Download presentation
Presentation is loading. Please wait.

1
Upper Respiratory Tract Infections

2
Upper R.T infections account for more visits to physicians than any other diagnosis.
In USA pharyngitis alone accounts for 40 million physician visits annually. Respiratory tract infections include: rhinitis, sinusitis, otitis media, pharyngitis, epiglottitis, bronchitis, bronchiolitis and pneumonia. Pneumonia is the leading cause of death in children worldwide. It kills children below five years old more than AIDS, malaria and tuberculosis combined.

3
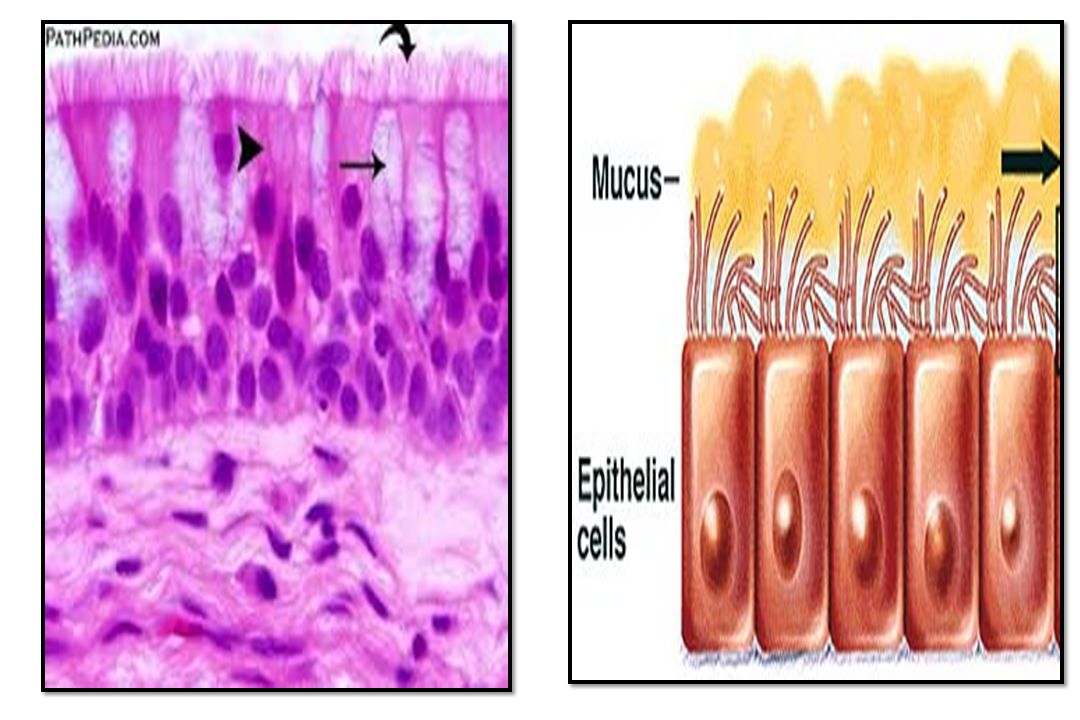
Defense Mechanisms of Respiratory system
The defense begins in the nose, through specialized hairs (vibrissae) that filter large particles from inhaled air. Epiglottis: protects airway from aspiration. Cough reflex. Mucociliary escalator. Alveolar macrophages (scavengers). Antimicrobial compounds: lysozyme, lactoferrin, complement and IgA.
 that filter large particles from inhaled air. Epiglottis: protects airway from aspiration. Cough reflex. Mucociliary escalator. Alveolar macrophages (scavengers). Antimicrobial compounds: lysozyme, lactoferrin, complement and IgA.")
5
Microbial Ports of Entry:
Direct inhalation. Aspiration of upper airway contents. Spreading along the mucous membrane surface. Hematogenous dissemination. Rarely: direct penetration.

6
Common cold Common cold (rhinitis) is a viral infection.
Infection of the upper respiratory tract (nose, nasopharynx and throat). Over 100 viruses can cause common cold. Preschool children are at greatest risk of frequent colds. Children have an average of 8 colds per year, adults 3 per year. Most people recover from common cold within a week or two.
. Over 100 viruses can cause common cold. Preschool children are at greatest risk of frequent colds. Children have an average of 8 colds per year, adults 3 per year. Most people recover from common cold within a week or two.")
7
Etiologies of Common Cold
Rhinoviruses 30 to 35%. Influenza and adenovirus-30%. Coronaviruses about 10%. human respiratory syncytial virus (RSV) &Parainfluenza. Miscellaneous viruses. Symptoms of common cold: Sore throat, runny nose, nasal congestion, sneezing, conjunctivitis (sometimes), myalgia, fatigue. Complications: Secondary bacterial infection (otitis media and sinusitis).
 &Parainfluenza. Miscellaneous viruses. Symptoms of common cold: Sore throat, runny nose, nasal congestion, sneezing, conjunctivitis (sometimes), myalgia, fatigue. Complications: Secondary bacterial infection (otitis media and sinusitis).")
8
Acute Otitis Media & Sinusitis
Causes of Otitis Media: Streptococcus pneumoniae (The most common bacterial cause), Haemophilus influenzae (The second common cause), S. pyogenes and Moraxella catarrhalis. Causes of Sinusitis: Community acquired bacterial sinusitis: S. pneumoniae, H. influenzae, S. pyogenes. Nosocomial sinusitis: in critically ill, mechanically ventilated patients: S. aureus, Pseudomonas aeruginosa, Serratia marcescens. Fungal sinusitis.
, Haemophilus influenzae (The second common cause), S. pyogenes and Moraxella catarrhalis. Causes of Sinusitis: Community acquired bacterial sinusitis: S. pneumoniae, H. influenzae, S. pyogenes. Nosocomial sinusitis: in critically ill, mechanically ventilated patients: S. aureus, Pseudomonas aeruginosa, Serratia marcescens. Fungal sinusitis.")
9
Throat Infection (Pharyngitis)
")
10
The most common cause of pharyngitis in school-aged children is group A Streptococci (S.pyogenes).
The next most common causes of pharyngitis are: In Oropharynx: EBV, adenoviruses and enteroviruses: Coxsackievirus group A causes herpangina (small vesicles on the mucus membrane of throat) and hand, foot and mouth disease. Non-group A streptococci. Chlamydophila pneumoniae. Gonococcus. Meningococcus. Corynebacterium diphtheriae.
 and hand, foot and mouth disease. Non-group A streptococci. Chlamydophila pneumoniae. Gonococcus. Meningococcus. Corynebacterium diphtheriae.")
11
In Nasopharynx (common cold):
Rhinoviruses, Coronaviruses, Influenza virus. Although no clinical features are diagnostic for specific etiologic cause of pharyngitis but: Fever, tonsillar exudates, and tender cervical adenopathy are usually associated with group A streptococci Infection. Conjunctivitis, cough, coryza, and diarrhea are usually associated with other causes.

12
Herpangina Hand, foot and mouth disease

13
S. pyogenes infection (Group A Streptococci):
Clinical presentations: Tonsillitis, pharyngitis, follicular tonsillitis, scarlet fever and septic shock. Toxigenic highly virulent strains of bacteria are associated with establishment of scarlet fever and septic shock ;(due to production of streptolysin-O, streptolysin-S and exotoxin, and exotoxin A). Scarlet fever*: Pharyngitis, fever, characteristic skin rash in the chest & extremities and bright red tongue with "strawberry" appearance. Scarlet = crimson, purple قرمزي.
. Scarlet fever*: Pharyngitis, fever, characteristic skin rash in the chest & extremities and bright red tongue with strawberry appearance. Scarlet = crimson, purple قرمزي.")
15
Infections by S. pyogenes can be complicated by:
Peritonsillar abscess. Sinusitis. Otitis media. Rheumatic fever. Glomerulonephritis.

16
Peritonsillar abscess

17
Diagnosis of S. pyogenes:
Clinical specimens: throat swab, nasopharyngeal swab and serum. Direct: Culture on blood agar or chocolate agar: beta-hemolytic, gram positive cocci in chains, capsulated and bacitracin sensitive. Indirect: serology: Anti streptolysin O titer (ASOT): significant titer is 200 IU or more.
: significant titer is 200 IU or more.")
18
Beta hemolytic bacitracin sensitive colonies

19
Asymptomatic meningococcal pharyngitis
Cause: Neisseria meningitides (gram –ve diplococci). Port of entry: inhalation of droplets from a carrier or a patient in the early stage of disease. Primary infection: Colonization of nasopharynx: asymptomatic pharyngitis (carriers). Secondary: Meningococcemia , and meningitis. Diagnosis: CSF culture on chocolate agar with 10% CO2.
. Port of entry: inhalation of droplets from a carrier or a patient in the early stage of disease. Primary infection: Colonization of nasopharynx: asymptomatic pharyngitis (carriers). Secondary: Meningococcemia , and meningitis. Diagnosis: CSF culture on chocolate agar with 10% CO2.")
20
Acute Epiglottitis: (Supraglottitis):
The most serious form of URTI. Most often in children 2 to 7 years of age. Most common cause in children is H. influenzae type b. Immunization of children (capsular Ag) reduced the percentage of infection. Causes of epiglottitis in adults: Streptococcus pneumoniae, Streptococcus pyogenes, H. influenzae. The infection results in rapid swelling of epiglottis and cause these symptoms: fever, difficult breathing and drooling of saliva. H. influenzae type b species can cross the mucosal barriers causing meningitis, and septic arthritis.
 reduced the percentage of infection. Causes of epiglottitis in adults: Streptococcus pneumoniae, Streptococcus pyogenes, H. influenzae. The infection results in rapid swelling of epiglottis and cause these symptoms: fever, difficult breathing and drooling of saliva. H. influenzae type b species can cross the mucosal barriers causing meningitis, and septic arthritis.")
21
Diagnosis of H. influenzae infection:
In Epiglottis infection: Radiology and blood culture. In Meningitis: Clinical specimens: CSF, Blood. Culture on chocolate agar at 10% CO2; because the microbe is fastidious for factor X (hemin) and V. (nicotinamide adenine dinucleotide).
 and V. (nicotinamide adenine dinucleotide).")
22
Treatment of H. influenzae infection:
Invasive infections: antibiotics e.g. third-generation cephalosporin (ceftriaxone) should be started as soon as appropriate specimens have been collected for culture. Sinusitis, otitis media, and other upper RTI: Trimethoprim-Sulfamethoxazole or amoxicillin-clavulanate combination.
 should be started as soon as appropriate specimens have been collected for culture. Sinusitis, otitis media, and other upper RTI: Trimethoprim-Sulfamethoxazole or amoxicillin-clavulanate combination.")
23
Croup: Infection of the Larynx (Laryngitis), Trachea (Tracheitis) and bronchi (bronchitis):
Almost all cases are caused by viruses esp. Parainfluenza viruses 1-3. In rare cases: Staphylococcus aureus. Children have smaller airways and nonexpendable rings of trachea so edema is more likely to cause narrowing of the lumen. Typically, mild upper R.T symptoms such as nasal discharge and dry cough are present days before signs of airway obstruction followed by sudden onset of barking cough and difficult respiration.

24
Treatment: It is a self-limited infection resolve after 5 to 7 days
Treatment: It is a self-limited infection resolve after 5 to 7 days. No specific antiviral drug. Corticosteroids and inhaled aerosolized epinephrine can be used.

25
Laryngitis and Bronchitis:
Laryngitis: in adults; the major clinical manifestation of larynx infection is hoarseness. Acute tracheobronchitis: Causes: Viruses: Rhinovirus, coronavirus, RSV, Influenzae virus. Bacteria: Chlamydophila pneumoniae, Mycoplasma pneumoniae, and Bordetella pertussis (the causative agent of whooping cough).
.")
26
Whooping cough Pathogenesis and virulence of B. pertussis (Toxins):
Whooping cough is a highly contagious fatal disease (outbreaks). Pathogenesis and virulence of B. pertussis (Toxins): Pertussis toxin: inhibition of immune cells response. Adenylate cyclase toxin; increase cAMP production: affect inflammation. Tracheal cytotoxin: Nitric oxide production: kill tracheal ciliated epithelial cells (paralyze the cilia and cause paroxysms to remove the mucus). Clinical presentation is characterized by two stages: Catarrhal stage:7-14 days; rhinorrhea, lacrimation, cough. Paroxysmal stage: (2 to 8 weeks): ten or more forceful coughs, cyanosis, and vomiting.
. Pathogenesis and virulence of B. pertussis (Toxins): Pertussis toxin: inhibition of immune cells response. Adenylate cyclase toxin; increase cAMP production: affect inflammation. Tracheal cytotoxin: Nitric oxide production: kill tracheal ciliated epithelial cells (paralyze the cilia and cause paroxysms to remove the mucus). Clinical presentation is characterized by two stages: Catarrhal stage:7-14 days; rhinorrhea, lacrimation, cough. Paroxysmal stage: (2 to 8 weeks): ten or more forceful coughs, cyanosis, and vomiting.")
27
Immunization in children (DTP) reduce Bordetella pertussis infection.
Diagnosis: The microbe can be isolated on charcoal cephalexin blood agar as mercury drop colonies Gram’s negative short, pleomorphic capsulated bacilli.

Similar presentations




 Lawrence Pike.>")







. The genus haemophilus organisms.>")








![BY RANJEET RAMAN GRAM NEGATIVE BACILLI- MICRO {ST1]](/15/4636473/big_thumb.jpg "BY RANJEET RAMAN GRAM NEGATIVE BACILLI- MICRO {ST1]>")