Download presentation
Presentation is loading. Please wait.

3
Khaled Halima Lecturer of chest diseases Al- Azhar University

4
Personal history: ► Male patient. ► 53 years old. ► Born, living in Eldarrasa. ► Married for 20 year. ► Electrical engineering. ► Heavy Smoker.

5
I 2 Months II 1.5 Months III 1Month VI 2 Weeks 1/11/2009 …. 31/3/2010 Stages

6
Stage 1

7
► Pain in both heels. 1/11/2009----1/1/2010 ► Swelling of both lower limbs up to both knees. ► Bluish discoloration of skin.

8
Treated with : 1) Brufen 400mg 1x2 2) Augmentin 625mg 1x3
 Brufen 400mg 1x2 2) Augmentin 625mg 1x3")
10
Referral to vascular physician

11
1) Colchicine tab 1x3 2) Marevan 5mg tab 1x1 3) Aspocid 75mg 2x1 4) Anti-cox cap 1x2 5) Thrombophob cream 1x2 Received the following medications :
 Colchicine tab 1x3 2) Marevan 5mg tab 1x1 3) Aspocid 75mg 2x1 4) Anti-cox cap 1x2 5) Thrombophob cream 1x2 Received the following medications :")
12
New symptoms: -Migrating pain and bluish discoloration of the skin appeared in both upper limbs. -Increased bluish discoloration of skin up to the thighs.

13
What are the possibilities? 1- Cellulitis ? 2- Vasculitis? 3- Local cause? TraumaV.V. I.V. Inject. 4- Burger’s Disease?

14
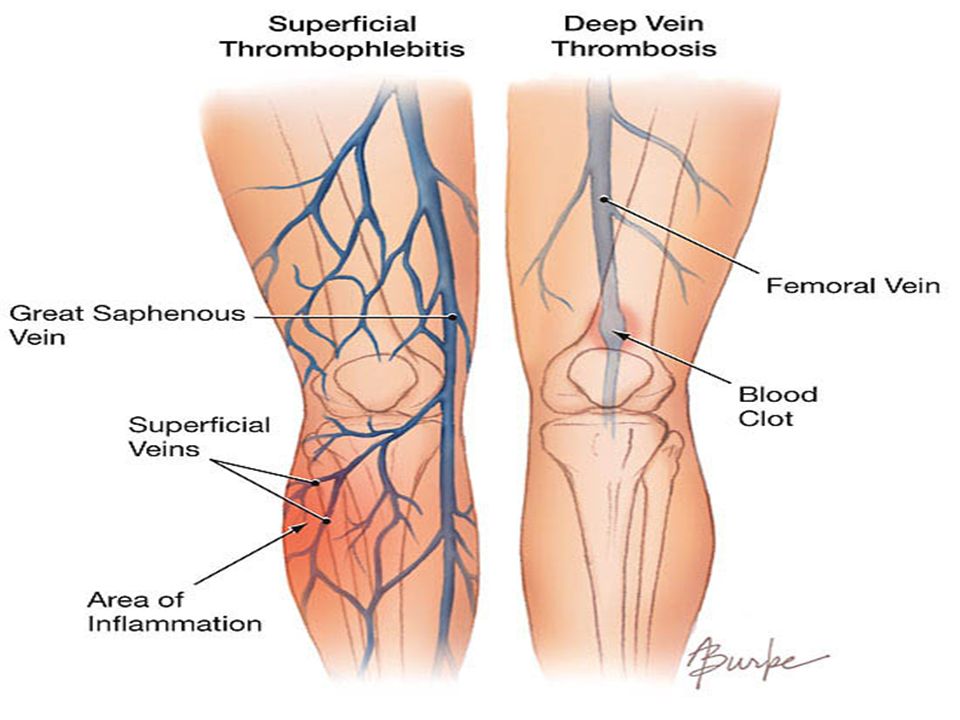
What investigations do you suggest? 1-X-ray for both feet 2-Duplex for both LL. 3-ESR. Normal Superficial thrombophlibitis in GSV ( Great Saphenous Veins ) in both limbs more in left side with no evidence of DVT. 125 4. ANA, ANCA, AntiDS DNA Negative
 in both limbs more in left side with no evidence of DVT ANA, ANCA, AntiDS DNA Negative.")
15
7-Renal function test. 6-Liver function test. 5-Complete blood count. HB 13.4 PLT 507 TLC 14.7

19
I Superficial Thrombophlibitis 2 Months

20
Partial improvement

21
Stage II

22
Pleuritic chest pain in left side. 1/1/2010-------20/2/2010 Haemoptysis.

23
Referral to chest physician

24
What Investigations do you suggest? ■ Coagulation profile.

25
Coagulation profile

26
Complete blood count

27
Liver, Renal function test

28
■ Chest X Ray P.A View 21/1/20104/2/2010

29
Pulmonary embolism involving the left lower lobar pulmonary artery & its anterior & lateral segmental branches with consequent left lower lobar pulmonary consolidation (likely an infarction & left sided mild pleural effusion). CT Pulmonary Angiography

30
CT Pulmonary Angiography 10/2/2010

31
- Pulmonary emboli at the posterior & medial segmental branches of the right lower lobar pulmonary artery.

33
DDecision: Pulmonary Embolism.

34
I Superficial Thrombophlibitis 2 Months II Pulmonary Embolism 1.5 Months

35
Stage III

36
Fever. Productive Cough. Dyspnea of gradual onset, progressive course, increased with mild exertion. 20/2/2010----18/3/2010

37
20/2/2010

38
Developed: Marked Dyspnea. Fever Subsided.

39
7/3/2010 8/3/2010 Before Aspiration After Aspiration

40
Simple aspiration was done >> Haemorrahgic in nature.

42
Marked loss of weight. Haemoptysis. Dyspnea at rest. Chest pain, severe back pain that decreased with potent analgesics. New Symptoms

43
Decision???

44
2- X-ray: Massive left sided pleural effusion. investigated by : 1- (INR: 9) So oral anti-coagulant was stopped.
 So oral anti-coagulant was stopped..")
45
15/3/2010

46
So thoracocentesis was done 4400 ml was aspirated by multiple sessions

47
3-Marevan toxicity? What the cause of pleural effusion?? 1-Pulmonary embolism? 2-Pneumonia? 5- Non of the above? 4-Trauma ?

48
I Superficial Thrombophlibitis 2 Months II Pulmonary Embolism 1.5 Months III Pleural Effusion 1Month

49
Reevaluation

50
Stage IV

51
progression of the previous symptoms 18/3/2010 …… 31/3/2010

52
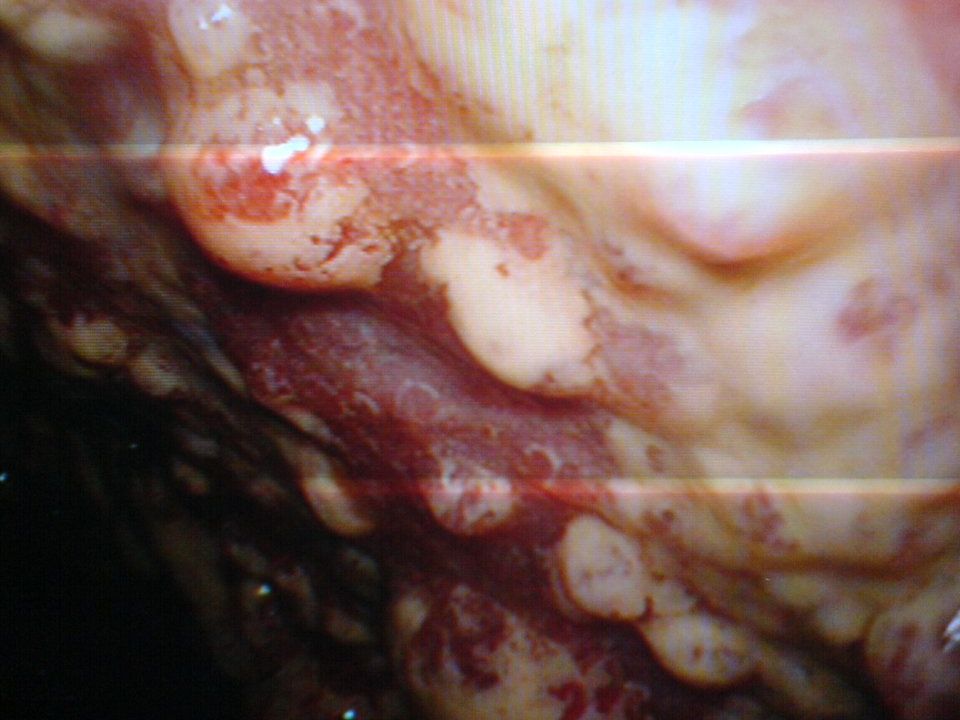
Thoracoscope was done

53
(multiple pleural nodule was seen & taken as biopsies) & another 1500 ml. of haemorrahgic effusion was aspirated). Result
. Result.")
56
18/3/2010

57
Marked loss of weight. Loss of appetite, cachexia. Marked dyspnea, orthopnea, cyanosis. Psychological depression. Generalized bone ache. New symptoms

58
Malignant infiltrating adenocarcinoma versus epithelial mesothilioma for immunophenotyping.

59
Immunophenotyping reaveled that it is adenocarcinoma.

60
Immunophenotyping reaveled that it is adenocarcinoma

61
I Superficial Thrombophlibitis 2 Months II Pulmonary Embolism 1.5 Months III Pleural Effusion 1Month VI Adenocarcinoma 2 Weeks

62
How???

63
Superficial Thrombophlibitis Pulmonary Embolism Massive Pleural effusion Adenocarcinoma

64
CAUSES OF SUREFICIAL THROMBOPHELEBITIS HEMATOLOGIC SYNDROMES: Most hematologic syndromes associated with lung tumors are not as well characterized as the endocrine syndromes, because the ectopic hormone responsible for the syndrome has not been identified in most tumor tissues.

65
In many of the hematologic syndromes, such as granulocytosis and thrombocytosis, clinical sequelae are often absent. As with the endocrine paraneoplastic syndromes, the most appropriate therapy for the hematologic syndromes is the treatment of the underlying neoplasm.

66
Granulocytosis Non – small-cell lung cancer is the most common cancer associated with granulocytosis. Twenty percent of patients with non – small-cell lung cancer have granulocytosis, with absolute white blood counts ranging from 10,100 to 25,000 (normal range is 4000 to 10,000).
..")
67
Although granulocyte colony – stimulating activity can be demonstrated in serum and/or urine in 80 percent of patients, the specific peptide hormone causing the syndrome has not been identified.

68
Tumor production of granulocyte colony – stimulating factor (G-CSF), granulocyte- monocyte colony – stimulating factor (GM- CSF), and interleukin-6 (IL-6) has been shown in a minority of patients.
, granulocyte- monocyte colony – stimulating factor (GM- CSF), and interleukin-6 (IL-6) has been shown in a minority of patients.")
69
Clinical: All patients with lung cancer who present with tumor - associated granulocytosis are asymptomatic.

70
Diagnosis: - The diagnosis is suggested by the presence of an increased white blood count in which neutrophils predominate without immature forms, in the absence of non neoplastic causes. - An increased leukocyte alkaline phosphatase score and a normal bone marrow are consistent with this diagnosis.

71
Thrombocytosis: Thrombocytosis is common in patients with lung cancer, afflicting 40 percent of patients with both non – small-cell and small-cell tumors.

72
Pathogenesis: The pathogenesis of thrombocytosis in patients with lung cancer has not been totally explained. IL-6, which is a cytokine for megakaryocytes, has been demonstrated in cell lines from patients with lung cancer and thrombocytosis, and increased levels of IL-6 have been demonstrated in the plasma of such patients.

73
The recent identification of the thrombopoietin gene should lead to a better understanding of the role of this protein in paraneoplastic thrombocytosis.

74
Clinical: Patients with thrombocytosis are nearly always asymptomatic and do not have an increased incidence of thromboembolism. The diagnosis of cancer-associated thrombocytosis is suggested by an increased platelet count (above 500,000/mm2) in a patient with newly diagnosed lung cancer.
 in a patient with newly diagnosed lung cancer..")
75
A primary myeloproliferative disorder can be excluded only by a bone marrow biopsy.

76
Thromboembolism: Twenty percent of patients with lung cancer develop venous thrombo embolism during the course of their disease. Twenty percent of patients who present with recurrent idiopathic venous thrombosis are found to have an underlying diagnosis of cancer.

77
THANK YOU

Similar presentations




















 F.R.C.P. (E) F.R.C.P. (LONDON) F.A.C.C DESIGNED AT A.V. DEPT F.J.M.C.>")

