Download presentation
Presentation is loading. Please wait.

1
Pediatric Board Review Course
The 3rd Annual New York/New Jersey Pediatric Board Review Course General Pediatrics Andrew D. Racine, M.D., Ph.D. May 18, 2008

2
Outline Update on immunizations Breastfeeding Injury Prevention
Anticipatory Guidance Dermatology review Child Abuse

3
Update on Immunizations

4
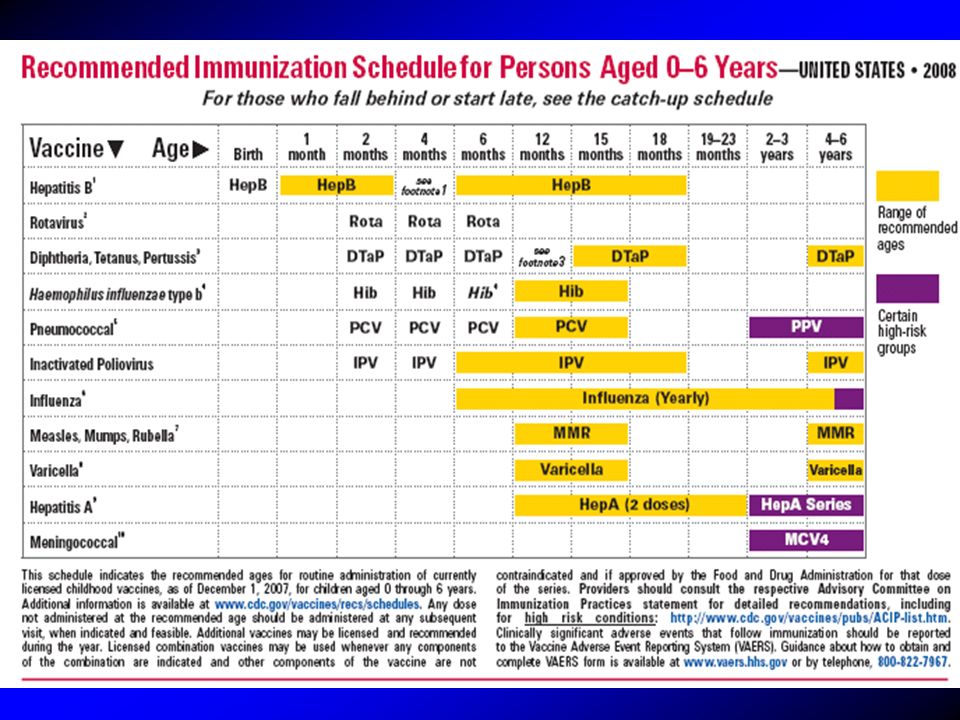
Case #1 Question 1 A 12 year old girl presents to your office for a regular checkup for school entry. She is a recent immigrant from Mexico. Her mother states that she does not have an immunization record. She denies any significant past medical history. There is no history of allergies. Physical exam reveals no abnormalities. Which immunizations would you give at this time?

5
A. Td, IPV, MMR, Varicella, Hep B, MCV4
B. Td, IPV, MMR, Varicella, Hep B, MPSV4 C. Td, IPV, MMR, Varicella, Hep B, Hep A, HPV D. Tdap, IPV, MMR, Varicella, Hep B, MPSV4 E. Tdap, IPV, MMR, Varicella, Hep B, MCV4, Hep A, HPV

8
Pertussis Vaccine (Tdap)
Two new tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines were approved by the FDA in 2005 and are now recommended for: Adolescents aged years who completed their primary series of DTP/DTaP and have not received a Td booster dose Adolescents years who missed the year Td/Tdap booster and completed their primary series Adolescents who have not received DTP/DTaP/Td/Tdap vaccination (or have no documentation) For wound management in adolescents who have not received Tdap before
 For wound management in adolescents who have not received Tdap before.")
9
Meningococcal Vaccine (MCV4)
Another change introduced into the schedule in 2005 is the meningococcal conjugate vaccine which is also recommended in Adolescents years Unvaccinated adolescents at school entry College freshmen living in dormitories Certain high risk groups

10
Hepatitis A Vaccine In May of 2006 the ACIP broadened its recommendations for the use of Hep A vaccine to include all children between 1-2 years of age. The use of Hep A vaccine is also recommended for high risk groups including: Travelers to endemic areas, MSM, drug users, persons with chronic liver disease, those with clotting factor disorders

11
Human Papillomavirus Vaccine
Licensed in June 2006, the ACIP recommends routine immunization of females from 9 years of age up to 26 years of age with a three-dose series where the second and third doses are administered at 2 months and 6 months after the first dose.

13
E. Tdap, IPV, MMR, Varicella, Hep B, MCV4, HEP A, HPV
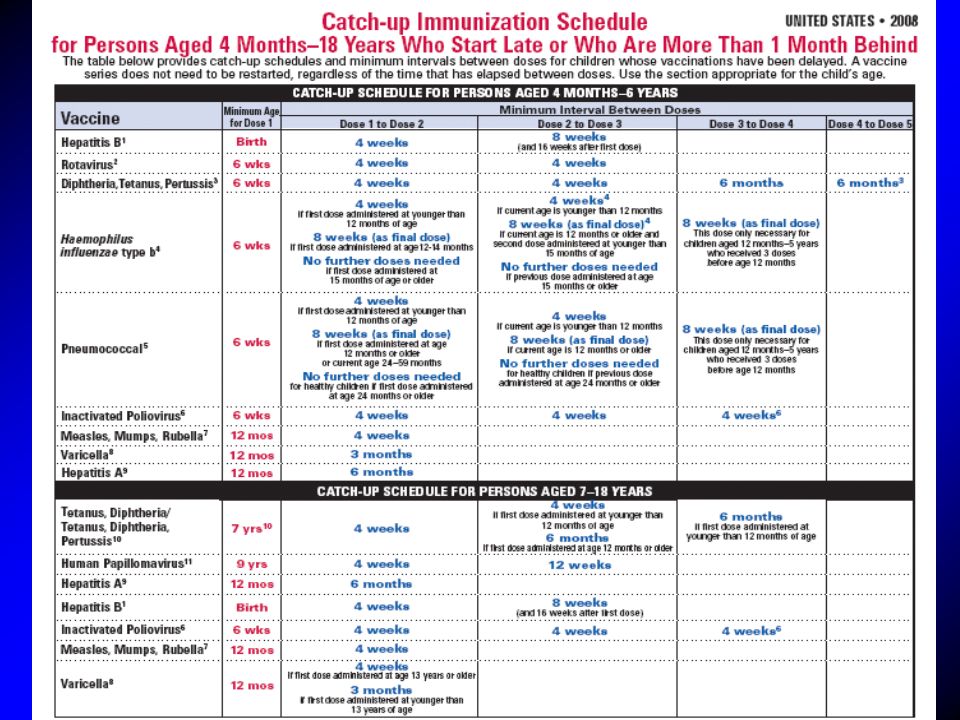
Based on the catch up schedule and the requirements for a patient this age the patient should receive: A. Td, IPV, MMR, Varicella, Hep B, MCV4 B. Td, IPV, MMR, Varicella, Hep B, MPSV4 C. Td, IPV, MMR, Varicella, Hep B, Hep A, HPV D. Tdap, IPV, MMR, Varicella, Hep B, MPSV4 E. Tdap, IPV, MMR, Varicella, Hep B, MCV4, HEP A, HPV

14
Pertussis Pertussis remains endemic despite universal immunization with DTaP. There are 2 peaks of incidence. One is in children under the age of 6 months who are not vaccinated or incompletely vaccinated. The other is in adolescent years whose immunity has waned. The morbidity in adolescents is significant. In 2004, 25,827 cases of pertussis were reported in USA. 34% were in children years.

15
Licensed Tdap Vaccines
BOOSTRIX GlaxoSmithkline Biologicals 10-18 years of age, same t, d, p antigens as INFANRIX but in smaller concentrations ADACEL sanofi pasteur 11-64 years of age, same t, d, p antigens as DAPTACEL but in smaller concentrations

16
Side Effects of Tdap Vaccination
Local Reactions Pain Erythema Swelling Systemic Reactions Headache Fatigue Fever GI events Immediate Reactions including dizziness, syncope and vasovagal reactions were reported with ADACEL

17
Case #1 Question 2 Before you give the Tdap vaccine to the patient you ask your attending what is a true contraindication for the vaccine. Your attending responds that:

18
A. Temperature greater than 105 F within 48 hours of a previous DTP/DTaP
B. Collapse or shock like state within 48 hours of a previous DTP/DTaP C. History of encephalopathy within 7 days of previous DTP/DTaP D. Latex Allergy E. Pregnancy

19
Contraindications of Tdap
Anaphylaxis to any components of the vaccine History of encephalopathy (coma or prolonged seizure) within 7 days of administration of a pertussis vaccine that cannot be attributed to a different cause
 within 7 days of administration of a pertussis vaccine that cannot be attributed to a different cause.")
20
Precautions of Tdap History of an Arthus-type reaction following a previous dose of tetanus- or diphtheria-containing vaccine Progressive neurological disorder, uncontrolled epilepsy, or progressive encephalopathy History of Guillain-Barre syndrome (GBS) within 6 weeks after a previous dose of tetanus toxoid-containing vaccine Moderate or severe acute illness
 within 6 weeks after a previous dose of tetanus toxoid-containing vaccine. Moderate or severe acute illness.")
21
Not Contraindications
Temperature > 105F within 48 hrs of DTP/DTaP Collapse or shock-like state within 48 hrs of DTP/DTaP Persistent crying for 3 hrs or longer within 48 hrs of DTP/DTaP Convulsions with or without fever within 3 days of DTP/DTaP History of entire or extensive limb swelling after DTP/DTaP/Td Stable neurological disorder

22
Not Contraindications
Brachial neuritis Latex allergy other than anaphylaxis-BOOSTRIX single dose and ADACEL are latex free Pregnancy and breastfeeding Immunosuppression Intercurrent minor illness Antibiotic use

23
The only true contraindication of the alternatives listed would be:
Temperature greater than 105 F within 48 hours of a previous DTP/DTaP B. Collapse or shock like state within 48 hours of a previous DTP/DTaP C. History of encephalopathy within 7 days of previous DTP/DTaP D. Latex Allergy E. Pregnancy

24
Meningococcal Disease
American Academy Of Pediatrics. Committee on Infectious Diseases. Prevention and Control of Meningococcal Disease: Recommendations for Use of Meningococcal Vaccines in Pediatric Patients. Pediatrics :116(2):
:")
25
Epidemiology of Meningococcemia
Children < 1 year of age Adolescents years of age College freshmen living in dormitories C5-C9 or C3 deficiency Functional asplenia

26
Licensed Meningococcal Vaccines
MENOIMUNE Meningococcal polysaccharide vaccine MPSV4 Purified capsular polysaccharides A/C/Y/W-135 Licensed in 1981 MENACTRA Meningococcal conjugate vaccine MCV4 Purified capsular polysaccharides A/C/Y/W-135 conjugated to diphtheria toxoid. Licensed in 2005

27
Case #1 Question 3 Your attending asks you what are the advantages of the new meningococcal conjugate vaccine vs. the old polysaccharide vaccine. You answer that all of the following are true except:

28
A. The conjugate vaccine produces an antibody response which lasts longer
B. The conjugate vaccine stimulates a booster response C. The conjugate vaccine promotes herd immunity D. The conjugate vaccine has less side effects E. The conjugate vaccine reduces nasopharyngeal carriage

29
MPSV4 antigens induce a T cell independent antibody response
MPSV4 antigens induce a T cell independent antibody response. As a result there is A short lived response No anamnestic or booster response with subsequent challenge No reduction in nasopharyngeal carriage MCV4 antigens are conjugated to diphtheria toxoid so they induce a T cell dependent response resulting in A long lasting memory Booster response and eradication of nasopharyngeal carriage which contributes to herd immunity. MPSV4 vs. MCV4

30
Advantages of MCV include all of the following except:
A. The conjugate vaccine produces an antibody response which lasts longer B. The conjugate vaccine stimulates a booster response C. The conjugate vaccine promotes herd immunity D. The conjugate vaccine has less side effects E. The conjugate vaccine reduces nasopharyngeal carriage

31
MCV4 Side effects include: Erythema, swelling and induration
Guillain-Barre – 17 reported cases from March 2005 – September GBS incidence estimated at 0.20 per 100,000 person months after vaccine compared to 0.11 per 100,000 person months among year olds generally.

32
Human Papillomavirus The most common sexually transmitted infection in the United States (6.2 million new cases annually). HPVs are non-enveloped double stranded DNA viruses of over 100 types including several (16,18,31,33,35, and others) detected in 99% of cervical cancer cases. Risk of HPV associated with number of sexual partners, partner sexual behavior, and immune status.
 detected in 99% of cervical cancer cases. Risk of HPV associated with number of sexual partners, partner sexual behavior, and immune status.")
33
Human Papillomavirus Most infections are transient, asymptomatic and clear within 1-2 years Of the 6.2 million new cases per year, about 74% occur in women 15-24 Acquisition occurs soon after sexual debut Prevalence of HPV 16 may be as high as 40% Consistent condom use may help prevent acquisition

34
HPV Vaccine Quadravalent HPV vaccine (Gardasil®) targets HPV types 6, 11, 16 and 18 HPV types 16 and 18 cause approximately 70% of cervical cancers and types 6 and 11 cause approximately 90% of genital warts Administered in 3 doses with second and third doses given 2 and 6 months after the first dose Combined protocols indicate an efficacy of % in the prevention of CIN 2/3, AIS or genital warts caused by HPV 6, 11, 16 and 18.

35
Case #1 Question 4 You explain to your attending your intention to administer the Gardasil® vaccine and he responds, “Are you nuts? That vaccine costs a gazillion dollars!! What are you a Merck shareholder or something?” You calmly reply that:

36
The vaccine only costs $50 per dose
The treatment of genital warts and cervical cancer costs more than $8 billion a year in the U.S. Depending upon how long you assume immunity lasts and what percent of girls get the vaccine, immunizing all 12 year old girls will cost only $3,000 to $25,000 per QALY. Vaccinating will save the future costs of having to screen for cervical cancer in these patients

37
HPV Costs and Benefits Management of warts and cervical cancer costs about $4 billion per year in the U.S. Vaccine for Children’s program (VFC) will cover costs of Gardasil for eligible patients Several cost/benefit analyses estimate the cost of a QALY to be between $3,000 and $25,000 depending upon underlying assumptions Factors to consider: duration of vaccine protection, duration of natural immunity, frequency of cancer screening, vaccine coverage
 will cover costs of Gardasil for eligible patients. Several cost/benefit analyses estimate the cost of a QALY to be between $3,000 and $25,000 depending upon underlying assumptions. Factors to consider: duration of vaccine protection, duration of natural immunity, frequency of cancer screening, vaccine coverage.")
38
The vaccine only costs $50 per dose
The treatment of genital warts and cervical cancer costs more than $8 billion a year in the U.S. Depending upon how long you assume immunity lasts and what percent of girls get the vaccine, immunizing all 12 year old girls will cost only $3,000 to $25,000 per QALY. Vaccinating will save the future costs of having to screen for cervical cancer in these patients

39
Case #1 Question 5 You ask your 12 year old patient to return in 4 weeks to continue the catch up schedule of vaccination you started. At that visit you will administer:

40
A. Td,IPV,MMR,Hep B B. Td,IPV,MMR,Varicella,Hep B C. Tdap,IPV,MMR,Hep B,MCV4 D. Tdap,IPV,MMR,Varicella,Hep B E. Tdap,IPV,MMR,Varicella,Hep B,MCV4

41
Catch-up Schedule Tdap is licensed for only one dose. According to the AAP, the patient in this case should receive 3 tetanus/diphtheria toxoid vaccines and only one of them should also contain pertussis, preferably the first dose. Varicella- Two doses are now recommended. A 2nd dose is given in 4 weeks for those over 13 and in 3 months for those less than 13. MCV4 only one dose is required.

42
Return Visit should include:
A. Td,IPV,MMR,Hep B B. Td,IPV,MMR,Varicella,Hep B C. Tdap,IPV,MMR,Hep B,MCV4 D. Tdap,IPV,MMR,Varicella,Hep B E. Tdap,IPV,MMR,Varicella,Hep B,MCV4

43
Hepatitis A Vaqta and Havrix are both licensed for children 1 year of age and older and they are now recommended as part of the routine immunization schedule to be given to all children at the age of 1 year. Children who are not vaccinated by 2 years should be vaccinated at subsequent visits. 2 doses are recommended 6 months apart.

44
Influenza Influenza vaccine risk factors now include children with compromised respiratory function or handling of respiratory secretions and also children that have an increased risk of aspiration. In July 2007, ACIP issued a recommendation expanding routine influenza vaccination to children 6 – 59 months and their household contacts. Previously unvaccinated children should receive 2 doses this vaccine.

45
Rotavirus Rotavirus is the leading cause of severe gastroenteritis worldwide resulting in more than 500,000 deaths/year. In the USA it is a major disease burden with 3.2 million episodes of diarrhea, 60,000 hospitalizations and deaths /year. Additional problems include Shedding of the virus before sxs develop and up to 21 days after onset of the disease Children developing insufficient immunity after one infection and therefore experiencing it more than once Major cause of day-care center acquired gastroenteritis

46
Rotavirus vaccines All rotavirus vaccines are oral, live attenuated, containing glycoprotein (VP7) and protease-cleaved proteins (VP4) of Group A rotavirus, the most prevalent type found in humans. ROTASHIELD –licensed in 1998, tetravalent rhesus-human reassortment, withdrawn from the market due to cases of intussusception. ROTATEQ – FDA approved in 2006, pentavalent bovine-human reassortment, no intussusception reported in large trial of 70,000 doses. ROTARIX – licensed in 30 countries but not in USA yet, divalent human vaccine, also well tolerated.
 and protease-cleaved proteins (VP4) of Group A rotavirus, the most prevalent type found in humans. ROTASHIELD –licensed in 1998, tetravalent rhesus-human reassortment, withdrawn from the market due to cases of intussusception. ROTATEQ – FDA approved in 2006, pentavalent bovine-human reassortment, no intussusception reported in large trial of 70,000 doses. ROTARIX – licensed in 30 countries but not in USA yet, divalent human vaccine, also well tolerated.")
47
Breastfeeding

48
Case # 1 A female infant presents for her two week check-up. She was born after a 38 week uncomplicated pregnancy via spontaneous vaginal delivery at a birth weight of 3 kg. Her mother is breastfeeding and asks whether breast milk alone is sufficient for her baby. What advice should you give her?

49
True or False? The baby should receive oral iron supplements for the first 6 months of life. The baby does not need vitamin K after birth so long as the mother is taking oral Vitamin K. Starting before 2 months of age the baby will need 200 IU of vitamin D daily while she is exclusively breastfed.

50
Question # 1 False

51
Iron Iron stores at birth are proportional to birth weight or size.
Iron stores for term infants are sufficient to meet needs for the first 4-6 months of life. Breast milk contains <0.1 mg/100cc of iron but it is in a highly bio-available form (50% of it is absorbed compared to 4% of iron in iron-fortified formulas). Infants’ adequate intake of iron is approximately 0.27 mg/day for the first 4-6 months of life.
. Infants’ adequate intake of iron is approximately 0.27 mg/day for the first 4-6 months of life.")
52
Question # 2 False

53
Vitamin K Vitamin K is a fat soluble vitamin necessary for the posttranslational carboxylation of glutamic acid residues of coagulation proteins Factors II, VII, IX and X. lpi.oregonstate.edu/infocenter/vitamins/vitamink/kcycle.html

54
Vitamin K Breast milk has inadequate amounts of vitamin K to satisfy infant requirements. All breastfed infants should receive mg of vitamin K IM after the first feeding and within the first 6 hrs of life. Oral vitamin K may not provide the stores necessary to prevent hemorrhage in later infancy and is not recommended at this time.

55
Question # 3 True

56
Vitamin D Vitamin D (calciferol) is available from certain dietary sources and can be synthesized in skin upon exposure to UV light. Adequate intake of vitamin D for infants is 200 IU per day. Vitamin D content of human milk is low (22 IU/L).
.")
57
Vitamin D Breastfed infants should receive supplements of 200 IU of vitamin D per day so long as the daily consumption of vitamin D-fortified formula or milk is below 500 ml. The recommended routine use of sunscreen in infancy decreases vitamin D production in skin.

58
More on Breastfeeding Compared to the weight gain of formula fed infants in the first year of life, the weight gain of breast fed infants: Is less rapid during the first 3-4 months but then catches up Is more rapid during the first 3-4 months but then slows down Generally results in a slightly heavier infant by 12 months of age Does not differ at all

59
More on Breastfeeding Compared to the weight gain of formula fed infants in the first year of life, the weight gain of breast fed infants: Is less rapid during the first 3-4 months but then catches up Is more rapid during the first 3-4 months but then slows down Generally results in a slightly heavier infant by 12 months of age Does not differ at all

60
More on Breastfeeding Breast fed infants tend to gain more weight than do formula fed infants in the first 3-4 months of life. It is acceptable for their weight gain to cross one or two percentiles downward in the period after 4 months so long as they maintain their length and head circumference.

61
More on Breastfeeding By the end of the first year of life, breast fed infants who had solids introduced at 4-6 months of age tend to be slightly leaner than formula fed infants. Term infants require between 100 to 120 kcal/kg per day in order to grow.

62
Injury Prevention

63
Injury Prevention A 6 month old boy is at your office with his father for a routine health care maintenance visit. In discussing injury prevention for his infant, the father wants to know what he should be most concerned about with respect to his infant’s safety. What should you tell him?

64
Leading Causes of Death by Age Group - 2001
< 1 yr 1-4 yrs 5-9 yrs 10-14 yrs 1 Congenital Anomalies 5,513 Unintentional Injury 1,714 1,283 1,553 2 Short Gestation 4,410 557 Malignant Neoplasms 493 515 3 SIDS 2,234 420 Congenital anomalies 182 Suicide 272

65
Leading Causes of Injury Deaths by Age Group 2001

66
Deaths Due to Injury in Childhood
SIDS is the leading preventable cause of death in children less than 1 year of age. Unintentional injury is the leading cause of death in children from 1 to 15 years of age. Motor vehicle incidents, drowning and deaths from burns taken together account for over 75% of all deaths from injury in children between 1 and 15 years of age.

67
Motor Vehicle Injury Prevention
When counseling a parent with respect to infant car seats, all of the following are true except: Children should face the rear of the vehicle until they are at least 1 year of age or weigh at least 20 lbs. Convertible safety seats positioned upright and facing forward should be used for children beyond 1 year and 20 lbs until they reach 40 lbs. A rear facing car safety seat must not be placed in the front passenger seat of any vehicle with an air bag on the front passenger side.

68
Motor Vehicle Injury Prevention
Answer A: Children must weigh 20 lbs and be at least 1 year of age before sitting in a forward facing car seat. Many infants reach 20 lbs before their first birthday but should not be turned to face forward before that time.

69
Motor Vehicle Injury Prevention
Convertible seats are the safest for children after they reach 1 year and 20 lbs until they are 40 lbs and can use booster seats. Convertible Car Seat (Up to 40 lbs) Booster Car Seat (More than lbs)
 Booster. Car Seat. (More than lbs)")
70
Motor Vehicle Injury Prevention
No rear facing seats should be placed in the front passenger seat of a car equipped with air bags; and any child less than 13 should preferentially sit in the rear seat to avoid injury from inflating air bags.

71
Drowning Injury The father of that 6 month old infant also has a 4 year old boy at home. When counseling him about the epidemiology of childhood drowning, a TRUE statement is:

72
Drowning is the leading cause of death due to injury
For every one drowning victim there are 5 near drownings Pool alarms have eliminated the need for fencing Residential pools are the most common drowning sites The ratio of male-to-female drowning deaths is 1:1

73
Drowning Injury Residential pools are the most common site of drowning for children younger than 5. Infants drown in bathtubs most often and adolescents in fresh water lakes and rivers. Drowning is the 2nd leading cause of death in this age group (remember earlier) with peak incidence in the summer months and highest rates in the west and the south.
 with peak incidence in the summer months and highest rates in the west and the south.")
74
Drowning Injury Four sided fences 5 ft high with self-closing self-locking gates are the most effective enclosures for residential pools. Pool alarms, pool covers, swimming lessons for young children and floatation devices are not as effective as proper enclosures in preventing drowning deaths. Male to female ratio is 3:1 and 50% of submersion victims are declared dead at the site (drowning to near drowning ratio of 1:1).
.")
75
Drowning is the leading cause of death due to injury
For every one drowning victim there are 5 near drownings Pool alarms have eliminated the need for fencing Residential pools are the most common drowning sites The ratio of male-to-female drowning deaths is 1:1

76
Injury Prevention: Burns
You are approaching the end of a health care maintenance visit for a 2 year old girl. The mother explains that the family recently moved into a private house having lived previously in an apartment. What four concrete pieces of advice can you give her about how she might make her new home safe from the standpoint of preventing burn injuries to her toddler?

77
Injury Prevention: Burns
Don’t smoke in the home. Home fires cause three fourths of all fire deaths and children below the age of 5 are at highest risk. Adults who smoke carelessly or who fall asleep while smoking are responsible for the largest percentage of home fires that kill or injure children.

78
Injury Prevention: Burns
Install smoke detectors on each floor in the house and test them every 6 months. Smoke detectors provide the best protection should a home fire begin since: a) most fires start in the early morning hours; b) most fires burn for a long time before discovery; and c) deaths are usually due to CO poisoning so early alerts can help prevent injury and death.
 most fires start in the early morning hours; b) most fires burn for a long time before discovery; and c) deaths are usually due to CO poisoning so early alerts can help prevent injury and death.")
79
Injury Prevention: Burns
Prepare emergency escape plans for use in the event of a fire. Even children as young as 3 can be taught how to safely get out of the house in the event of a fire. If fire extinguishers are available in the home (and they should be) children should always be taught to leave the house rather than try to put out a fire themselves.
 children should always be taught to leave the house rather than try to put out a fire themselves.")
80
Injury Prevention: Burns
Set hot water heaters at no higher than 120o F. Tap water at 160o F can produce a full-thickness scald burn in less than 1 second. At 120o F the scalding time is increased to between 2 and 10 minutes.

81
Anticipatory Guidance Potpourri
A six month old breast fed male infant is at your office for a well child check-up. He has been previously well and on exam babbles, reaches for your stethoscope and pulls to a sitting position without head lag. He can also: Finger feed himself Imitate sounds Pull to stand Transfer objects from one hand to the other Use a scissors grasp to obtain a piece of cereal

82
Anticipatory Guidance Potpourri
Correct answer is 4, transfer objects. As part of his normal development this infant probably began to hold a rattle briefly at 2 months, reached for objects and and lifted himself onto extended elbows at 4 months. He probably also began to roll over at 4 months and could roll both ways by 6 months. He likely began to coo at 2 months, to laugh out loud at 4 months, and to begin to babble at 6 months. Pulling to stand usually begins around 8 months. Finger feeding and imitating sounds usually starts at 9 months.

83
Anticipatory Guidance Potpourri
You are seeing a set of parents with their 8 year old boy for a health care maintenance visit. The mother asks you whether allowing her son to watch TV when he comes home from school is a bad idea. The MOST accurate statement you can make to her about the influence of television viewing on children is:

84
TV Viewing Most adolescents have difficulty discriminating between what they see on TV and what is real. Nearly 2/3 of all programming includes violence and children’s programming contains the most violence. 50% of 2-7 year olds have a TV in their room. A majority of parents report that they always watch TV with their children to monitor the content of what is seen.

85
TV Viewing Although young children and adolescents are vulnerable to the messages conveyed on television, it is predominantly younger children who cannot discriminate between what is real and what they see on TV. In a random survey of parents with children from kindergarten through 6th grade published in 1996, 37% reported that their child had been frightened or upset by a TV program seen during the preceding year. Cantor J, Nathanson AI. Children’s fright reactions to television news. J Commun. 1996;46:

86
TV Viewing About one third of parents of 2-7 year olds report that their children have a television in their room. Less than half of all parents state that they always watch television with their children to monitor the content of what is being seen.

87
TV Viewing A recently completed 3 year National Television Violence Study reported that: Nearly 2/3 of all programming contains violence; That children’s shows contain the most violence; That portrayals of violence are usually glamorized; and Perpetrators often go unpunished. Federman J. ed. National Television Violence Study Vol 3. Thousand Oaks, CA: Sage; 1998.

88
TV Viewing Most adolescents have difficulty discriminating between what they see on TV and what is real Nearly 2/3 of all programming includes violence and children’s programming contains the most violence 50% of 2-7 year olds have a TV in their room A majority of parents report that they always watch TV with their children to monitor the content of what is seen

89
Dermatology

90
Case # 1 A 2 month old boy experiences the onset of a salmon-colored confluent scaly rash on his cheeks, neck, groin and axillae. The mother points out an erythematous patch behind the right ear. There is no history of fever or other systemic symptoms. The patient seems otherwise well and is not uncomfortable with the rash. There is no involvement of his nails.

91
dermatlas.com/derm/

92
The rash is consistent with
A. Atopic Dermatitis B. Candidal Dermatitis C. Seborrheic Dermatitis D. Contact Dermatitis E. Psoriasis

93
C. Seborrheic Dermatitis
Etiology – unknown Epidemiology – seen during infancy and in adolescence Clinical – symmetric distribution in areas of high concentration of sebaceous glands (face, scalp and intertriginous areas such as neck, axilla, groin, post auricular). Salmon colored and scaly. Non pruritic. Treatment – Skin – topical steroids Scalp – oil/comb or antiseborrheic shampoo Complications – Secondary infection Post inflammatory pigmentary changes
. Salmon colored and scaly. Non pruritic. Treatment – Skin – topical steroids. Scalp – oil/comb or antiseborrheic shampoo. Complications – Secondary infection. Post inflammatory pigmentary changes.")
94
dermatlas.med.jhmi.edu

95
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

96
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

97
Atopic Dermatitis Etiology – Unknown. Interplay of genetics and environment. Associated with atopy. More than 50% develop asthma/allergic rhinitis. Epidemiology – 10-15% of children, with rapidly increasing prevalence. Pathogenesis – Keratinocytes induce T cells to produce decreased g interferon (a T2 inhibitor) thus contributing to eosinophilia and IgE. Clinical – Vicious cycle which begins with predisposition to dry skin – pruritis - scratching - more dryness and erythematous weeping crusted rash with indistinct border.
 thus contributing to eosinophilia and IgE. Clinical – Vicious cycle which begins with predisposition to dry skin – pruritis - scratching - more dryness and erythematous weeping crusted rash with indistinct border.")
98
Distribution varies with age:
Infantile - Starts on cheeks and spreads to neck/wrists/hands/abdomen/extensor surfaces. Diaper area often spared. Childhood – Extensor lesions now become flexural. Greater tendency for chronicity. Adolescent – Also includes dorsal hands, feet and between fingers and toes. May also involve eyelids, infra auricular fold and vulva. Lichenification – thickened, hyperpigmented skin Atopic pleats – extra groove on lower eyelid Pallor around nose, mouth and ears

99
Treatment – “Break vicious cycle” lubrication, humidifiers, mild soaps, soft cotton clothing, anti pruritics. Food elimination – May be considered in children under 2 yrs. since it is associated in 40% of cases. Topical Steroids – Start with low potency. Immune modulators –The FDA after reviewing their safety has issued a warning that the use of calcineurin inhibitors may be associated with an increased risk of cancer. For refractory mod to severe cases. Tar, phototherapy and systemic treatment with glucocorticoids, cyclosporine and interferon reserved for severe cases. Complications – Secondary infection due to altered cell immunity (MRSA, eczema herpeticum).
.")
100
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

101
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

102
Psoriasis Etiology – Unknown. Associated with certain HLA types. Multifactorial inheritance. Epidemiology – Incidence 1-3%. Onset before age 20 in 37% of cases. In childhood F:M ratio 2:1. Adults 1:1. Clinical – Round, erythematous, well marginated patches covered by a grayish or silvery white scale. Individual small lesions coalesce to form patches. Distribution – scalp, extensor surfaces, lumbosacral, anogenital regions. Sometimes flexural.

103
Special Features Auspitz sign – removal of scale results in fine punctate bleeding points. Koebner phenomenon – skin lesions that occur at the site of local injury Guttate psoriasis – round or oval lesions appear suddenly over a large part of the body after a URI, with strep or withdrawal of steroids. Pityriasis amianteca – psoriasis on the scalp - firmly adherent crusts somewhat resistant to tx. Nail involvement – Pitting, discoloration, subungal hyperkeratosis, onycholysis.

104
Pathogenesis – Marked increase in epidermal cell turnover.
Treatment – Lubrication, avoid scratching. Steroids – use least potent topical that’s effective Vit D Analogs – calcipotriene stings, takes long to work Topical Retinoids – syst tox in large quantity Tar +/- UV light or PUVA (UV + psoralens) Systemic methotrexate, oral retinoids, cyclosporine. Complications – Psoriatic arthritis. No relationship between severity of cutaneous disease and the development of joint disease.
 Systemic methotrexate, oral retinoids, cyclosporine. Complications – Psoriatic arthritis. No relationship between severity of cutaneous disease and the development of joint disease.")
105
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

106
Contact Dermatitis – non allergic
Irritant Contact Dermatitis – results from direct contact with caustic agents which include soaps, bleaches, detergents, solvents, bubble baths, saliva, urine, feces, etc. resulting in changes in the skin which follow the distribution of the contact. Classical example is diaper dermatitis – Fecal enzymes are activated by alkaline urea in the urine. Rash is erythematous, scaly, well demarcated and distributed along the convex surfaces of the perineum, sparing intertriginous areas. Treatment includes frequent diaper changes, gentle cleaning and barrier pastes.

107
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

108
Contact Dermatitis - allergic
Etiology – Type IV delayed type hypersensitivity reaction. Agents include poison ivy, oak and sumac, nickel, rubber, glue, dye, neomycin, topical anesthetics and antihistamines, cosmetics. Clinical – Erythema, intense pruritis, vesiculation, crusting and scaling with distribution following the pattern of sensitization. Initial reaction – 8-12 hours following exposure. Subsequent reaction – 7 – 10 days following exposure. Treatment – avoidance, washing skin immediately after contact, steroids topical and oral, antihistamines.

109
Case #2 The following painful lesion developed in a 5 year old boy who was playing in his back yard where there were a lot of mosquitoes.

111
The lesion is A. Impetigo B. Folliculitis C. Furuncle D. Ecthyma
E. Erysipelas

112
D. Ecthyma Etiology – beta hemolytic strep, occasionally staph and pseudomonas. Epidemiology – Poor hygiene, malnutrition, trauma, insect bites and other pruritic lesions. Clinical – Vesicle with erythematous base and crusting erodes into the skin forming an ulcer with elevated margins. Lesions are painful, slow growing and chronic. Commonly found in the lower extremities and the buttocks. Treatment – warm compresses, removal of crusts, systemic antibiotics

113
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

114
Impetigo Etiology – beta hemolytic strep and staph
Epidemiology – any age but more common in the young, in exposed areas (non bullous), in traumatized areas of skin (bullous) Clinical – Non bullous – erythematous macules -> thin roofed vesicles surrounded by a red base –> rupture and release yellow fluid –> drying with formation of honey colored crust. Bullous – superficial blisters that rupture and leave an erythematous, denuded base. Autoinoculation contributes to spread.
, in traumatized areas of skin (bullous) Clinical – Non bullous – erythematous macules -> thin roofed vesicles surrounded by a red base –> rupture and release yellow fluid –> drying with formation of honey colored crust. Bullous – superficial blisters that rupture and leave an erythematous, denuded base. Autoinoculation contributes to spread.")
115
Treatment – With localized lesions topical mupirocin. With disseminated lesions systemic treatment with diclox, augmentin, cephalexin, clindamycin. Complications – Beta strep infections can result in acute glomerulonephritis and scarlet fever. In addition, both organisms can contribute to the development of osteomyelitis, arthritis, pneumonia, sepsis, cellulitis, lymphangitis.

116
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

117
Folliculitis Superficial or deep infection of hair follicles
Etiology – S. aureus. Occasionally strep, proteus, pseudomonas. Epidemiology – Induced by agents that obstruct pilosebacious glands such as oils, tars, occlusive dressings. Atopic dermatitis and seborrhea predispose as well as poor hygiene and excess sweating. Shaving can cause sycosis barbae, a deeper form of folliculitis. Hot tub dermatitis occurs in areas covered by the bathing suit and is caused by pseudomonas 8-12 hrs after exposure. Clinical – yellow pustule surrounded by red areola surrounding a hair shaft. Distributed anywhere on the body where there is hair. Treatment – avoid offending agent, gentle cleansing, topical antibiotics.

118
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

119
Furuncle Develops from preceding folliculitis which extended more deeply into the skin or from trauma. Etiology – Staph aureus Group I and II. Clinical – red, tender, well circumscribed nodule which enlarges and then becomes boggy and fluctuant. If untreated it will suppurate and release purulent discharge. Healing results in scar formation. Treatment – systemic antibiotics and incision and drainage. Complications – carbuncles which are aggregates of interconnected furuncles that drain at multiple points on the cutaneous surface. They present with systemic symptoms such as fever, malaise and prostration. Seen more commonly with obesity, diabetes and immunosuppression.

120
dermatlas.med.jhmi.edu forlag.fadl.dk

121
Erysipelas Cellulitis with marked lymphatic vessel involvement due to Group A beta hemolytic streptococci. Epidemiology – direct inoculation or hematogenous spread. Clinical – Abrupt onset of systemic symptoms followed by an area of erythema which enlarges to reveal a tense, hot, painful, shiny, brawny infiltrated plaque with a distinct and well marginated border. Most commonly on the face and the scalp but can be anywhere. Treatment – Penicillin. If allergic then erythromycin or clindamycin. With penicillin resistance nafcillin, oxacillin, augmentin, cephalothin, cefazolin Complications – Patients my become bacteremic, especially infants.

122
Case #3 A 12 year old female patient is diagnosed with UTI. Two days after starting treatment with bactrim she experiences the acute onset of the following rash:

123
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

124
The rash is most likely to be
A. Fixed Drug Eruption B. PLEVA C. Exanthematous Drug Eruption D. Urticaria E. Erythema Multiforme

125
E. Erythema Multiforme Mucocutaneous hypersensitivity syndrome
Etiology – Viruses (most commonly herpes simplex), bacteria (including mycoplasma), protozoa, fungi, TB, foods, immunizations, sunlight, malignancy, radiotherapy, IBD, Polyarteritis Nodosa, Sarcoidosis, Graft vs. Host disease. Many drugs can cause EM including sulfa, penicillin, tetracycline, anticonvulsants, allopurinol, barbiturates, salicylates, NSAIDs, isoniazid, captopril, etoposide.
, bacteria (including mycoplasma), protozoa, fungi, TB, foods, immunizations, sunlight, malignancy, radiotherapy, IBD, Polyarteritis Nodosa, Sarcoidosis, Graft vs. Host disease. Many drugs can cause EM including sulfa, penicillin, tetracycline, anticonvulsants, allopurinol, barbiturates, salicylates, NSAIDs, isoniazid, captopril, etoposide.")
126
Clinical – Acute onset of a fixed, symmetrical eruption consisting of erythematous macules, papules, vesicles or bullae with predilection for palms, soles, dorsi of hands and feet, extensor surface of arms and legs. May extend later to trunk, face and neck. The hallmark lesion of EM is the target – an erythematous plaque with central clearing and a dusky center. If an enanthem is present it involves oral lesions only. Treatment – Supportive.

127
Stevens – Johnson Severe form of EM. Characterized by an abrupt prodrome, same eruption as EM and involvement of at least 2 mucous membranes. Treatment is supportive and morbidity and mortality are significant. dermatlas.med.jhmi.edu

129
Pityriasis Lichenoides et Varioliformis Acuta
Also known as Mucha Habermann’s Disease Thought to result from immune dysregulation prompted by exposure to viral, bacterial or other environmental antigen Recurrent crops of red papules 2-4 mm with central crustingb (looks like chickenpox) May treat with oral erythromycin for 1 –2 months
 May treat with oral erythromycin for 1 –2 months.")
130
Zitelli. Atlas of Pediatric Diagnosis. 2nd Edition

131
Urticaria Experienced by 20%, but most of the time the etiology is unknown. Allergic causes Antibiotics –Penicillins/Cephalosporins/Sulfa Urticaria can occur during or soon after course. Bee stings Seasonal and contact allergens Food – Infants – eggs/milk –may outgrow. Older children – peanuts/sesame/shellfish/fish --- do not outgrow.

132
Non-allergic Causes Cholinergic – heat, exertion, sweating & stress induce acetylcholine which in turn induces histamine release and urticaria. Starts in adolescence. Aquagenic – contact with water or perspiration. Solar – with minimal exposure to sunlight. Cold – inherited (mild), acquired (severe) Viral – EBM, Hep C, Herpes, Coxsackie Pressure – tight clothes. Onset 4-6 hrs after pressure. Vibratory – working with drills or jackhammers. Papular – at the site of insect bites. Histamine induced –product induces histamine release in non allergic patient (IVP dye, azo dye)
, acquired (severe) Viral – EBM, Hep C, Herpes, Coxsackie. Pressure – tight clothes. Onset 4-6 hrs after pressure. Vibratory – working with drills or jackhammers. Papular – at the site of insect bites. Histamine induced –product induces histamine release in non allergic patient (IVP dye, azo dye)")
133
Characteristic rash is composed of erythematous wheals that are highly variable, rapidly changing and transient with individual lesions lasting less than hours. Intensely pruritic. It may be associated with angioedema. Acute <6 weeks, causes can often be found. Chronic > 6 weeks, commonly unknown etiology. May be an important sign of systemic disease including malignancy, CV, autoimmune disease. Treatment – avoidance, antihistamines (H1 +H2 may work better than H1), steroids, cyproheptadine (cold), leukotriene inhibitors (together with H1).
, steroids, cyproheptadine (cold), leukotriene inhibitors (together with H1).")
134
Vanderhooft. Contemporary Pediatrics. 1998. Vol 15(5):118-137
:")
135
Exanthematous Drug Eruption
This is the most common drug reaction and is responsible for 50% of all drug reactions. It consists of erythematous macules and papules which begin on the trunk, then spread to the face and extremities and may include palms and soles. It is pruritic and not associated with fever. It resembles a viral exanthem and must be carefully distinguished.

136
Child Abuse

137
Case #4 The parents of a 9 month old baby girl who is new to your practice bring her for a regular checkup. There are no complaints. Physical exam reveals the following lesion:

138
dermatlas.com/derm/

139
The following risks factors may indicate child abuse except:
A. Patient is less than 3 years of age B. There is a history of spousal abuse C. Father is an alcoholic D. Mother did not breastfeed the child E. The child is a foster child

140
D. Mother did not breastfeed the child
Risk factors for Child Abuse – Parental Past history of abuse or family violence Inability to cope, lack of support, attachment issues Closely spaced pregnancies, financial problems Alcoholism, addiction, psychosis, depression Young parental age, single parent Risk factors for Child Abuse – Child Child is less than 3 years of age Twin, prematurity Chronic illness, mental retardation, learning disability Foster or adopted child

141
Child abuse – Physical signs
Bruises, burns, bites, blunt-instrument marks Fractures – bucket handle, posterior rib fractures, multiple fractures at different stages of healing Intracranial hemorrhages Retinal hemorrhages Duodenal hematomas, lacerations of liver and spleen, mesenteric tears Oral lacerations Failure to thrive

142
Multiple posterior rib fractures
Bucket handle fracture aafp.org/afp/ /3057_f7.jpg

Similar presentations













 SC.912.L.14.52 Explain the basic functions of the human immune system, including specific and nonspecific immune response, vaccines,>")





 Primary infection results in varicella (chickenpox) Recurrent infection results in herpes zoster (shingles) Short.>")


