Download presentation
Presentation is loading. Please wait.

2
Pathophysiology of asthma and chronic obstructive pulmonary disease M. Tatár

4
OBSTRUCTIVE LUNG DISEASES localized: laryngeal constriction, tracheal and bronchial carcinoma, foreign bodies localized: laryngeal constriction, tracheal and bronchial carcinoma, foreign bodies generalized: asthma, COPD, bronchiectasis, cystic fibrosis OBSTRUCTIVE VENTILATORY DISORDER - spirometry Airflow limitation

6
0.5 End of quiet expiration - 0.5 0 0 0 00 Inspiration - 2.5

7
0.5 - 2.5 0 - 1.0 - 0.5 - 1.5 - 2.0 Inspiration Forcedexpiration + 2.0

8
0.5 Forced expiration + 2.0 + 2.5 0 + 2.0+ 1.5 + 1.0 EPP

9
ASTHMA - definition Chronic inflammatory disorder of the airways Mast cells, eosinophils, T-lymphocytes Recurrent episodes of wheezing, dyspnoea, and cough particularly at night and early morning Symptoms are associated with airflow limitation that is partly reversible either spontaneously or with therapy Bronchial hyperresponsiveness is present very often

10
1234512345 Time (seconds) FEV 1 Volume Normal subject Asthmatic (after bronchodilator) Asthmatic (before bronchodilator)
 FEV 1 Volume Normal subject Asthmatic (after bronchodilator) Asthmatic (before bronchodilator)")
11
ASTHMA - classification A. Intrinsic asthma no environmental causes can be identified negative skin test to common airborn allergens rather negative family history B. Extrinsic asthma atopy, genetic predisposition IgE, mast cells and eosinophils response to allergens C. Occupational asthma sensibilisation of airways to inhalant chemicals

12
Development of asthma Risk factors Predisposing: atopy, gender Causal: allergens, aspirin, chemicals Contributing: respiratory infections, diet, air pollution, smoking Factors that exacerbate asthma - triggers allergens, respiratory infections, exercise, emotions

13
Respiratory infections epithelial damage airway inflammation Exercise reflex airflow limitation cooling of mucosa osmolarity changes of fluid lining epithelium Emotions (laughing, crying, anger, fear) hyperventilation hypocapniaTriggers
 hyperventilation hypocapniaTriggers")
14
Asthma - bronchial hyperresponsiveness Instability of the airways = exaggerated bronchoconstrictor response to a wide variety of stimuli Key factor - airway inflammation Mechanisms: direct and indirect

15
Direct agonists e.g. methacholine Airway with limited airflow Mediators Nerve SO 2, bradykinin Indirect agonists e.g. exercise, adenosine, hypotonic or hypertonic aerosols Mast cell Airway hyperresponsiveness

16
balance antihyperreactiv factors antihyperreactiv factors prohyperreactiv factors Normal airway reactivity 2 -adrenergic VIP/PHM anticholinergic NEP antioxidants corticoids -adrenergic cholinergic SP/NK oxygen-free radicals peptidases Airway hyperresponsiveness im

17
Pathological changes in chronic asthma Normal airway Airway wall remodeling Epithelium Basement membrane Smooth muscle Mucus plug Mucus glands

18
Mechanisms of asthma 1. Airway inflammation - recruitments of inflammatory cells from circulation - endothelial adhesion molecules - activation of T lymphocytes (Th 2 clone) - production of IgE, leukotriens, prostanoids - cytokines (CD4+ Th subtype) 2. Neural control of airways
 - production of IgE, leukotriens, prostanoids - cytokines (CD4+ Th subtype) 2. Neural control of airways.")
20
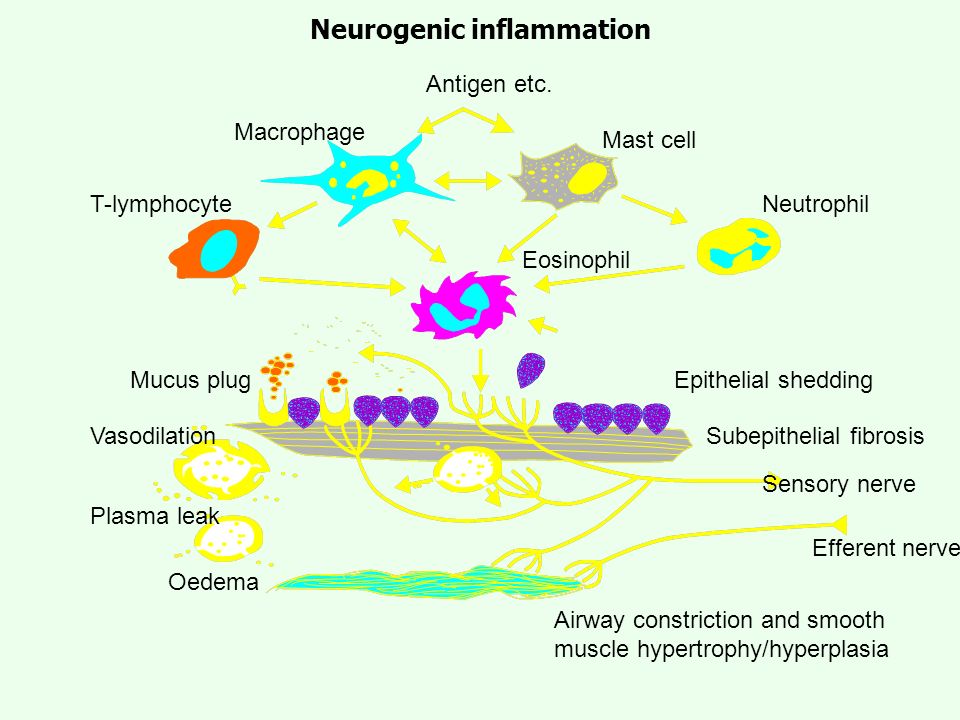
Antigen etc. Macrophage T-lymphocyteNeutrophil Mast cell Eosinophil Mucus plug Vasodilation Plasma leak Oedema Epithelial shedding Subepithelial fibrosis Sensory nerve Efferent nerve Airway constriction and smooth muscle hypertrophy/hyperplasia Neurogenic inflammation

21
Asthma - airflow limitation 1. Acute bronchoconstriction 2. Swelling of the airway wall 3. Chronic mucus plug formation 4. Airway wall remodeling

22
RelaxationConstriction Normal Asthma Airway narrowing Exaggerated airway narrowing R = 1 R = 1 R = 10 R = 10 R = 2 R = 2 R = 40 R = 40 muscle constriction 35 %

23
INFLAMMATION Risk factors (for development of asthma) Airway hyperresponsiveness Airflow limitation Risk factors (for exacerbations) Symptoms
 Airway hyperresponsiveness Airflow limitation Risk factors (for exacerbations) Symptoms")
24
Asthma is a highly variable disease Asthma is a chronic inflammatory disease of variable severity. Worsening and exacerbations of asthma are associated with episodes of acute inflammation, which develop on top of persistent underlying chronic inflammation. This acute inflammation causes an increase in symptoms and may also lead to an increased sensitivity to triggers and a worsening in airway hyperresponsiveness. The variability and severity of „real life“ asthma is dependent on a number of factors, including a patient´s adherence to the prescribed treatment.

27
COPD - definition Chronic airflow limitation ( maximum expiratory flow, slow forced emptying of the lungs) Airflow limitation is slowly progressive and irreversible Due to varying combinations of: airway disease emphysema
 Airflow limitation is slowly progressive and irreversible Due to varying combinations of: airway disease emphysema")
28
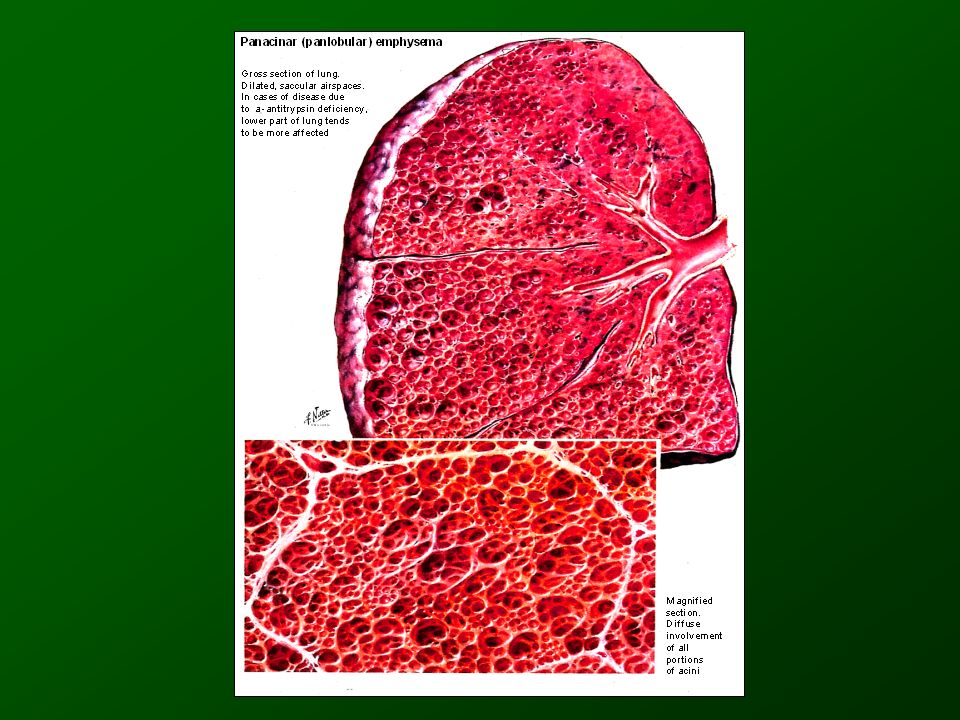
COPD Chronic bronchitis defined in clinical terms chronic cough with sputum production - (3 months a year, 2 successive years) - excluded cardiac or other pulmonary causes Emphysema Emphysema defined anatomically permanent, destructive enlagrement of airspaces distal to the terminal bronchioles without obvious fibrosis
 - excluded cardiac or other pulmonary causes Emphysema Emphysema defined anatomically permanent, destructive enlagrement of airspaces distal to the terminal bronchioles without obvious fibrosis")
32
COPD - risk factors Cigarette smoking 1 - antitrypsin deficiency Solid fuel used for indoor heating or cooking without adequate ventilation Heavily polluted environments

33
100 75 50 25 0 50 75 Age yrs FEV 1 % Disability Death Never smoked Stopped at age 45 yrs age 45 yrs Stopped at age 65 yrs Smoked regularly

34
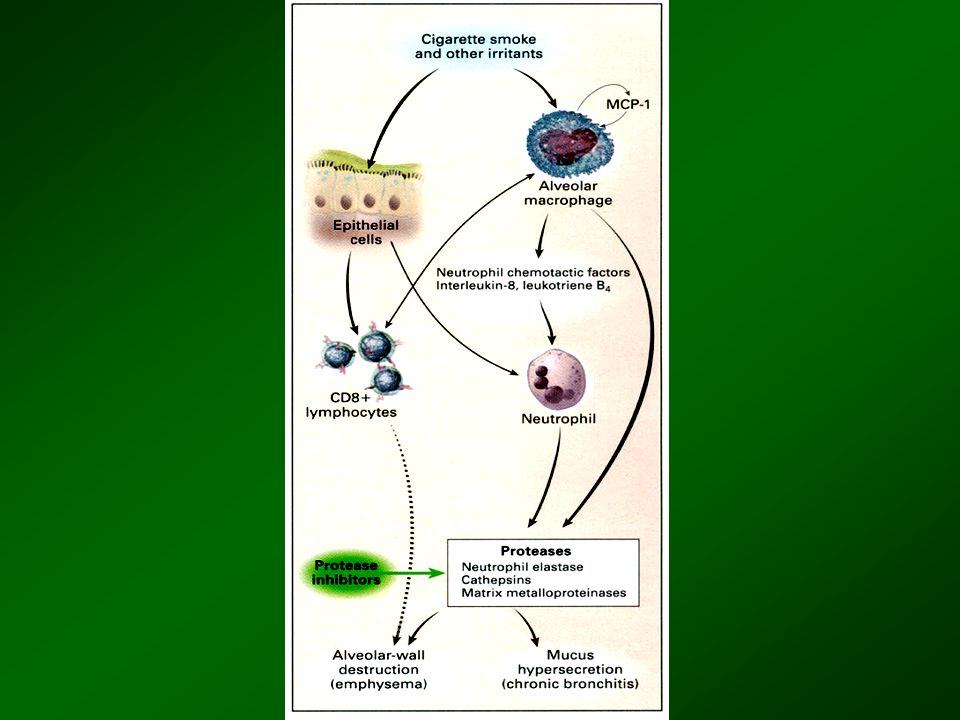
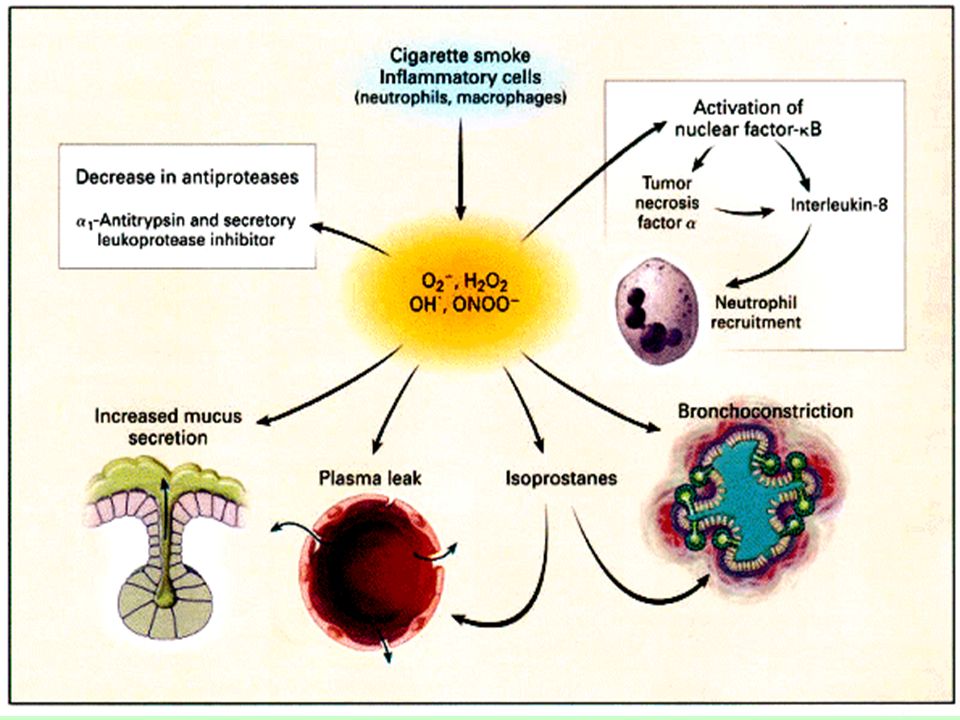
COPD - cellular and biochemical mechanisms Inflammation: alveolar macrophages, neutrophils Neutrophil and macrophage enzymes and oxidants destroy components of extracellular matrix (collagen, elastin, fibronectine, proteoglycans) Loss of cellular components of lung parenchyma: - elastase can induce apoptosis - cells exposed to oxidants may undergo apoptosis or necrosis oxidative stress in smokers and in COPD patients production of elastase, cathepsine G, collagenase
 Loss of cellular components of lung parenchyma: - elastase can induce apoptosis - cells exposed to oxidants may undergo apoptosis or necrosis oxidative stress in smokers and in COPD patients production of elastase, cathepsine G, collagenase")
35
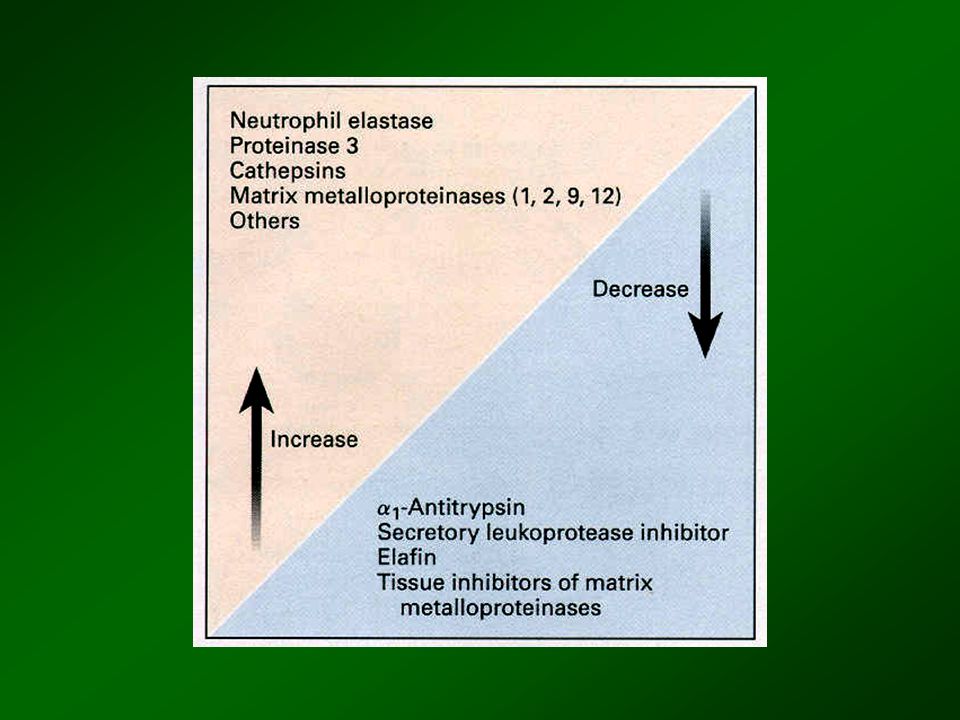
COPD - cellular and biochemical mechanisms Destruction of lung parenchyma Imbalance proteases antiproteases system oxidants antioxidants Small airways disorder

41
COPD - pathology of peripheral airways mucus plugging goblet cell metaplasia fibrosis smooth muscle hypertrophy

43
102345 Volume from TLC ( l ) - 6 0 6 12 V´ ( l.s -1 ) Maximal expiratory effort Spontaneous breath
 V´ ( l.s -1 ) Maximal expiratory effort Spontaneous breath")
44
0 2040 60 80 100 Lung volume (% TLC) Oxygen consumption (ml.min -1.kg -1 ) Normals VTVT IRV V T IRV Airflow limit
 Oxygen consumption (ml.min -1.kg -1 ) Normals VTVT IRV V T IRV Airflow limit")
46
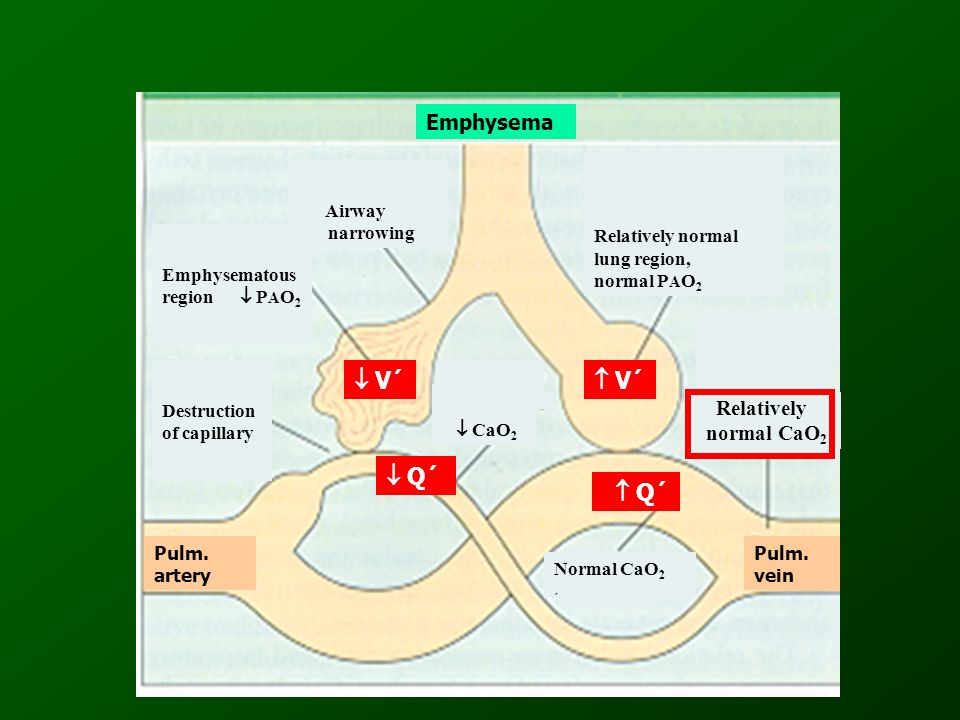
Relatively normal lung region, normal P A O 2 Emphysema Pulm. vein Pulm. artery Normal CaO 2 ´ CaO 2 Airway narrowing Emphysematous region P A O 2 Destruction of capillary V´ V´ Q´ Q´ Relatively normal CaO 2

48
Relatively normal lung region, normal P AO 2 normal CaO 2 Airway narrowing Pulm. v.Pulm. a. Bronchitis P AO 2 CaO 2 V´ norm V´ norm Q´ CaO 2

49
0 4 6 10 0,5 1,0 1,52,02,53,0 FEV 1 ( l ) Pa CO 2 ( kPa )
 Pa CO 2 ( kPa )")
50
Sleep period 20 40 60 80 100 Oxygen saturation ( % ) REM
 REM")
51
Components of chronic obstructive pulmonary disease Airflow limitation by spirometry Chronic bronchitisEmphysema Asthma Simple bronchitis Asthma with no airflow limitation Emphysema but no COPD

Similar presentations












>")




>")
Asthma 2)COPD 3)Comparison.>")







