Download presentation
Presentation is loading. Please wait.

1
1 Covenants of the Medical Home Neighborhood How Primary Care Physicians and Specialists can “Choose Wisely”

2
2

3
Pre-Operative Evaluations Issue was identified by the ACO as an area for cost savings and improvement. Dr. Gray and Dr. Trimble heading up ACO project. Dr. Maxwell and Dr. Phoenix were asked to participate as primary care representatives. Pathway of a pre-operative consult starts with surgeon and often goes through PCP. As PCP’s we have control over how much testing is done, and how much money is spent.

4
Pre-Operative Evaluations Multiple areas for cost savings but one of the high dollar items is nuclear stress testing. Estimated that 90% of MPS exams are normal, indicating that too many tests are being ordered, or are being ordered inappropriately. ACC/AHA guidelines have been simplified and most often do not recommend pre-operative stress testing.

5
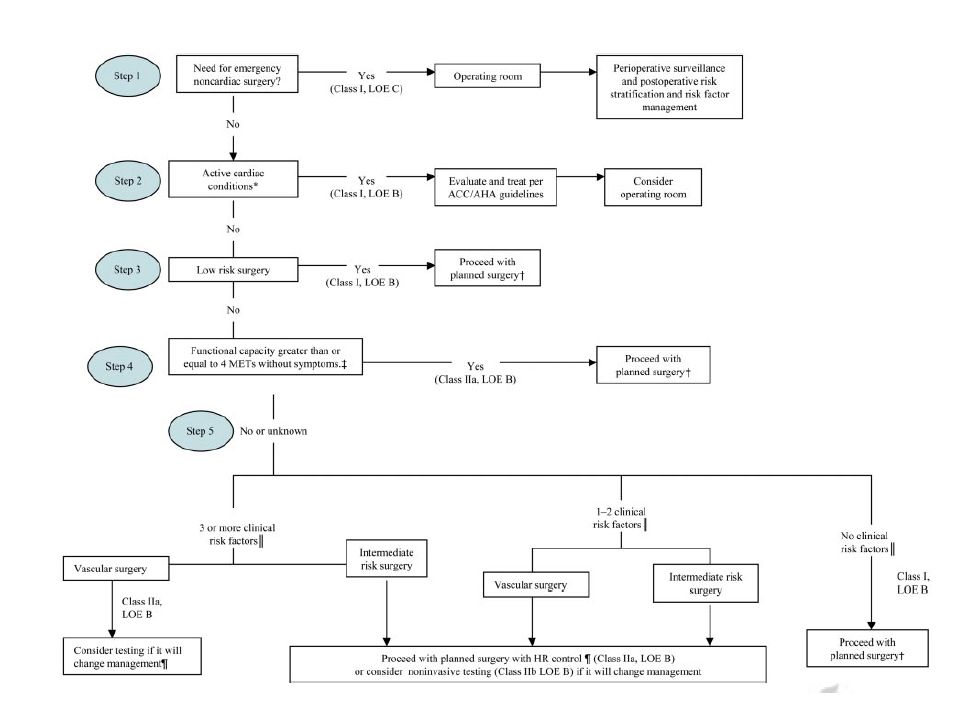
For Patients Needing Elective Surgery Surgery Non-cardiac Surgery Nonvascular surgery: If the patient can do the following without cardiac symptoms – Proceed to surgery without stress testing Walk up a hill Run a short distance Do light work around the house Climb a flight of stairs If the patient has cardiac symptoms, refer for cardiac consultation

6
Summary of the CARP Study Patients scheduled for high risk Vascular surgery Patients were high risk patients Patients had ≥ 70% stenosis at preop Heart Cath No difference in post operative MI or Death with preoperative stenting or CABG versus proceeding to surgery with Beta blockers without preoperative revascularization.

8
Pre-Operative Evaluations Cardiology has already come up with some auto-texts to ease documentation. Subjective The patient is scheduled to undergo surgery with Dr. _____ Can the patient exercise > 4 METS ( Walk up a hill, run a short distance, do light house work, climb a flight of stairs) without ischemic symptoms? Does the patient have a cardiac condition to address prior to surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, or severe aortic / mitral valve stenosis?
 without ischemic symptoms. Does the patient have a cardiac condition to address prior to surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, or severe aortic / mitral valve stenosis .")
9
Pre-Operative Evaluations Cardiology has already come up with some auto-texts to ease documentation. Assessment for patients who are able to exercise 4 METS: The patient is planning to have a surgery that is not defined as high risk surgery (such as aortic surgery, major vascular surgery, peripheral vascular surgery ). There are no active cardiac contraindications for surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, or severe aortic or mitral stenosis. They are able to exert themselves greater than 4 METS (walk up a hill, run a short distance, do light housework) without ischemic symptoms. Therefore, the ACC guidelines recommend proceeding to surgery without further testing.
. There are no active cardiac contraindications for surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, or severe aortic or mitral stenosis. They are able to exert themselves greater than 4 METS (walk up a hill, run a short distance, do light housework) without ischemic symptoms. Therefore, the ACC guidelines recommend proceeding to surgery without further testing..")
10
Pre-Operative Evaluations Cardiology has already come up with some auto- texts to ease documentation. Assessment for patients who are not able to exercise 4 METS. The patient is planning to have a surgery that is not defined as high risk surgery (such as aortic surgery, major vascular surgery, peripheral vascular surgery ). There are no active cardiac contraindications for surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, severe aortic or mitral stenosis. The patient is not having ischemic cardiac symptoms, however they don’t routinely exercise > 4 METS. If the patient has one or more clinical risk factors ( ischemic heart disease, compensated or prior heart failure, diabetes mellitus, renal insufficiency, and cerebrovascular disease ), I would recommend perioperative beta blockers to lower their ischemic risk.
. There are no active cardiac contraindications for surgery including unstable coronary syndrome, decompensated heart failure, uncontrolled arrhythmia, severe aortic or mitral stenosis. The patient is not having ischemic cardiac symptoms, however they don’t routinely exercise > 4 METS. If the patient has one or more clinical risk factors ( ischemic heart disease, compensated or prior heart failure, diabetes mellitus, renal insufficiency, and cerebrovascular disease ), I would recommend perioperative beta blockers to lower their ischemic risk..")
11
Proposal SJC Primary Care Physicians agree to participate in more formalized plan for pre-operative testing. When issue is clear-cut the above verbiage can be used to justify less pre-operative testing. For more complex cases the cardiology service will work on a “fast-track” pre-operative consult visit. Cardiology consultation is less expensive than ordering a stress test, and cardiologists are more comfortable with medical management and avoiding tests.

12
Proposal - Benefits We see these patients anyway, this is not a plan to send more of these patients to us. Systematic easy evidence to fall back on for decision making. Pre-defined documentation. Better patient care, less testing. Triple aim, etc. Possible overlap with CPCI Milestone 6 Consider care agreement with cardiology rather than GI?

Similar presentations














>")






