Download presentation
Presentation is loading. Please wait.

1
Lower Abdominal Pain Aashesh Verma July 2013 Dr. Sclamberg & Dr. Cameron

2
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Disease Expected Imaging Treatment Options Our Patient Outline

3
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Disease Expected Imaging Treatment Options Our Patient Outline

4
The patient is a 45 y/o female with a known history of fibroids diagnosed on US at OSH who presents to the ED with progressively worsening lower abdominal pain. The patient describes the pain as achy and cramping located in the LLQ, RLQ and suprapubic regions. The patient denies any f/c, n/v, bleeding or diarrhea/constipation. History

5
Vitals: Stable General: NAD, A&Ox3 Abdominal: Soft, distended, normoactive BS, ttp in LLQ and RLQ, no hepatosplenomegaly, multiple lower abdominal masses are palpable Physical

6
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Disease Expected Imaging Treatment Options Our Patient Outline

7
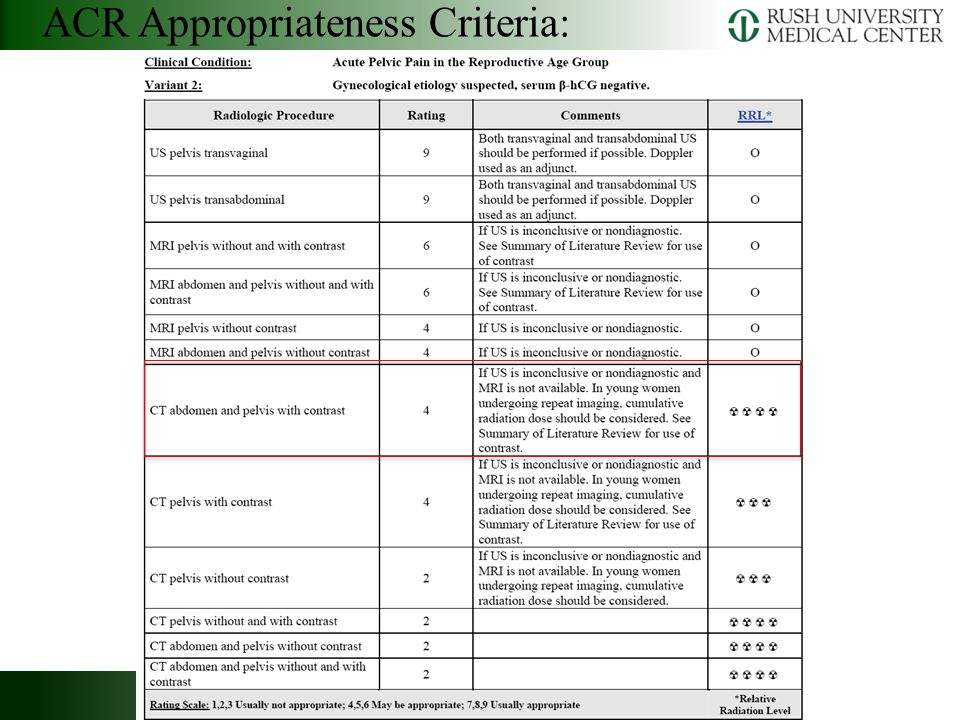
ACR Appropriateness Criteria:

9
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Disease Expected Imaging Treatment Options Our Patient Outline

13
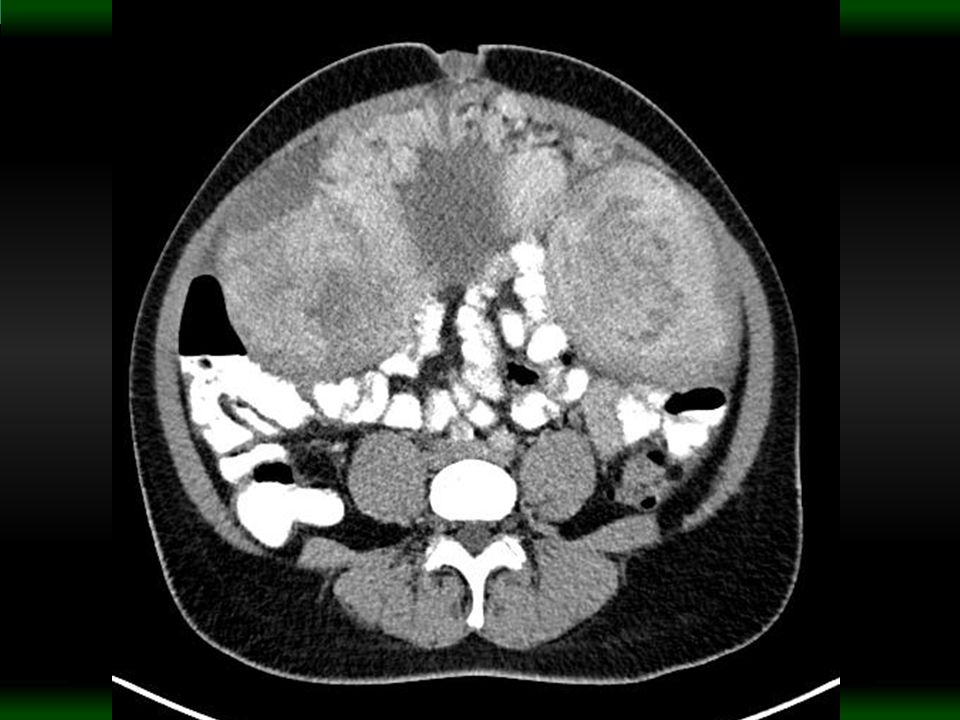
Several heterogeneously enhancing lesions are visualized within the abdomen and pelvis One mass has a lobulated continuation with the right aspect of the uterus The uterus itself has a leiomyomatous appearance Left-para aortic space has several lobulated hypodense masses Mild to moderate ascites CT Abd-Pelvis w/ Contrast MRN: 6572547 Accession #: 5311403

14
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Disease Expected Imaging Treatment Options Our Patient Outline

15
-Disseminated Peritoneal Leiomyomatosis -Benign Metastasizing Leiomyomas -Lymphangioleiomyomatosis -Disseminated Leiomyosarcoma -Metastatic Ovarian Cancer -Peritoneal Carcinoma Differential Diagnosis

16
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Fibroids Expected Imaging Treatment Options Our Patient Outline

17
Leiomyomas, or fibroids, are benign monoclonal tumors that typically originate from the smooth muscle of the uterine myometrium Fibroids are the most common uterine neoplasm, occurring in up to 70% of women by age 50 More common in African American women, and typically more severe Hormone dependent, respond to both Estrogen and Progesterone Risk Factors include early age of menarche and obesity (likely secondary to increased Estrogen exposure) Fibroids
 Fibroids")
18
Classification of Fibroids Stewart, 2012

19
As fibroids enlarge, they can outgrow their blood supply, resulting in various types of degeneration – Hyaline degeneration Homogeneous plaques of proteinaceous tissue in extracellular space – Myxoid Degeneration Gelatinous, hyaluronic acid rich mucopolysaccharides – Calcification – Cystic Degeneration – Red (hemorrhagic) Degeneration Secondary to hemorrhagic infarction, during pregnancy Fibroids
 Degeneration Secondary to hemorrhagic infarction, during pregnancy Fibroids")
20
Majority of women are asymptomatic 20 – 50% have symptoms that include: – Abnormal Uterine Bleeding Most Common Symptom – Pelvic Pain and Pressure Secondary to Mass Effect – Reproductive Dysfunction Secondary to distortion of the uterine cavity Fibroids

21
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Fibroids Expected Imaging Treatment Options Our Patient Outline

22
Usually not identified on plain X-Ray Seen only if they are calcified or rarely as a large soft tissue mass displacing bowel gas Plain Radiography

23
KUB Calcification Overlying the Left Hip CT Subsequently shows Calcified Fibroid Sue and Sarah, 2009

24
Ideally the initial investigation to examine the female pelvis Transvaginal scans are more sensitive, able to detect fibroids as small as 5mm Findings: – Well-defined solid mass with whorled appearance – Usually similar echogenicity to myometrium – May cause alteration of normal uterine contour – Often show a degree of posterior shadowing Ultrasound

25
Transvaginal Ultrasound Arrow: 1.1cm Sub- mucosal Fibroid Arrow- heads: showing posterior shadowing Sue and Sarah, 2009

26
Transabdominal Ultrasound Bulky Uterus 10cm submucosal fibroid between cursors Sue and Sarah, 2009

27
Transabdominal US 7cm intramural fibroid Arrows: cystic areas Sue and Sarah, 2009

28
MR is the most accurate imaging technique for detection and localization of fibroids More sensitive than US Demonstrates uterine zonal anatomy Good for differentiating between: – Submucosal – Intramural – Subserosal MRI

29
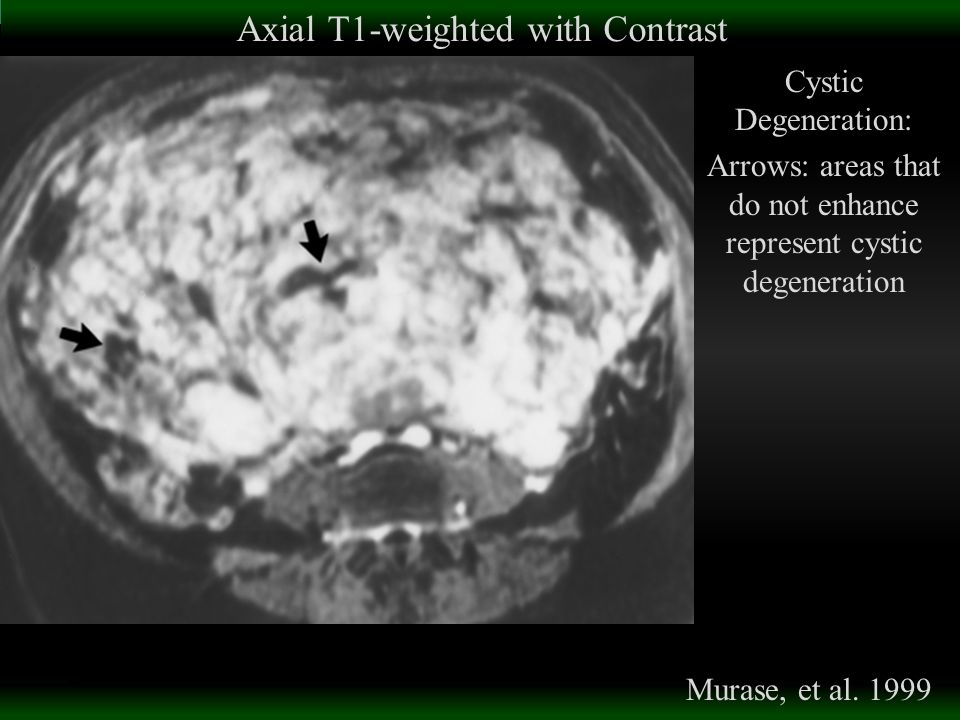
Nondegenerate uterine fibroids have a typical appearance: – Well-circumscribed masses of homogeneously decreased signal intensity compared to the myometrium on T2- weighted images Degenerated fibroids have a variable appearance: – Hyaline or Calcific Degeneration Low Signal Intensity on T2, similar to standard fibroids – Cystic Degeneration High Signal Intensity on T2, the cystic areas do not enhance – Myxoid Degeneration Very high Signal Intensity on T2, enhance minimally with contrast – Necrotic Degeneration Low Signal Intensity on T2 – Red (hemorrhagic) Degeneration Peripheral high signal intensity on T1 Variable intensity on T2, with/without low-intensity rim MRI
 Degeneration Peripheral high signal intensity on T1 Variable intensity on T2, with/without low-intensity rim MRI")
30
Axial T2-weighted Murase, et al. 1999 * - Intramural Straight Arrow – Submucosal Curved Arrow – Subserosal

31
Axial T1-weighted Red Degeneration: Peripheral High Signal Intensity Murase, et al. 1999

32
Axial T1-weighted with Contrast Cystic Degeneration: Arrows: areas that do not enhance represent cystic degeneration Murase, et al. 1999
33
Sagittal T2-weighted Myxoid Degeneration: Well circumscribed mass, with components of high signal intensity (arrowheads) Sue and Sarah, 2009
 Sue and Sarah, 2009")
34
Not the primary modality for diagnosing or evaluating fibroids However, fibroids are often found incidentally on CT Typical Finding: bulky, irregular uterus or mass in continuity with the uterus IV contrast is often heterogeneous Degeneration: diminished contrast enhancement and areas of low attenuation Key Finding: Solid “mass-type” calcifications in the uterus are the most specific sign for leiomyomas CT

35
Axial CT with contrast Several bulky, irregular masses in continuity with the uterus with areas of calcification (arrows) Sue and Sarah, 2009
 Sue and Sarah, 2009")
36
Axial Contrast-Enhancing CT Bennet, et al. 2002 Thick walled mass with air fluid level with a coarse calcification (arrow)
.")
37
Axial CT Sue and Sarah, 2009 Large heterogeneous mass Histologically confirmed to be a partially degenerate fibroid

38
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Fibroids Expected Imaging Treatment Options Our Patient Outline

39
Asymptomatic fibroids can be followed without intervention Gonadotropin-releasing hormone agonists are considered the most effective medical therapy Surgery is indicated for abnormal uterine bleeding or bulk-related symptoms – Hysterectomy – Myomectomy – Endometrial Ablation (if only submucosal fibroids) Treatment
 Treatment")
40
IR Options: Uterine Artery Embolization – Women who wish to preserve their uterus – Advantages: shorter hospital stay, less pain – Disadvantages: higher failure rate with larger fibroids High rate of re-intervention for treatment failure Magnetic Resonance Guided focused Ultrasound – Premenopausal women who have completed childbearing – Advantages: rapid recovery and low short-term morbidity – Disadvantages: time consuming and costly Treatment

41
History and Physical Choice of Imaging Radiographic Findings Differential Diagnoses Background on Fibroids Expected Imaging Treatment Options Our Patient Outline

42
Patient was discharged from the ED and sent to OB/GYN to obtain specimen for pathology, with expected diagnosis of diffuse leiomyomatosis Records do not show a pathological specimen at this time Follow-up

43
Murase, E ; Siegelman, ES ; Outwater, EK ; et al.” Uterine leiomyomas: Histopathologic features, MR imaging findings, differential diagnosis, and treatment” Radiographics. 1999. 19;5: 1179 – 97. Wilde S, Scott-Barrett S. “Radiological appearances of uterine fibroids.” Indian J Radiol Imaging. 2009. Jul-Sep;19(3):222-31. Bennett GL, Slywotzky CM, Giovanniello G. “Gynecologic causes of acute pelvic pain: spectrum of CT findings.” Radiographics. 2002. Jul- Aug;22(4):785-801. Stewart, Elizabeth A. "Epidemiology, Clinical Manifestations, Diagnosis, and Natural History of Uterine Leiomyomas (fibroids)." UpToDate. UpToDate, 1 June 2012. Web Stewart, Elizabeth A. "Overview of Treatment of Uterine Leiomyomas (fibroids)." UpToDate. N.p., 27 Feb. 2012. Web. Works Cited and Referenced
: Bennett GL, Slywotzky CM, Giovanniello G. Gynecologic causes of acute pelvic pain: spectrum of CT findings. Radiographics Jul- Aug;22(4): Stewart, Elizabeth A. Epidemiology, Clinical Manifestations, Diagnosis, and Natural History of Uterine Leiomyomas (fibroids). UpToDate. UpToDate, 1 June Web Stewart, Elizabeth A. Overview of Treatment of Uterine Leiomyomas (fibroids). UpToDate. N.p., 27 Feb Web. Works Cited and Referenced.")
44
Thank You! The END

Similar presentations














>")






