning-Software Transfer of Table Position Data to Planning-Software If dedicated 3D RT-Laser @ PET/CT: PET/CT Scan and Dedicated Planning CT as „One-Stop-Shop“ Virtual Simulation on PET/CT Data feasible Technical Requirements II

8
Pitfalls in Target Volume Definition based on PET/CT Nestle et al.; J Nucl Med. 2005 (Aug.)
")
9
Impact of PET/CT on Target Volume Definition Avoidance of ‚Geographic Miss‘ Enlargement of Target Volume Requirement: High Sensitivity and Specificity Protection of non involved Tissue Decrease of Target Volumes Requirement: High Sensitivity

10
PubMed: 1200 Entries for „PET Radiotherapy“ PET/CT: Impact on Target Volume Definition since early 2000‘s Large number of studies but small collectives Up to now no relevant prospective stuedies and long term outcomes Current Evidence

11
A. van Baardwijk et al.; Cancer treatment reviews 2006 Metaanalysis

12
Studies until August 2005 Only one Study (Daines et al. 2004) providing Correlation with Histologic Findings Variable Impact of PET/CT on Target Volume Definition A. van Baardwijk et al.; Cancer treatment reviews 2006 Metaanalysis
 providing Correlation with Histologic Findings Variable Impact of PET/CT on Target Volume Definition A. van Baardwijk et al.; Cancer treatment reviews 2006 Metaanalysis.")
13
Improved Target Volume Definition Avoidance of Organs at Risk (OAR) Potential Dose Escalation in Target Volume PET/CT During Radiotherapy: Therapy Monitoring Predictor for Outcome A. van Baardwijk et al.; Cancer treatment reviews 2006 Metaanalysis

14
Van Baardwijk et al. 2006: 6 Studies 2004-2005 (n=139; 4-40/Study) Comparison of GTV CT and GTV PET/CT 2 Studies: No relevant Difference in Target Volumes 4 Studies: GTV PET/CT < GTV CT Head and Neck Cancer
 Comparison of GTV CT and GTV PET/CT 2 Studies: No relevant Difference in Target Volumes 4 Studies: GTV PET/CT < GTV CT Head and Neck Cancer.")
15
G.P., m, 46y; LN-Metastasis of Hypopharynxcarcinoma Head and Neck Cancer: Example

16
Van Baardwijk et al. 2006: 4 Studies 2000-2005 (n=51; 6-25/Study) Comparison GTV CT and GTV PET/CT 1 Study: No Difference in Target Volume Definition 2 Studies: GTV PET/CT < GTV CT 1 Study: Average Change of Target Volume 26% Messa et al. 2005: Improved Detection and Delineation of Atelectases Lung Cancer
 Comparison GTV CT and GTV PET/CT 1 Study: No Difference in Target Volume Definition 2 Studies: GTV PET/CT < GTV CT 1 Study: Average Change of Target Volume 26% Messa et al. 2005: Improved Detection and Delineation of Atelectases Lung Cancer.")
17
Senan et al. (2005), Crit Rev Oncol Hematol NSCLC: Avoidance of Geographic Miss
, Crit Rev Oncol Hematol NSCLC: Avoidance of Geographic Miss")
18
C. Messa et al.; Q J Nucl Med Mol Imaging 2006 NSCLC: PET/CT During Radiotherapy

19
Moureau et al. IJROBP 2005 Increased Target Volume in Oesophageal Carcinoma

20
Van Baardwijk et al. 2006: 2 Studies (n=41) Lee et al. 2004: In 6/10 Cases Decrease of Target Volume Dizendorf et al. 2003: in 8% additional Lymphnodes, Change of Target Volume in 4% PET/CT in Lymphoma

21
Van Baardwijk et al. 2006: 2 Studies (n=46) Ciernik et al. 2003: In 3/6 (!) Cases Increased Target Volume (Additional Lymph Node Metastases) Lammering et al. 2004: Good Correlation between CT- and PET/CT-based Target Volumes Significant Increase of Target Volume in 6/40 Patients Colorectal Carcinoma
 Cases Increased Target Volume (Additional Lymph Node Metastases) Lammering et al. 2004: Good Correlation between CT- and PET/CT-based Target Volumes Significant Increase of Target Volume in 6/40 Patients Colorectal Carcinoma.")
22
Van Baardwijk et al. 2006: 2 Studies 1998, 2005: Different Tracers (FDG, 11 C-Methionine) GTV PET/CT << GTV MRI Brain Tumours
 GTV PET/CT << GTV MRI Brain Tumours.")
23
Poor Amount of Data for: Breast Cancer and other Gynecologic Tumours Bladder Cancer Prostate Cancer Other Tumours

24
21 consecutive patients 9 male, 12 female Age range 25-68 years Own Experience: Patient Data

25
Own Experience: Tumours I NSCLC:n=6 Lymphoma: n=4 Gastrointestinal Tumours: n=5 Head and neck cancer:n=2

26
Prostate cancer: n=1 Medullary thyroid cancer: n=1 Cancer of Meibom gland:n=1 Cancer of uterine cervix:n=1 Own Experience: Tumours II

27
PET alone:n=9 Integrated PET/CT:n=12 PET-Tracers: 18 F-FDG:n=19 18 F-DOPA:n=1 18 F-Choline:n=1 Own Experience: Devices / Tracers

28
Omission of EBRT: n=3 Extent of presumed volume: n=2 Distant metastases:n=1 EBRT (LINAC):n=18 3D conformal RT:n=11 IMRT:n=6 Stereotactic RT:n=1 Own Experience: Impact of PET on Indication for EBRT
:n=18 3D conformal RT:n=11 IMRT:n=6 Stereotactic RT:n=1 Own Experience: Impact of PET on Indication for EBRT")
29
H.A., f, 68y; NSCLC; Additional Bone Metastases Example: Omission of EBRT

30
Target volume delineation by PET/CT:2/18 Increased target volume:6/18 Decreased target volume:3/18 Unchanged target volume:7/18 Own Experience: Impact on Target Volumes

31
VN.C., f, 34y; Cancer of Cervix Uteri; Additional Retroperitoneal Metastases Example: Increased Target Volume

32
W.L., f, 61y; NSCLC; No Contralateral Involvement Example: Decreased Target Volume

33
Dedicated 3D-RT Lasers @ PET/CT Unit Virtual Simulation 4D-PET/CT: Respiratory Gating Heart Gating Use of SPECT/CT? New Horizons: Nuclear Medicine

34
C. Messa et al.; Q J Nucl Med Mol Imaging 2006 New Horizons: Nuclear Medicine

35
Extended Use of PET/CT in GI-Tumours Soft Tissue Sarcomas New Horizons: Nuclear Medicine

36
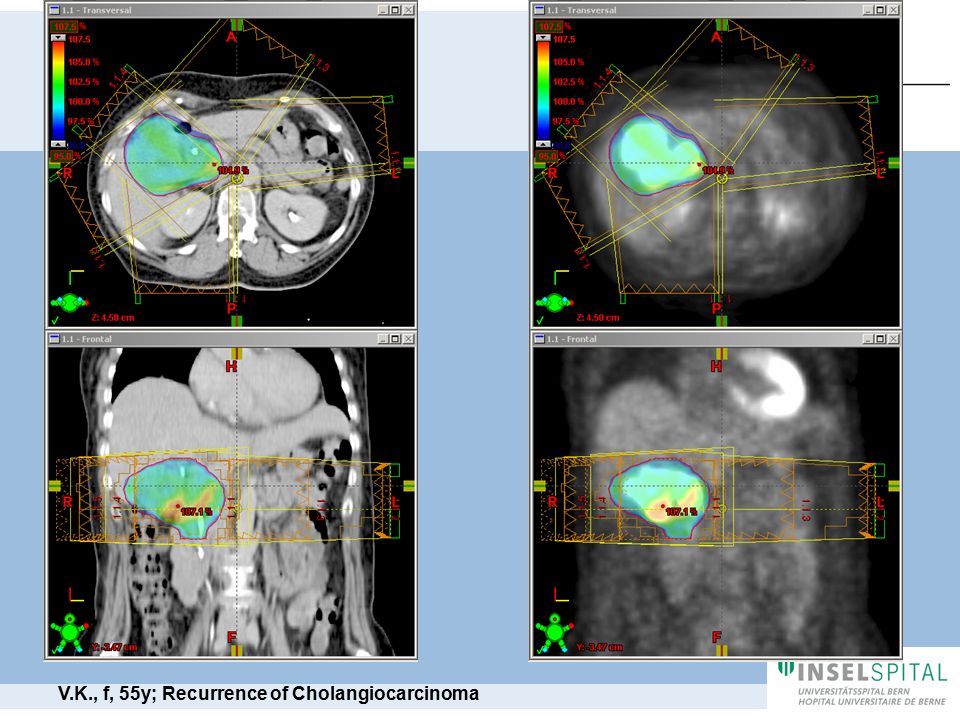
V.K., f, 55y; Recurrence of Cholangiocarcinoma

39
Markers of Hypoxia and Proliferation => „Dose-Painting“ in IMRT Acetate / Choline; Aminoacids: e.g. Brain Tumours Prostate Cancer: 68 Ga-DOTA-BOM Neuroendocrine Tumours: 68 Ga-Peptides New Horizons: Nuclear Medicine

40
G.N., 8y, f; Recidive of anaplastic Oligodendroglioma WHO Grade III Brain Tumours: 18 F-FET-PET/CT

41
S.W., m, 64y; Bone Metastasis of Atlas Prostate Carcinoma: 18 F-Choline PET/CT

42
68 Ga-DOTABOM PET in Prostate Carcinoma Prostata-Ca rechts Prostata-Ca links New Horizons: Nuclear Medicine

43
Virtual Simulation On-Board Imaging Extended Use of IMRT New Horizons: Radiation Oncology

44
On-Board Imaging

45
Tomotherapy? Gamma-Knife? Stereotaxia? Brachytherapy? New Horizons: Radiation Oncology

46
C. Messa et al.; Q J Nucl Med Mol Imaging 2006 New Horizons: Radiation Oncology

47
Need for Provision of Technical Requirements Feasibility Proven Using FDG-PET/CT Currently available Data insufficient Conclusions I

48
Need for Prospective Studies New Horizons in Nuclear Medicine and Radiation Oncology Interdisciplinary Team Work Indispensable Conclusions II

Similar presentations




 is effective, but can be associated with debilitating side.>")







 is well established Tomoharu T. et.>")
: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")






