Download presentation
Presentation is loading. Please wait.

1
Proton Therapy for Lung Cancer Therapeutic Advance or The Straw that Broke the U.S. Medical System’s Back? Jeffrey A. Bogart M.D. Upstate Medical University November 15, 2013

2
Disclosures Chair, Alliance Radiation Oncology Committee – Stipend Upstate Medical University recently signed a MOU with Advanced Oncotherapy PLC to proceed with developing a proton therapy center

3
Learning Objectives Review current state of the art (radio)therapy for locally advanced NSCLC Describe available evidence for proton therapy in treatment of early stage NSCLC Discuss opportunities and challenges in treatment of locally advanced NSCLC with proton therapy
therapy for locally advanced NSCLC Describe available evidence for proton therapy in treatment of early stage NSCLC Discuss opportunities and challenges in treatment of locally advanced NSCLC with proton therapy")
4
Background Stage III NSCLC – Primary RT: Local tumor control ~ 15% – ChemoRT: In-field failure 33%+ (RTOG 9410) Hypothesis: Modulating RT delivery will improve local control and ultimately survival
 Hypothesis: Modulating RT delivery will improve local control and ultimately survival")
5
RT Practice Standards The new millennium … – IMRT, IGRT, 4D planning now routine – Should shift therapeutic index – But..no change in the radiotherapy dose schedule for locally advanced NSCLC since the 1970’s 6000 cGy / 6 weeks

6
3D Dose Escalation Dose Escalation : Conventional Fractionation 74 Gy in 2 Gy fractions was feasible with concurrent weekly paclitaxel and carboplatin TrialPhasenMed survival RTOG 9410 (63Gy)III20017 months UNC 9603I/II6224 mo CALGB 30105II4324 mo NCCTG 0028I1337 mo RTOG 0117I/II44 (stage 3)21.6 mo
III20017 months UNC 9603I/II6224 mo CALGB 30105II4324 mo NCCTG 0028I1337 mo RTOG 0117I/II44 (stage 3)21.6 mo")
7
Concurrent Chemotherapy: RTOG 0617 STRATIFYSTRATIFY RT Technique 1.3D-CRT 2.IMRT Zubrod 1.0 2.1 PET Staging 1.No 2.Yes Histology 1.Squamous 2.Non- Squamous RANDOMIZERANDOMIZE Concurrent TreatmentConsolidation Treatment Arm A Concurrent chemotherapy* RT to 60 Gy, 5 x per wk for 6 wks Arm A Consolidation chemotherapy* Arm B Concurrent chemotherapy* RT to 74 Gy, 5 x per wk for 7.5 wks Arm B Consolidation chemotherapy* Arm C Concurrent chemotherapy* and Cetuximab RT to 60 Gy, 5 x per wk for 6 wks Arm C Consolidation chemotherapy* and Cetuximab Arm D Concurrent chemotherapy* and Cetuximab RT to 74 Gy, 5 x per wk for 7.5 wks Arm D Consolidation chemotherapy* and Cetuximab Bradley, ASCO 2013

8
RTOG 0617 Local Relapse also increased (37%) on 74 Gy arm Well conducted trial allowing state of the art technology and good QA Bradley, ASCO 2013 ArmMedian OSSevere Esophagitis Grade 5 Toxicity 60 Gy28.7 months7%2 patients 74 Gy19.5 months21%10 patients
 on 74 Gy arm Well conducted trial allowing state of the art technology and good QA Bradley, ASCO 2013 ArmMedian OSSevere Esophagitis Grade 5 Toxicity 60 Gy28.7 months7%2 patients 74 Gy19.5 months21%10 patients")
9
Conventional RT Traditional “protracted” dose escalation is a flawed and failed strategy in combined modality therapy Protracted Conventional Radiotherapy Locally Advanced NSCLC

10
What Now? Alternate Radiotherapy Schedules

11
Hyperfractionation RTOG 9410: 1.2 Gy BID to 69.6 Gy –Lower dose per fx reduced toxicity? Curran, JNCI 2011 Con.STD 63GyCon. HFX 69.6 Gy Median survival17 mo15.6 5-year survival16%13% Acute Esop. Tox.22%45% Late Pulm. Tox.13%19%

12
Hypofractionation TrialRT RegimenChemoSurvivalLate Toxicity EORTC (1999-03) 2.75 Gy x 24 (66 Gy) Cisplatin 6 mg/m2 daily 3 yr: 33%4 % Esophageal 18 % Pulmonary SOCCAR 2.75 Gy x 20 (55 Gy) Cisplatin/ vinorelbine 27.6 mo median “acceptable” Stricture? KROG (2003-05) 2.4 Gy x 25 (60 Gy) Paclitaxel/ carboplatin 28.1 mo median 2 hemoptysis 3 stricture Higher dose per fraction – Safe with advanced technology?
 2.4 Gy x 25 (60 Gy) Paclitaxel/ carboplatin 28.1 mo median 2 hemoptysis 3 stricture Higher dose per fraction – Safe with advanced technology .")
13
Active Photon Studies Stage III ChemoRT CALGB 31102 Phase I : Maintain Total Dose at 60Gy Increase dose/fraction - reduce treatment time Next cohort : 3 Gy x 20 Fx over 4 weeks RTOG 1106 Random phase II : individualized adaptive RT using during-treatment FDG-PET/CT Doses as high as 85 Gy in 30 fx given

14
What Else? Charged particle therapy

15
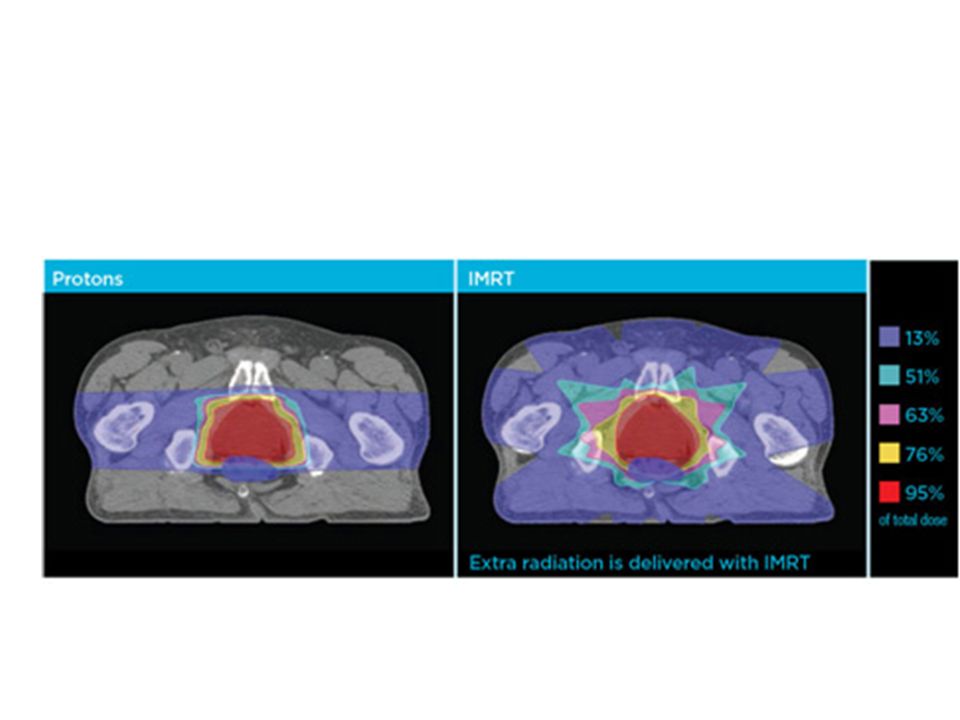
Proton Therapy + Charged Particle Physical properties differ from photons – Potential for better protection of normal structures – But treatment planning relatively immature c/w photons Passive Scattering (~ 3D) : majority of published studies IMPT (~ IMRT) – dose painting Biologic efficacy similar
 : majority of published studies IMPT (~ IMRT) – dose painting Biologic efficacy similar")
16
Precise Energy Placement 16

17
17 Pediatric Malignancies Reduced dose to normal tissue -limit impact on growth -reduce secondary malignancy risk

18
Proton Therapy Cost : $25,000,000 to > $200,000,000

20
Building Boom of Proton Beam Centers Flares Up in Washington and Baltimore Cancer Letter : Oct 25, 2013 “About 100,000 people have been treated with proton beam radiation, and about 85 percent of them received it for prostate cancer “ - Level 1 evidence supporting protons over photons does not exist - Undue severe toxicity has not been reported

22
Early Lung Cancer

23
Photon SBRT

24
“Protons generate larger high-dose regions than photons because of range uncertainties. This can result in nearby healthy organs (e.g., chest wall) receiving close to the prescription dose, at least when two to three beams are used, such as in our study” Seco et al Red Journal 2012
 receiving close to the prescription dose, at least when two to three beams are used, such as in our study Seco et al Red Journal")
25
Georg Radioth Onc 2008 Reduced (low dose) lung, heart, esophagus dose with proton SBRT
 lung, heart, esophagus dose with proton SBRT")
26
Photon SBRT RTOG 0236 60 Gy / 3 fx (peripheral tumors only) 97% in-field local control Timmerman JAMA 2010
 97% in-field local control Timmerman JAMA 2010")
27
Proton Therapy Early Lung Cancer Loma Linda (2013) – 111 patients, T1+ T2 tumors – 4-year OS dose dependent :18% (50 Gy), 32% (60 Gy), 51%(70 Gy) – Local Control 96% for Peripheral T1 if 60 Gy + – Clinical radiation pneumonitis was not found to be a significant complication “Meta-analysis” (2010) – “ Five-year overall survival similar with SBRT (42%), proton therapy (40%) and carbon-iontherapy (42%). However, caution is warranted due to the limited number of patients and limited length of follow-up of the particle studies” Bush et al Red Journal 2013Grutters et al Radioth Oncol 2010

28
Proton Therapy Locally Advanced Lung Cancer Photon IMRT

29
Proton Therapy Locally Advanced Lung Cancer V20 Lung = Volume of Lung Receiving 20 Gy

30
Proton Therapy Locally Advanced NSCLC Chang et al Red Journal 2006

31
Stage III NSCLC Does what we see on paper (or the computer screen) translate into real life?
 translate into real life")
32
Proton Therapy Locally Advanced Lung Cancer Complicating Factors Depth of penetration /Bragg peak varies significantly based on the density of tissues Range uncertainty (extra margin of safety) Tumor Motion introduces further uncertainty
 Tumor Motion introduces further uncertainty")
33
PT + Chemotherapy Stage III NSCLC Phase II (MD Anderson, n = 44) – 74 Gy(RBE) + weekly carboplatin (AUC 2) and paclitaxel (50 mg/m2 ) – FDG-PET/CT staged – passively scattered proton – Cone beam CT not available Median Survival 29.4 months (19.7 month median FU) – Local relapse 20.5 %, 9.3 % nodal relapse Toxicity – 11.4% grade 3 dermatitis, 11.4% grade 3 esophagitis – 1 grade 3 pneumonitis and 1 pulmonary/pleural fistula Chang et al Cancer 2011
 – 74 Gy(RBE) + weekly carboplatin (AUC 2) and paclitaxel (50 mg/m2 ) – FDG-PET/CT staged – passively scattered proton – Cone beam CT not available Median Survival 29.4 months (19.7 month median FU) – Local relapse 20.5 %, 9.3 % nodal relapse Toxicity – 11.4% grade 3 dermatitis, 11.4% grade 3 esophagitis – 1 grade 3 pneumonitis and 1 pulmonary/pleural fistula Chang et al Cancer 2011")
34
PT + Chemotherapy Stage III NSCLC University of Florida (n = 19) – Median 74 Gy(RBE) + chemotherapy – Median 16 month FU Toxicity – 1 acute grade 3 and 1 late grade 3 non-hematologic toxicity 1 documented in-field progression Hoppe et al Lung Cancer 2012
 – Median 74 Gy(RBE) + chemotherapy – Median 16 month FU Toxicity – 1 acute grade 3 and 1 late grade 3 non-hematologic toxicity 1 documented in-field progression Hoppe et al Lung Cancer 2012")
35
Locally Advanced Primary RT – Poor DFS/OS with PT alone Re-irradiation(n= 33) – MD Anderson – Repeat RT to 66 Gy (median 3 year interval) – 54% 1-yr local control, 9/33 in-field relapse – Toxicity Gr 3 : 9% Esophageal, 21 % pulmonary Gr 4 : 3% Esophageal, 7 % pulmonary PORT/Mediastinal RT – Better Protect Heart and Surrounding Lung c/w photon McAvoy et al Radiother Oncol 2013
 – MD Anderson – Repeat RT to 66 Gy (median 3 year interval) – 54% 1-yr local control, 9/33 in-field relapse – Toxicity Gr 3 : 9% Esophageal, 21 % pulmonary Gr 4 : 3% Esophageal, 7 % pulmonary PORT/Mediastinal RT – Better Protect Heart and Surrounding Lung c/w photon McAvoy et al Radiother Oncol 2013")
36
Stratify Stage 1.II 2.IIIA 3.IIIB GTV 1.<= 130 cc 2.>130 cc Histology 1.Squamous 2.Non-Squamous Neoadjuvant Chemotherapy 1.Yes 2.No RANDOMIZATION Photon: Highest achievable dose between 60-70 Gy at 2 Gy, once daily plus platinum-based doublet chemotherapy Protons: Highest achievable dose between 60-70 Gy (RBE) at 2 Gy (RBE) once daily plus platinum- based doublet chemotherapy Arms 1 and 2: Consolidation Chemotherapy x 2 is allowed Arm 1 Arm 2 RTOG 1308: Phase III Randomized Trial Comparing Overall Survival after Photon vs. Proton Radiochemotherapy for Stage II-IIIB NSCLC Plan must meet dose and volume constraints of all OARs

37
Stage III Trials Ongoing and planned trials evaluating proton therapy – Preoperative therapy – Hypofractionated – IMPT with simultaneous integrated boost

38
Conclusions RTOG 0617 set the bar high : 28 month median OS –Modern staging (FDG-PET) –Sophisticated Treatment Planning Whether altering fractionation, dose, or treatment particle will improve outcomes is unclear Proton therapy has potential to permit less toxic delivery of intensive RT … but limited data –Treatment techniques rapidly evolving (IMPT/CBCT) PT may facilitate getting to the the right RT schedule
 –Sophisticated Treatment Planning Whether altering fractionation, dose, or treatment particle will improve outcomes is unclear Proton therapy has potential to permit less toxic delivery of intensive RT … but limited data –Treatment techniques rapidly evolving (IMPT/CBCT) PT may facilitate getting to the the right RT schedule")
Similar presentations


 CISPLATIN 40 mg/m2 Days 1 2 22 36 50 64 92 E V A L U A.>")








: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")







