Download presentation
Presentation is loading. Please wait.

1
Decision Analysis

2
Real Case 63 year old housewife with 6 grown children. 10 year history of stable angina pectoris. 8 years ago she had total hip replacement. Had post operative pulmonary embolism but recovered and was pain free and fully mobile 1 year later.

3
For the last 12 months she had experienced increasing pain in her hip on weight bearing. Is now mostly confined to a wheelchair. 8 months ago she had an uncomplicated non- Q wave anterior wall MI. Her stable angina limits her ability to get about on crutches. Orthopedic surgeon reviewed the case and concluded she most likely had loosening of the femoral component. He spelled out the risks and benefits of reoperation:

4
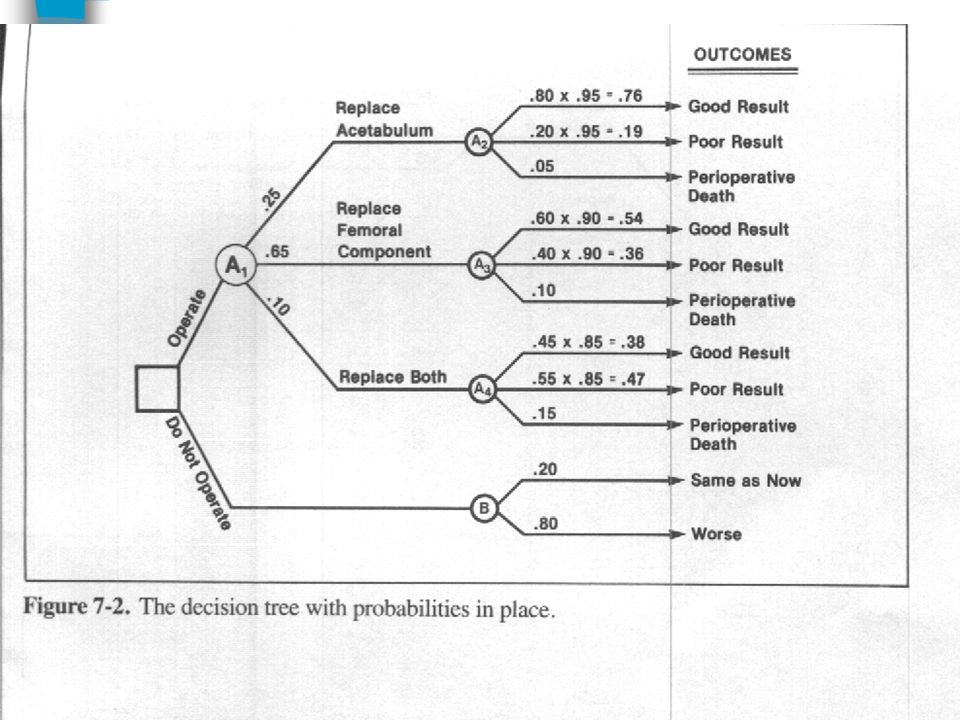
If only the femoral component needed replacement: Chances of that are 65%. The probability of a good result would be 60%. (Probability of poor result 40%). Operative mortality is 10%.
. Operative mortality is 10%..")
5
If only the acetabular component needed replacement: Chances of that are 25%. The probability of a good result would be 80%. (Probability of poor result 20%). Operative mortality is 5%.
. Operative mortality is 5%..")
6
If both components needed replacement: Chances of that are 10%. The probability of a good result would be 45%. (Probability of poor result 55%). Operative mortality is 15%.
. Operative mortality is 15%..")
7
If no surgery: She would remain the same (chances of that 20%). Or she would get worse and become permanently confined to her wheelchair (80%).
..")
8
Debate ensued within the care team Some advocated surgery. Others recommended against it. Moreover, although they wanted to involve the patient, they feared they would sway her by the fashion in which they presented the facts to her.

9
The debate was occurring Despite agreement about the risks and benefits. This suggested that a decision analysis may provide: 1. An objective resolution. 2. Would allow the team to involve the patient without unfairly swaying her decision.

10
Step 1 Create a decision tree A map of all the courses of action and all their consequences. Boxes are decision nodes. Circles are chance nodes. Ovals are end nodes.

12
Step 2 Assign probabilities To all the branches all the way to end.

14
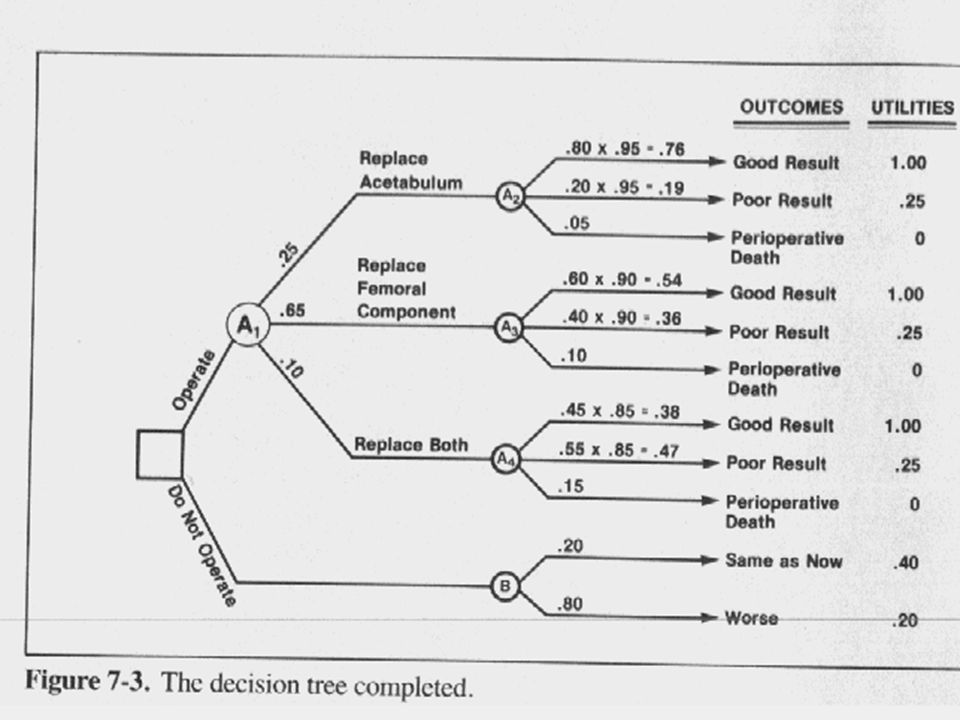
Step 3 Assign utilities To all the potential outcomes (the end nodes) First rank the outcomes from best to worst. Assign numerical values to them. This is where it gets tough, not because it’s artificial (for we always assign utilities when dealing with patients) but because it forces us to be explicit.
 but because it forces us to be explicit..")
15
Standard reference gamble To assign utility to an intermediate outcome we offer a gamble between the two extremes versus the guaranteed intermediate.

16
Utilities Ranking: 1. Good result 1.0 2. Same as now 0.4 3. Poor result 0.25 4. Worse 0.2 5. Death 0

18
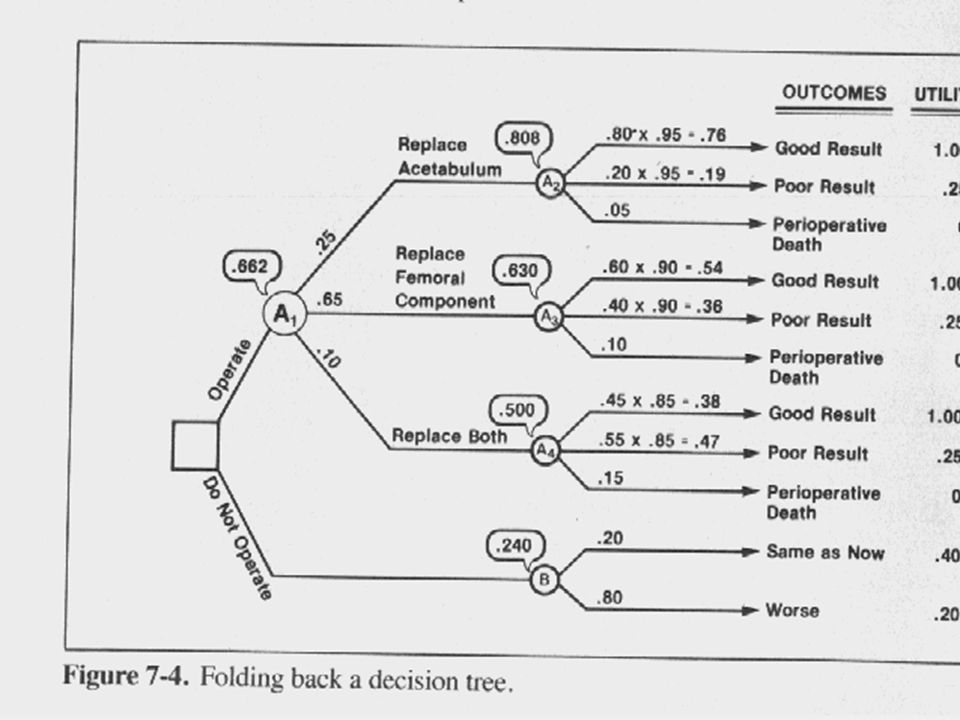
Step 4 Fold back Multiply utilities by probabilities. The utility of a chance node is the weighted sum of it’s branches. The utility of a decision node (if there are any intermediate ones) is that of the highest branch.
 is that of the highest branch..")
20
The Verdict Operate 0.66 (0.81, 0.63, 0.50). Do not operate 0.24.
. Do not operate 0.24.")
21
Step 5 Pick the decision That has the highest utility.

22
Step 6 Sensitivity analysis Test the decision for its vulnerability to clinically sensible changes in probabilities and utilities.

23
Sensitivity analysis After the patient pondered with family she revised utilities upward for current status and future without surgery. That did not reverse the preference for surgery. Some team members objected to some utilities. All adjustments made the decision to operate stronger.

24
Introduction Aortic stenosis often requires the replacement of the aortic valve with a prosthesis(AVR). Both short-term survival and long-term survival are influenced by the presence or absence of CAD, which may be asymptomatic. The prevalence of occult CAD in women in this age and race is 0.067.

25
CABG Coronary artery bypass graft (CABG), performed at the same time as the AVR improves the survival, both long-term and short term, of patients with CAD requiring AVR. Of course, CABG is an operative procedure that increases both the peri-operative mortality and the cost for a patient without CAD, and accordingly, one wishes to avoid it in a patient with NO CAD.

26
Cath Catheterization is the "gold standard" for the diagnosis of CAD. However, it too has a mortality associated with it, (.001 in a cohort of unselected patient; but.002 in patients with aortic stenosis) and should be avoided if this can be done without increasing the estimated expected risk to the patient.
 and should be avoided if this can be done without increasing the estimated expected risk to the patient..")
27
DTH In an attempt to improve the overall management strategy, a technique known as dipyridamole thallium imaging has been devised. This technique involves the administration of dipyridamole thallium, accompanied by hand-grip exercise (DTH test). Images of the heart are obtained, and the degree of perfusion is observed. This procedure is essentially free of mortality or serious side-effects.
. Images of the heart are obtained, and the degree of perfusion is observed. This procedure is essentially free of mortality or serious side-effects..")
28
DTH In populations with coronary artery disease, 85 out of 100 patients will have a positive test (sensitivity =.85). In patients without coronary artery disease, 14 out of 100 patients will have a positive test (specificity =.86).
..")
29
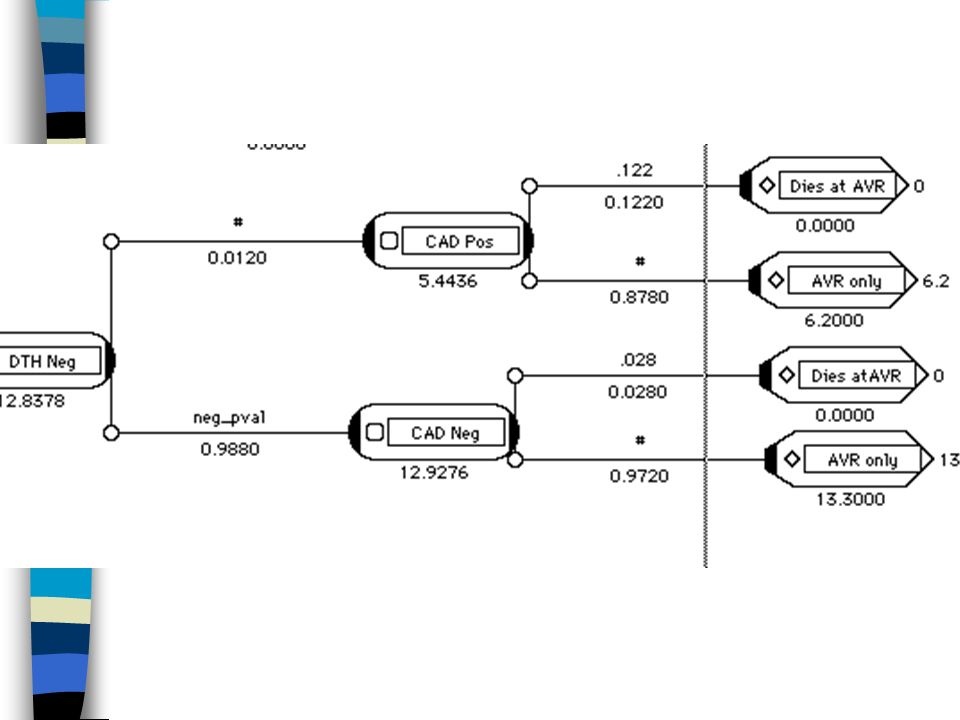
Operative Mortality for AVR replacement Patients with CAD receiving CABG............... 0.061 Patients with CAD not receiving CABG......... 0.122 Patients without CAD...................................... 0.028

30
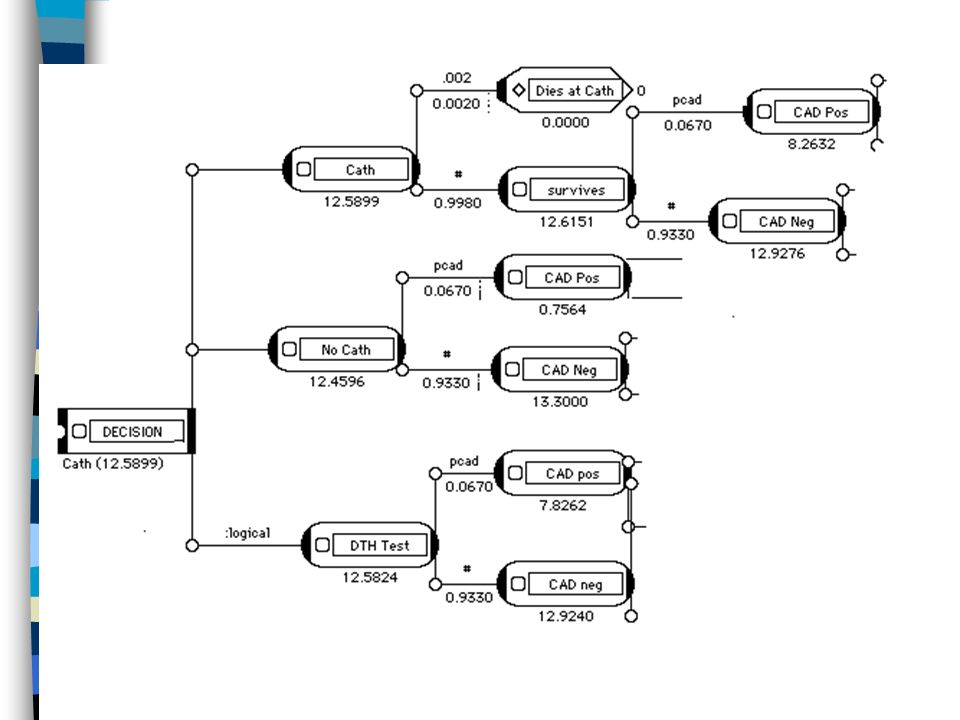
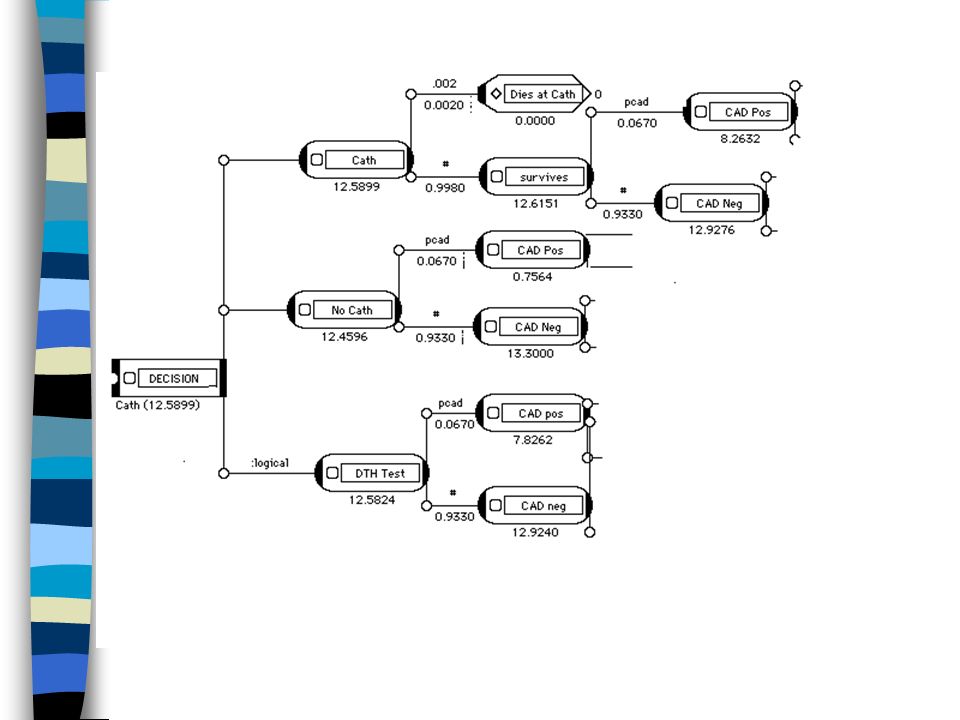
The Case A 63 year old white woman with symptomatic AS requires an aortic valve replacement. She has no angina or evident signs of CAD. Potential Management Strategies. 1. Perform AVR in the AS patient, with no CABG. No catheterization is performed in this strategy.

31
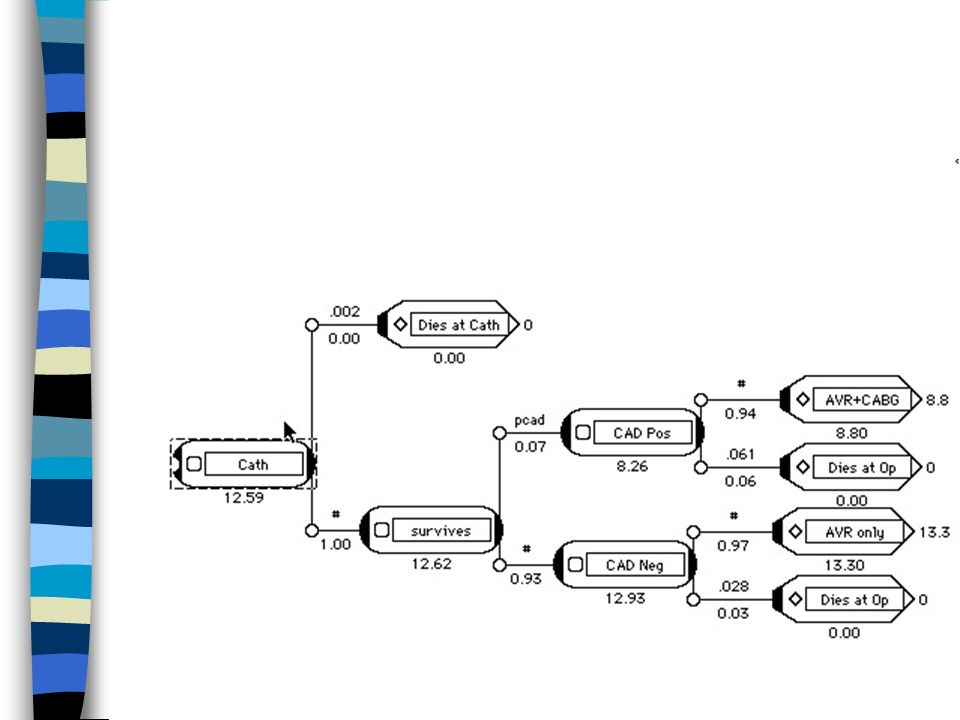
2. Catheterize this patient and if CAD is shown, perform a CABG and AVR. Several consequences: Those patients whose occult coronary artery disease is detected will receive the benefit of longer long-term survival by virtue of CABG. All patients in this group are also subject to the additional risk of the catheterization itself.

32
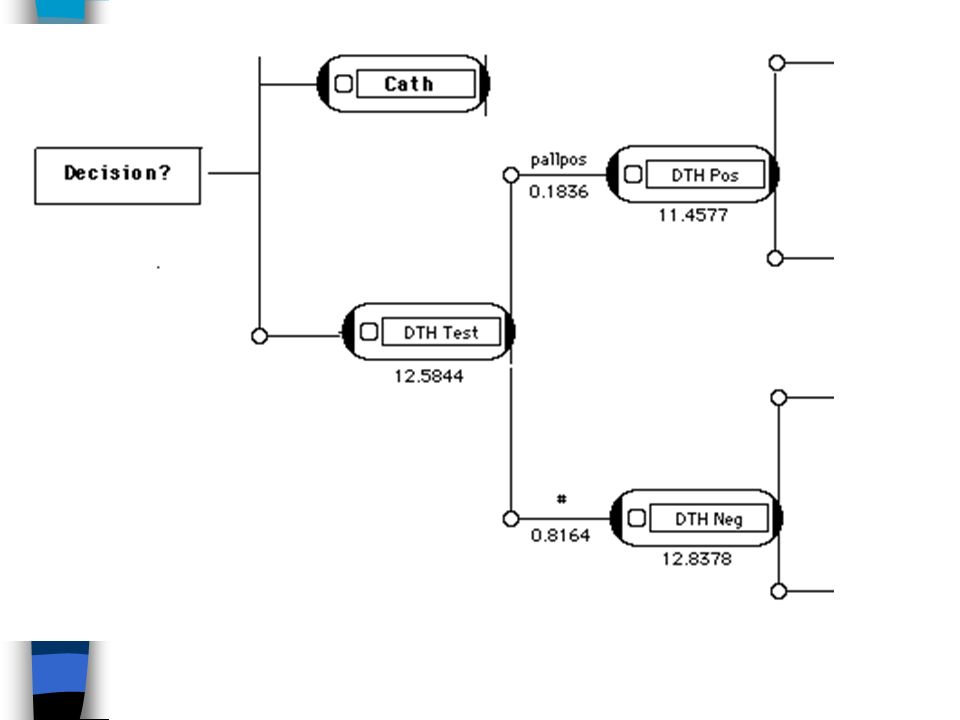
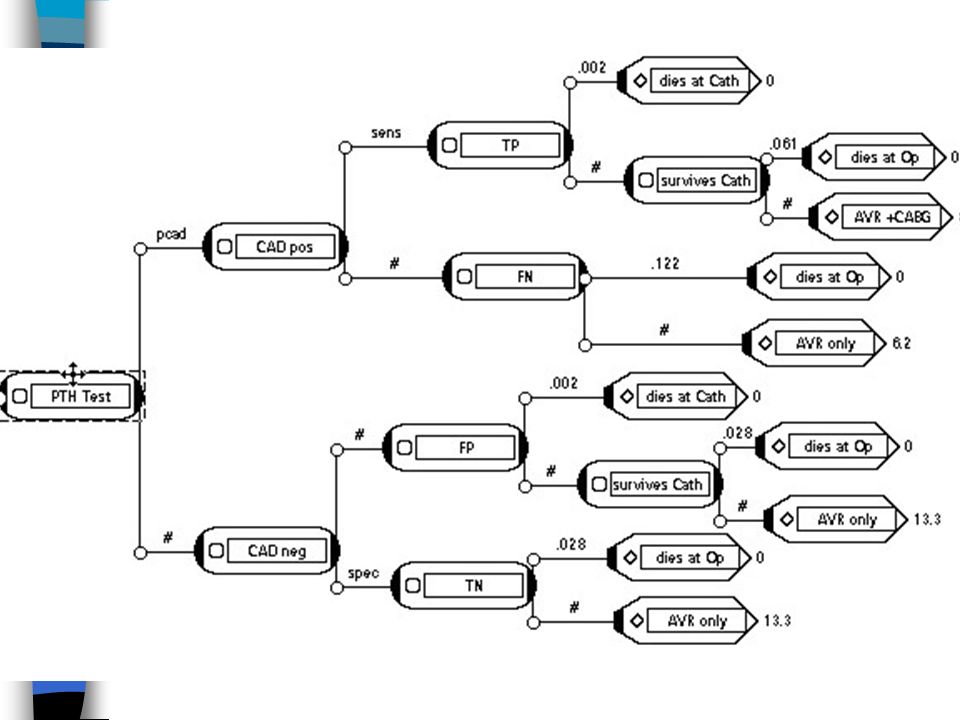
3. Carry out the dipyridamole thallium handgrip test (DTH). If DTH positive perform catheterization, and if that shows CAD, then perform CABG and AVR. If catheterization negative, only perform AVR. If DTH negative, only perform AVR.

33
Utilities No coronary artery disease (CAD).....13.3 years Coronary artery disease present - No CABG performed.....6.17 years Coronary artery disease present - Simultaneous CABG.....8.8 years
 years Coronary artery disease present - No CABG performed years Coronary artery disease present - Simultaneous CABG years")
34
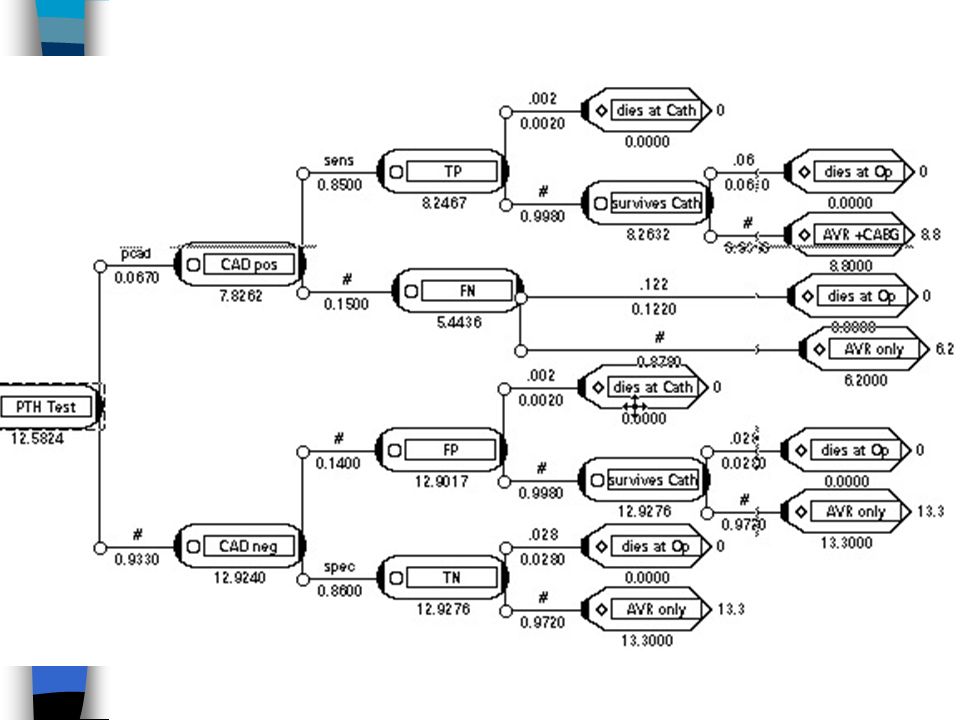
The assignment is: 1. Make a decision tree, incorporating the 3 strategies named above and the associated probabilities of each outcome.Label each node, associated probabilities and utilities. 2. Fold back the tree(s)showing the folded back values at each node.
showing the folded back values at each node..")
35
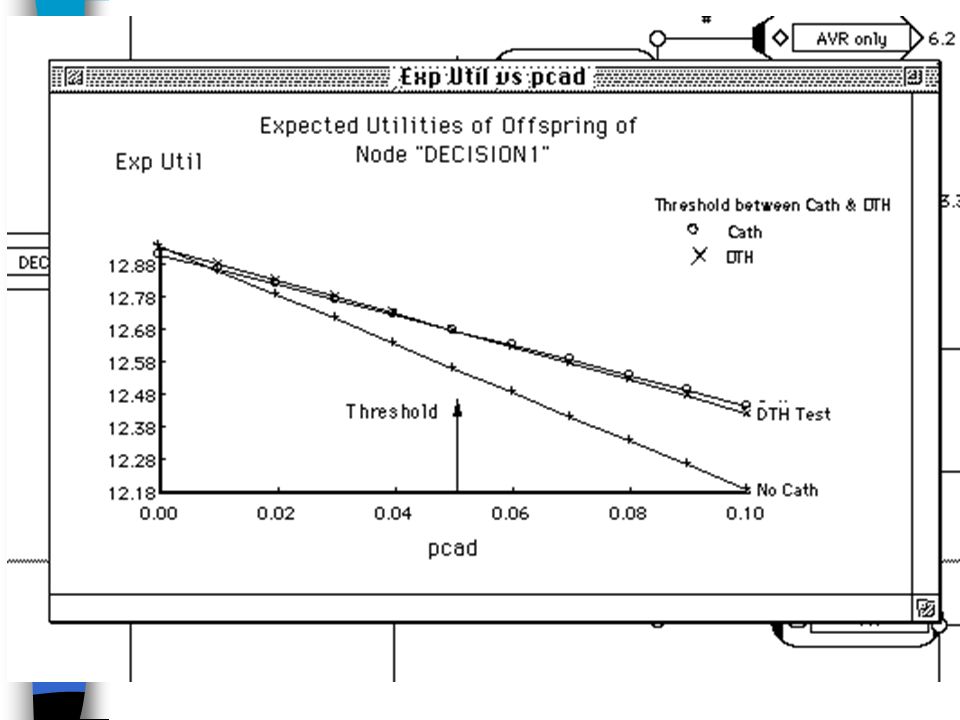
Assignment cont. What is the preferred management strategy, based solely on expected longest length of survival as the utility. What is the estimated number of person- months of additional life that the preferred strategy provides over the second best strategy? For the preferred strategy, carry out a sensitivity analysis with respect to the prevalence of CAD versus the expected survival. sensitivity analysis

45
At any prevalence of CAD below.050, it would be preferable to do a DTH test, and catheterize or not based on the results of that test. At prevalences above that threshold, catheterization of all candidates for AVR is preferred

Similar presentations



 Coronary artery bypass.>")













 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")




