Download presentation
Presentation is loading. Please wait.

1
Causes Blood loss – usually from uterus or GI tract Increased demands such as growth and pregnancy Decreased absorption – post gastrectomy, Coeliac disease Poor intake

2
Clinical Features Symptoms of anaemia: fatigue, headaches, faintness, breathlessness, angina, palpitations, intermittent claudication Brittle hair and nails Koilonychia Painless glossitis Angular stomatitis A syndrome of dysphagia (due to pharyngeal webbing) and glossitis = Plummer-Vinson or Paterson-Kelly
 and glossitis = Plummer-Vinson or Paterson-Kelly")
3
Diagnosis History: -dietary intake -? NSAIDS -? Blood in faeces -Menstrual history

4
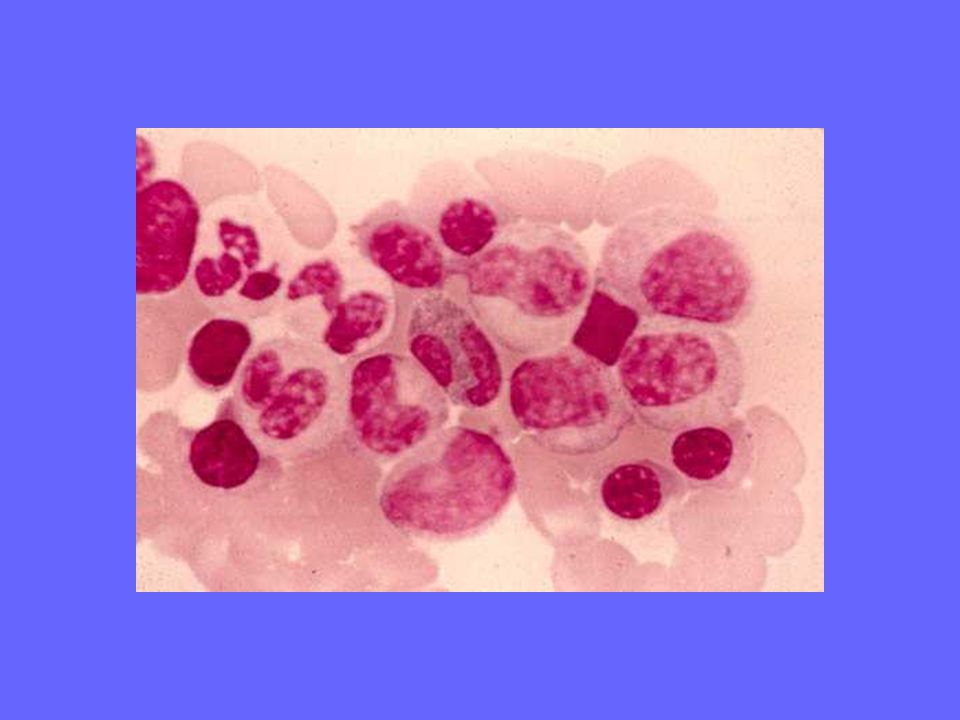
Investigations Blood count and film - microcytic (MCV <80fl) and hypochromic (MCH <27pg) - poikilocytosis, anisocytosis, pencil cells
 and hypochromic (MCH <27pg) - poikilocytosis, anisocytosis, pencil cells")
5
Investigations Serum iron decreased TIBC increased Transferrin saturation is commonly below 19% Serum ferritin reflects the amount of stored iron low in iron deficiency (normal 30-300μg/L) Serum soluble transferrin receptor is increased. This may help to distinguish between iron deficiency anaemia and anaemia of chronic disease

6
Investigations Bone marrow: -erythroid hyperplasia, ragged normoblasts -Staining using Perl’s reaction doesn’t show the characteristic blue granules of stainable iron -Not essential for diagnosis but may be helpful in the investigation of complex cases of anaemia

8
Investigations Other: (used to determine the cause of the iron deficiency) -Faecal occult bloods -MSU -Endoscopic studies of the GI tract -Clotting studies -Hookworm ova in stools -e.g. Giardiasis -Endomysial and gluten antibodies +/- duodenal biopsy

9
Differential Diagnosis Anaemia of Chronic Disease: -Serum ferritin normal or raised; TIBC reduced; SSTR normal, iron present in marrow Thalassaemia: -Serum I, TIBC, ferritin and SSTR normal, iron present in marrow and erythroblasts Sideroblastic anaemia: - Raised serum iron, normal TIBC, raised serum ferritin, iron present in the marrow, ring sideroblasts seen

10
Treatment Treat the underlying cause Give iron to correct anaemia and replenish iron stores. Can monitor response using reticulocyte count and Hb level – expect ~1g Hb rise per week Oral iron – commonly ferrous sulfate 200mg tds -best given on an empty stomach -Should be taken for at least 6 months -Side effects = nausea, abdo pain, constipation/diarrhoea take with food or reduce the dose -Vit C can be used to improve absorption – and avoid tea (phytates)
.")
11
Treatment If failing to respond to oral therapy then consider 1)lack of compliance 2)Continuing haemorrhage 3)Incorrect diagnosis e.g. thalassaemia trait 4)Mixed deficiency If none of these apply then may need to proceed to parenteral iron
Mixed deficiency If none of these apply then may need to proceed to parenteral iron.")
12
Treatment Parenteral iron: -iron-sorbitol-citrate given IM or ferric hydroxide- sucrose by slow IV infusion -May be hypersensitivity or anaphylactic reactions so only give if need to replenish iron rapidly (eg late pregnancy), if on haemodialysis and EPO therapy or when oral iron is ineffective or impractical (active Crohn’s) -The haematological response is no faster than with oral iron but the iron stores are replaced much faster -Calculate the required dose based on the degree of anaemia and the patient’s body weight
, if on haemodialysis and EPO therapy or when oral iron is ineffective or impractical (active Crohn’s) -The haematological response is no faster than with oral iron but the iron stores are replaced much faster -Calculate the required dose based on the degree of anaemia and the patient’s body weight")
Similar presentations







/ HYPOCHROMIC &/or (NORMO)/ MICROCYTIC ANEMIAS 1. Disorders of iron utilization a. iron deficiency b. anemia of.>")











