Download presentation
Presentation is loading. Please wait.

1
Routes for Vaccine Administration: Intramuscular, Subcutaneous, Intradermal and Intranasal Ruth Carrico PhD RN FSHEA CIC Associate Professor Division of Infectious Diseases University of Louisville

2
Objectives Describe basic infection prevention and control relevant to administration of medication including vaccines Review administration of vaccines via intramuscular, subcutaneous, intradermal, and intranasal routes Apply knowledge of administration techniques in simulated setting

3
Infection Prevention Practice Competencies Safe Injection Practices – Role of microorganisms in disease – Transmission – Precautions – Problem solving – Preparedness

4
Injection Safety Measures taken to perform injections in a safe manner for patients and providers Part of Standard Precautions – Infection prevention practices that apply to all patients, regardless of suspected or confirmed infection status, in any healthcare setting Healthcare should not provide any opportunity for transmission of bloodborne viruses – Patient protections in the context of IV injections should be on par with transfusion safety and healthcare worker safety (OSHA BBP Standard)
")
5
Transmission of Bloodborne Pathogens Via Unsafe Injection Practices SOURCE Infectious person, e.g. chronic, acute CASE Susceptible, non-immune person CONTAMINATED INJECTABLE EQUIPMENT OR PARENTERAL MEDICATION Limit or eliminate reuse

6
Standard Precautions Assume that anyone might be infected with a bloodborne pathogen Basic infection control principles that apply every where and every time healthcare is delivered Safe Injection Practices – Never administer medications from the same syringe to more than one patient – Do not enter a vial with a used syringe or needle – Minimize the use of shared medications – Maintain aseptic technique at all times

7
What are some of the incorrect practices that have resulted in transmission of pathogens? Direct (i.e., “overt”) syringe reuse – Using the same syringe from patient to patient (even if needle changed) Indirect syringe reuse – Accessing shared medication vials with a used syringe Reuse of single dose vials Contamination of multidose vials Using a common bag of saline or other IV fluid for more than one patient – Leaving IV set in place for dispensing fluid – Accessing IV bag with syringe that has already been used to flush a catheter Sharing of blood contaminated glucose monitoring equipment Preparing medications in area contaminated with used syringes
 syringe reuse – Using the same syringe from patient to patient (even if needle changed) Indirect syringe reuse – Accessing shared medication vials with a used syringe Reuse of single dose vials Contamination of multidose vials Using a common bag of saline or other IV fluid for more than one patient – Leaving IV set in place for dispensing fluid – Accessing IV bag with syringe that has already been used to flush a catheter Sharing of blood contaminated glucose monitoring equipment Preparing medications in area contaminated with used syringes.")
8
Storage of multidose vials and preparation of injections in same area that used needles and syringes were dismantled and discarded FACT: injection preparation on surfaces where contaminated substances are handled can lead to the spread of infections Ref: Samandari et al. ICHE 2005; 26: 745-750 Photo: Don Weiss / NYCDOHMH

9
Indirect Syringe Reuse Nevada endoscopy center HCV outbreak investigation, 2008 Syringes were reused to withdraw multiple doses for individual patients Remaining volume in single dose propofol vials was used for subsequent patients The vial became the vehicle for HCV spread

10
Misperceptions I changed the needle so I can reuse the syringe The vial says single dose but it has enough medication for more than one patient, so I can use it This is an emergency situation so I can push aside strict adherence with good technique

11
Examples of some “BIG IF s” IF I’m going to be throwing away this vial after this case, I can reuse this syringe to draw more meds IF we always use a new needle and syringe to draw meds, it’s OK to reuse vials IF I’m very careful, I can safely predraw multiple syringes from this saline bag or vial IF I keep things straight, I can predraw meds for the next person while I am preparing for the present person

12
Injection Safety – Standard Precautions Use aseptic technique during the preparation and administration of injected medications Do not use medication drawn into a single syringe for multiple patients, even if the needle is changed Consider a syringe or needle contaminated after it has been used to enter or connect to a patients’ intravenous infusion bag or administration set Do not enter a vial with a used syringe or needle Single dose vials have no preservative so the vial must be discarded after that single dose Adapted from: CDC. Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings 2007. http://www.cdc.gov/ncidod/dhqp/gl_isolation.html

13
Minimizing the use of shared medications affords an extra layer of protection to reduce patient risk Use single-dose medication vials whenever possible Single-dose vials should not be used for more than one patient Multi-dose vials have preservatives but still require aseptic technique when entered Adapted from: CDC. Guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings 2007. http://www.cdc.gov/ncidod/dhqp/gl_isolation.html

14
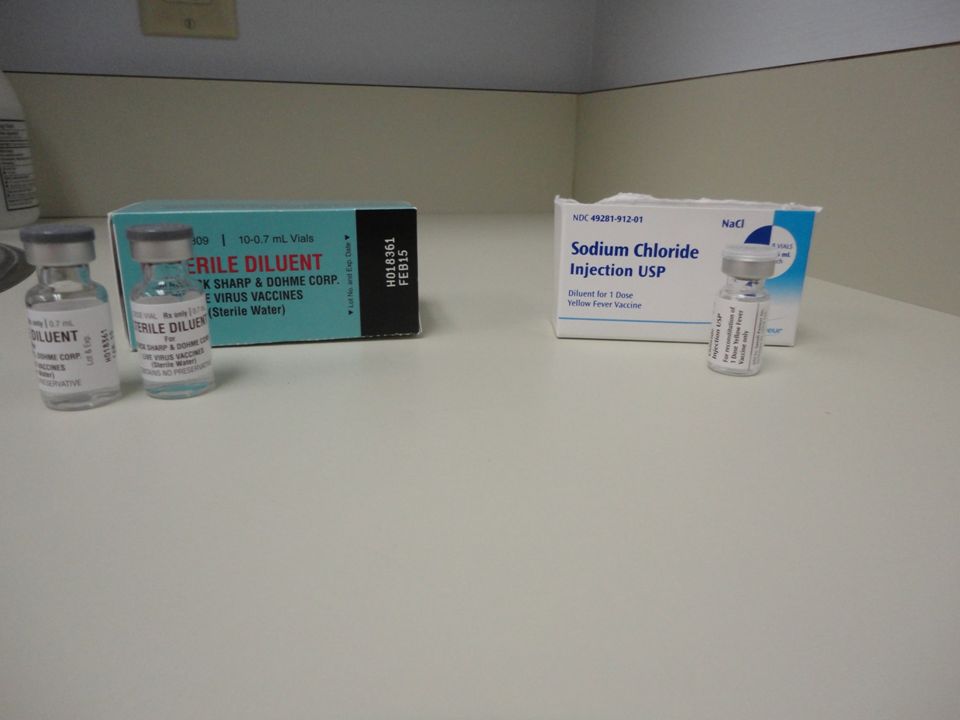
Basics of assessment and triage prior to pharmaceutical agent administration Be aware of purpose of the pharmaceutical intervention Know the agent (action, the 5 Rs, contraindications, other safety issues) Know the type of vaccine (live or killed) Know the targeted patient population Special needs necessitate special interventions
 Know the type of vaccine (live or killed) Know the targeted patient population Special needs necessitate special interventions")
15
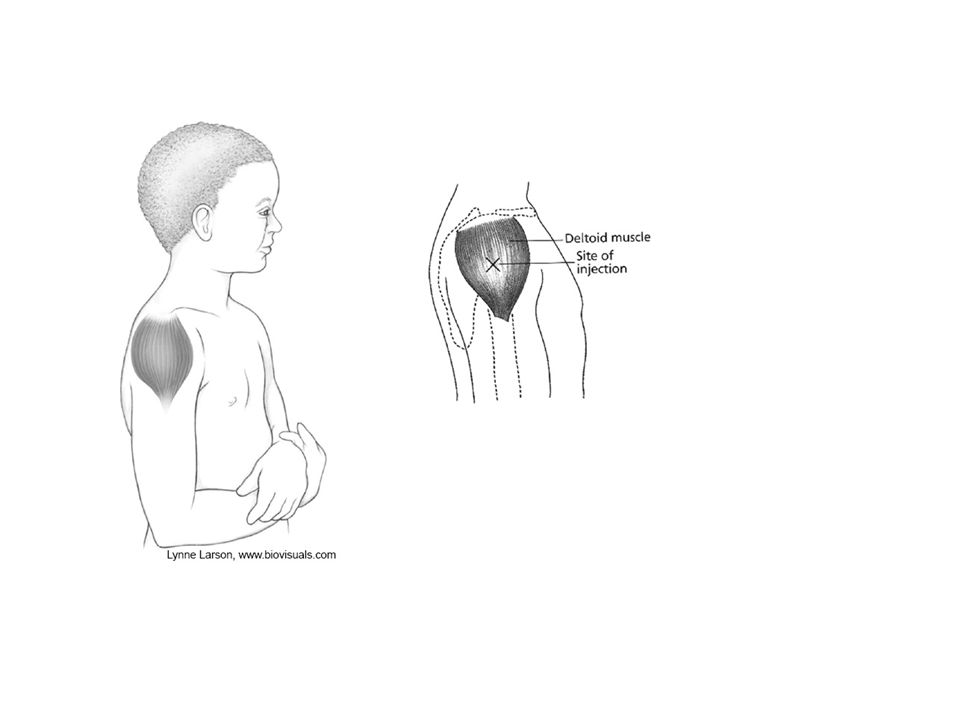
Intramuscular Injection Sites Children (3-18 years) – Deltoid – 22 to 25 gauge 5/8 to 1 inch needle depending upon body mass – May use gluteal muscle but know the landmarks Adults (19 years and older) – Deltoid using 1 inch to 1 ½ inch needle 130-152 lbs use 1 inch 152-200 lbs 1 to 1 ½ inch >200 lbs use 1 ½ inch – Can use anterolateral thigh if deltoid not an option
 – Deltoid – 22 to 25 gauge 5/8 to 1 inch needle depending upon body mass – May use gluteal muscle but know the landmarks Adults (19 years and older) – Deltoid using 1 inch to 1 ½ inch needle lbs use 1 inch lbs 1 to 1 ½ inch >200 lbs use 1 ½ inch – Can use anterolateral thigh if deltoid not an option")
16
Intramuscular Injection Sites Infants <12 months – Anterolateral aspect of the thigh (vastus lateralis muscle) is preferred site – 22-25 gauge needle – 5/8 inch needle for neonates (first 28 days of life) and preterm infants – 1 inch for others Toddlers (12 months-2 years) – Anterolateral thigh using 1 inch needle – Can use deltoid if muscle mass is adequate. May use 5/8 inch needle for deltoid.

17
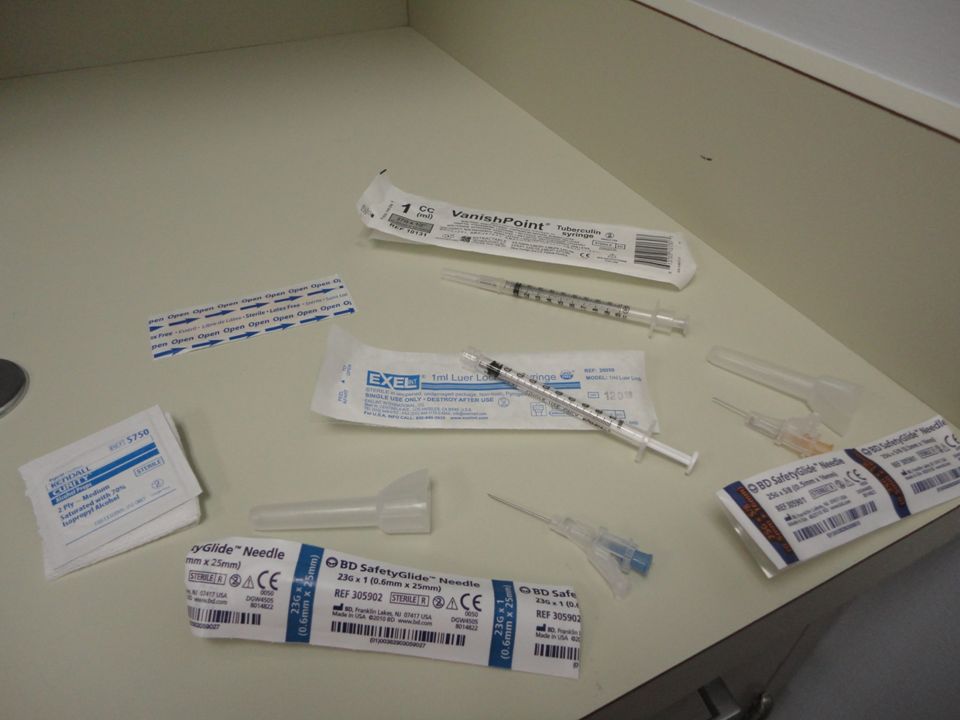
Steps in administration of intramuscular, intradermal, intranasal, subcutaneous and oral vaccines/agents Know administration site Be aware of any special handling required of the vaccine or agent Be familiar with the steps involved in administration Be familiar with equipment and supplies Identify critical steps in the process Practice, when possible

28
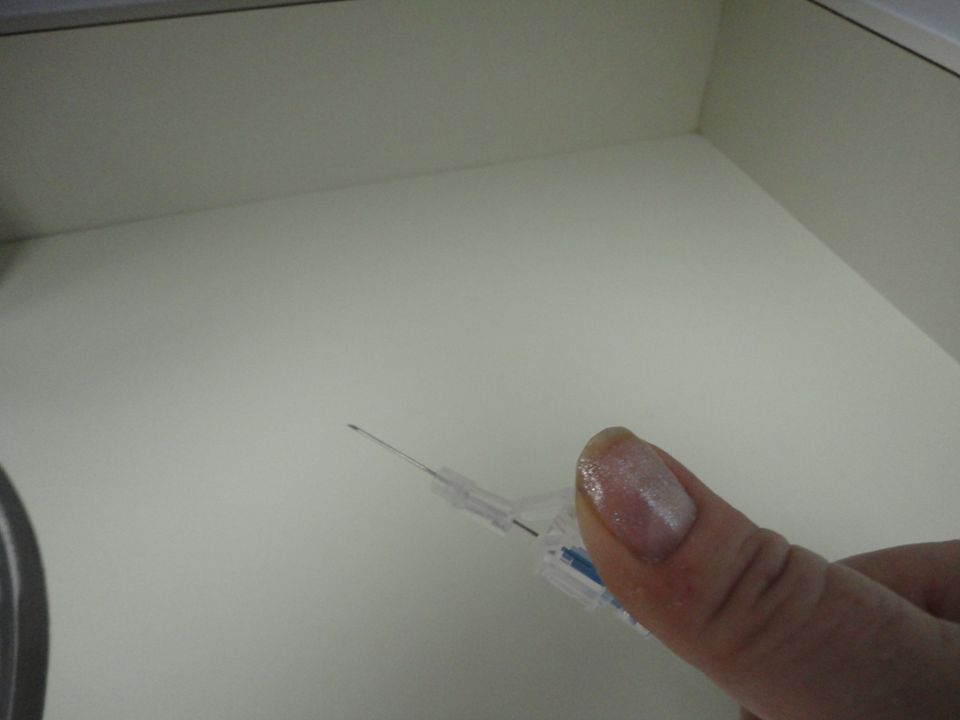
Needle Selection for Intramuscular Injection Injection technique is critical Use of a longer needle has been associated with less redness or swelling than with a shorter needle Needle must be long enough to reach the muscle mass and prevent seeping into subcutaneous tissue. Vaccinators must be familiar with the anatomy of the area in which the vaccine is to be injected Needles are inserted at 90° angle for intramuscular injection in children and adults

29
Subcutaneous Involves injection of the agent into the tissue beneath the skin but above the muscle Generally requires a needle of approximately 5/8 of an inch Area of administration is generally in the upper third of the upper arm away from larger muscles, in the abdomen or thigh.

36
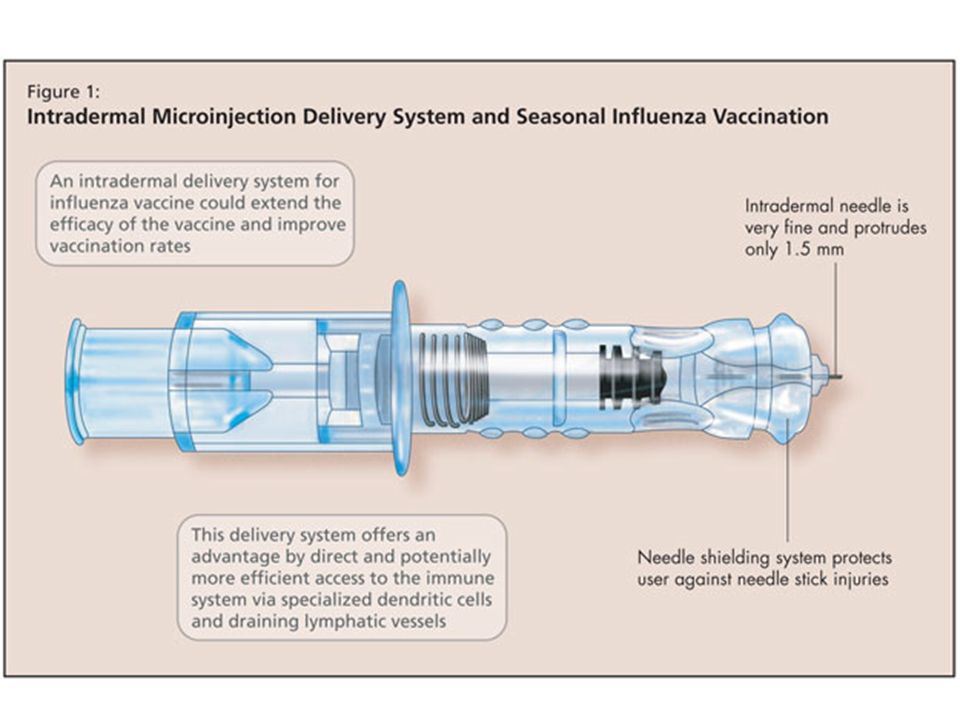
Intradermal Intradermal administration utilizes a smaller needle length and administers a smaller dose volume. Administration of intradermal vaccine differs from other intradermal medication administration such as the TB skin test At present, the intradermal flu vaccine comes in its own prefilled syringe. Verify the age requirements for this, and all other vaccines Let the vaccine recipient know what to expect following immunization

42
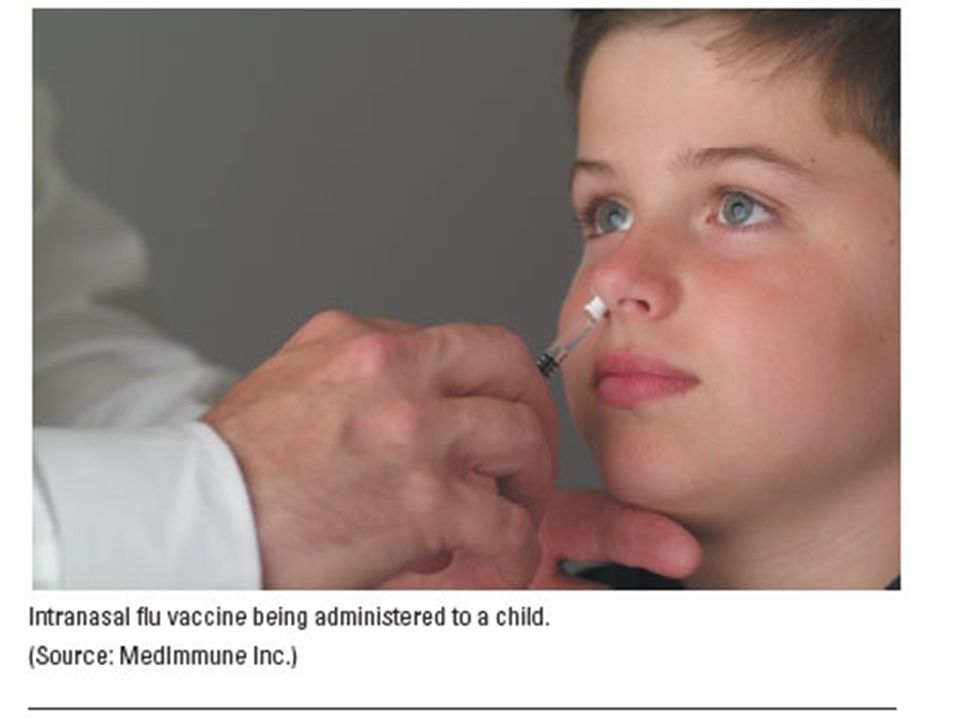
Intranasal Know equipment Position patient Provide tissue Prepare the patient for administration Administer the dose Provide post-immunization education Dispose of supplies and equipment Hand hygiene

43
Patient Positioning Dependent upon age, ability to participate, setting for administration, type of pharmaceutical agent Children may need secure, comforting position that prevents movement Injection position influenced by setting (e.g., sitting, drive-thru, standing) Intranasal may be given sitting, standing, drive- thru Oral agent administration v. dispensing

47
Handling and Disposal of Medical Waste Regulated – Blood/potentially infectious body fluids, some pharmaceutical wastes – Federal and state regulations – Impacts disposal as well as transporting waste – Designated receptacles Non-regulated – General trash – Items not considered to be soaked, saturated with blood, body fluids, or other potentially infectious material; non- regulated biologic/pharmaceutical waste

Similar presentations























 中国医科大学护理学院 王健. Medications (three) PARENTERAL MEDICATIONS Nurses given parenteral medications intradermally (ID), subcutaneously (SC or SQ),>")








 to humans from other humans, animals or the.>")


