Download presentation
Presentation is loading. Please wait.

1
Nodules and infiltrates

2
Pulmonary TB, main radiological aspects and differential diagnoses
Common TB in adults Miliary Serous membrane TB Node TB Pleural TB Sequela Tuberculosis and AIDS: AIDS modifies the clinical and radiological course of TB. Differential diagnoses are many. It is important to know them, in order to chose the adapted treatment

3
Common adult TB Basic radiological images:
Nodule Infiltrate Cavity Tuberculous pneumonia

4
These elements are very often associated in the same patient
- These images can follow in time : nodule macronodule excavated nodule caverna These elements are very often associated in the same patient The association of several images of different ages and different aspects is very indicative for TB Round picture with a diameter > 3 cm, non- excavated, is very rarely TB

5
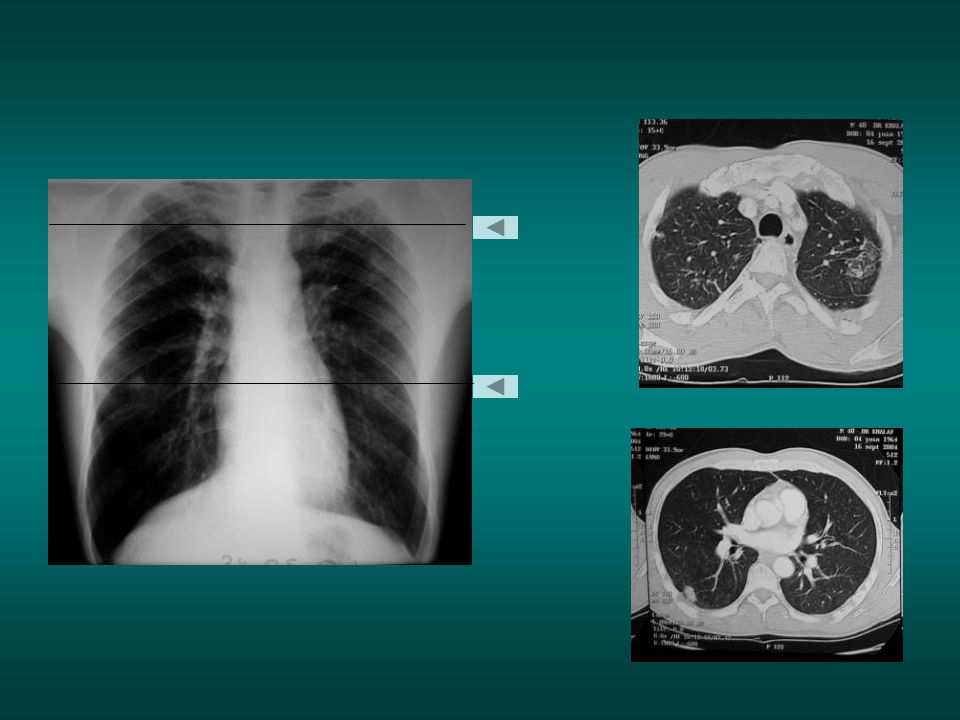
Nodule: isolated or grouped in the superior lobes or in the apical segment of the inferior lobes. Infiltrate: group of various-sized nodules with unequal dimensions. The excavation is not always visible on the chest x-ray. If the excavation exists, the bacterial analysis of the sputum is generally positive: TPM+. (The TDM could show the excavation even if it is not visible on the chest x-ray)
.")
6
. For the supra clavicles area analysis, the chest x-ray with antero posterior incidence is usefull.

7
Probable TB infiltrate
Tuberculine skin test 5U = 15mm Good performance status, FS = 0, Physical signs = 0 Inflammatory S = 0 Expectoration: AFB - Cultures - Probable TB infiltrate

8
TB infiltrate TPM-

9
Probable TB infiltrate
Non productive cough Good performance status, FS = 0, Physical signs = 0 Inflammatory S = 0 Expectoration: AFB - Cultures - Probable TB infiltrate

10
Cough, chronic fever. Hemoptoïc sputum. AFB neg. in sputum

12
Man, 55 years old Antecedent of pleural effusion Fever, cough, weight loss Hemoptoic sputum Chest x-ray: left pleural sequela, retractile Right nodular infiltrate. AFB+ in sputum

13
cavited nodules >>> AFB+

14
Woman 48years old. Close contact with patient AFB+ in sputum.
PCR positive in sputum for mycobacterium tuberculosis in sputum

15
San view of the previous case : microcavity in the nodule

16
Man ,heavy smoker, cough, dyspnea and worsening condition
AFB + in sputum

17
cavited nodule Tubercular pneumonia

18
AFB positive in sputums
cavity. AFB positive in sputums Bronchoscopic view: tubercular endobronchic lesion With tubercular granulomas In the biopsy samplings

19
Small TB infiltrate TPM-

20
Bilateral nodules. AFB- in sputum. BK Cultures negative

22
nodule macronodule cavited nodule cavity In this case, association of an infiltrate in the right superior lobe and cavity in the left inferior lobe is highly indicative of TB

23
TB nodules and infiltrates are most often isolated or grouped in the superior lobes or in the apical segment of the inferior lobes. - They are difficult to see in the retro-clavicle area - These lesions are often AFB- because non-excavated, no communication with bronchi and pauci-bacillar - The association of lesions with different seniority (nodules, cavity, sequelas) or with extra pulmonary localisations is very indicative of TB.
 or with extra pulmonary localisations is very indicative of TB.")
24
Nodules and infiltrates are often AFB- in sputum
Nodules and infiltrates are often AFB- in sputum. So the risk of contamination is low (but not zero). AFB is negative in sputum, but sometimes cultures are positive. Even if the risk of contamination is low, it is important to detect these patients and treat them because these patients can develop severe and contaminent TB
. AFB is negative in sputum, but sometimes cultures are positive. Even if the risk of contamination is low, it is important to detect these patients and treat them because these patients can develop severe and contaminent TB.")
25
Cough, fever, weight loss, asthenia
Male, 30 years old Cough, fever, weight loss, asthenia T left upper lobe infiltrate not noticed by the physician (not good quality of CXR) Amoxicillin treatment…
 Amoxicillin treatment…")
26
4 months later: left superior excavation with important infiltrate,
AFB +++

27
Nodules and Infiltrate -Summary
Sometimes difficult to see (small, retroclavicular areas) Sometimes AFB+ if cavity (not always visible on CXR) Most often no cavitation and AFB- They are true TB on the beginning and must be treated by anti TB They are true TPM - Physicians of national TB program hesitate to treat these patients but they treat a lot of “TPM – who are not real TB (bronchial cancer, inactive sequella bronchectasis, aspergilloma…) It is absolutely necessary to improve quality of CXR interpretation Especially for physicians in charge of TB program.
 Sometimes AFB+ if cavity (not always visible on CXR) Most often no cavitation and AFB- They are true TB on the beginning and must be treated by anti TB. They are true TPM - Physicians of national TB program hesitate to treat these patients but they treat a lot of TPM – who are not real TB (bronchial cancer, inactive sequella bronchectasis, aspergilloma…) It is absolutely necessary to improve quality of CXR interpretation. Especially for physicians in charge of TB program.")
Similar presentations


 Active TB Routine; FBE WCC (Infection) Hb (Anaemic of chronic disease) U&Es (baseline) LFTs (baseline) ESR/CRP (inflammation/infection)>")


 The diagnosis of miliary requires a chest radio of good quality and careful analysis of the image The radiological image.>")






 vs HIV (-) TB Infection 3-13% every year 5% first 2 years >30% lifetime >")







