Download presentation
Presentation is loading. Please wait.

1
Notice Content: Clinical practice Time: 2:00pm this Thursday Address: Department of Neurosurgery, the 8th floor, No.5 Building , No.1, Hospital. Notice Content: Clinical practice Time: 2:00pm this Thursday Address: Department of Neurosurgery, the 8th floor, No.5 Building , No.1, Hospital.

2
Neurosurgery

3
INTRACRANIAL DYNAMICS

4
The first principle is obvious: the cranial cavity has a fixed volume that is filled by various things: 1. Brain tissue 2. CSF 3. Blood vessels and intravascular blood volume 4. Volume associated with any pathologic process, which can include tumor, cyst, abscess, hemorrhage, edema, necrosis

5
A consequence of this principle: If there is an elevation in the volume of any one compartment, there is a stage of compensation in which the volume of one or more other compartments can be reduced to avoid elevations in ICP.

6
QUESTION: What is Intracranial Pressure (ICP)? ICP : the pressure produced by the content of the cranial cavity (brain tissue, CSF and blood) on the cranial cavity wall. Normal ICP : Adult : 0.7 ~ 2.0 kPa ( 70 ~ 200mmH 2 O )。 Child : 0.5 ~ 1.0kPa ( 50 ~ 100mmH 2 O )。
 on the cranial cavity wall. Normal ICP : Adult : 0.7 ~ 2.0 kPa ( 70 ~ 200mmH 2 O )。 Child : 0.5 ~ 1.0kPa ( 50 ~ 100mmH 2 O )。.")
7
The second principle is not obvious and may seem counterintuitive: The spinal fluid is produced at a constant rate ( ∼ 15-20 mL/hr) largely by the choroid plexus of the ventricles by an energy- dependent, physicochemical process.
 largely by the choroid plexus of the ventricles by an energy- dependent, physicochemical process.")
8
The third basic principle: The cerebral blood flow (CBF) normally varies over a wide range (30-100 mL per 100 g brain tissue per minute), depending on metabolic demand from neuronal activity within a particular area of the brain.
 normally varies over a wide range ( mL per 100 g brain tissue per minute), depending on metabolic demand from neuronal activity within a particular area of the brain.")
9
For any brain region CBF=Cerebral perfusion pressure/ Cerebral vascular resistance For any brain region CBF=Cerebral perfusion pressure/ Cerebral vascular resistance

10
The fourth principle : Injured tissue swells, making obvious the potential for a cascading injury by a vicious cycle. If the stage of compensation mentioned earlier, even with therapy, is exceeded and ICP is elevated high enough by whatever mechanism so that cerebral perfusion pressure (CPP) declines, CBF can decline to levels where tissue injury occurs. The fourth principle : Injured tissue swells, making obvious the potential for a cascading injury by a vicious cycle. If the stage of compensation mentioned earlier, even with therapy, is exceeded and ICP is elevated high enough by whatever mechanism so that cerebral perfusion pressure (CPP) declines, CBF can decline to levels where tissue injury occurs.
 declines, CBF can decline to levels where tissue injury occurs. The fourth principle : Injured tissue swells, making obvious the potential for a cascading injury by a vicious cycle. If the stage of compensation mentioned earlier, even with therapy, is exceeded and ICP is elevated high enough by whatever mechanism so that cerebral perfusion pressure (CPP) declines, CBF can decline to levels where tissue injury occurs..")
11
Edema Infarction ICP CPP The vicious cycle. CPP, cerebral perfusion pressure; ICP, intracranial pressure.

12
Cerebral perfusion pressure (CPP) = mean systemic arterial pressure (MAP)-ICP
 = mean systemic arterial pressure (MAP)-ICP")
13
The fifth principle: Focal mass effect and its progression within the complex anatomy of the cranial cavity. The fifth principle: Focal mass effect and its progression within the complex anatomy of the cranial cavity.

14
A sixth principle: The separateness of the phenomenology of the following: 1. Focal mass effect 2. Diffuse raised ICP 3. Ventriculomegaly (enlargement of the cerebral ventricles) A sixth principle: The separateness of the phenomenology of the following: 1. Focal mass effect 2. Diffuse raised ICP 3. Ventriculomegaly (enlargement of the cerebral ventricles)
 A sixth principle: The separateness of the phenomenology of the following: 1. Focal mass effect 2. Diffuse raised ICP 3. Ventriculomegaly (enlargement of the cerebral ventricles).")
15
The pure form of raised ICP (without focal mass lesion, and without enlargement of the ventricular system) is a condition known as pseudotumor cerebri. The pure form of ventriculomegaly is a condition known as normal- pressure hydrocephalus (NPH).
..")
16
Question: What is intracranial hypertension? Question: What is intracranial hypertension? Cranial cavity volume increase, ICP Increase above 2.0 kPa (200mmH2O), resulting in a series of corresponding syndrome.
, resulting in a series of corresponding syndrome..")
17
Causes of intracranial hypertension 1. the content of cranial cavity increase 2. mass effect 3. congential malformation

18
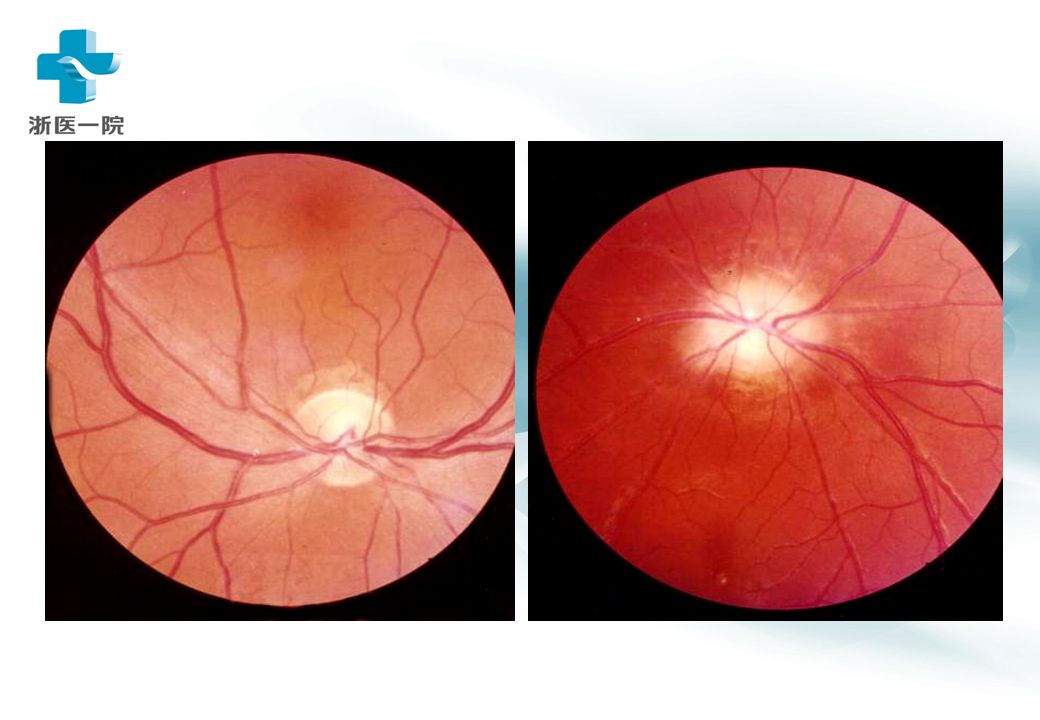
Clinical manifestations( 一) 1. 头痛 (headache ) : the most common symptom of intracranial hypertension. 2. 呕吐 (vomit ) : projectile vomiting 3. 视神经乳头水肿 (papilloedema) : Above three is the typical manifestations of intracranial hypertension. Clinical manifestations( 一) 1. 头痛 (headache ) : the most common symptom of intracranial hypertension. 2. 呕吐 (vomit ) : projectile vomiting 3. 视神经乳头水肿 (papilloedema) : Above three is the typical manifestations of intracranial hypertension.
 : the most common symptom of intracranial hypertension. 2. 呕吐 (vomit ) : projectile vomiting 3. 视神经乳头水肿 (papilloedema) : Above three is the typical manifestations of intracranial hypertension. Clinical manifestations( 一) 1. 头痛 (headache ) : the most common symptom of intracranial hypertension. 2. 呕吐 (vomit ) : projectile vomiting 3. 视神经乳头水肿 (papilloedema) : Above three is the typical manifestations of intracranial hypertension..")
20
Clinical manifestations ( 二) 4. disturbance of consciousness and changes of physical signs 5. others Clinical manifestations ( 二) 4. disturbance of consciousness and changes of physical signs 5. others
 4. disturbance of consciousness and changes of physical signs 5. others.")
21
The diseases caused intracranial hypertension 1. craniocerebral injury

22
Acute subdural hematoma

23
Subacute subdural hematoma

24
2. intracranial tumor :

25
3. intracranial infection : intracerebral abscess 、 tuberculous meningitis 、 tuberculoma of brain 。

26
intracerebral abscess 脑脓肿 CT 片 intracerebral abscess

27
Brain abscess

28
4. cerebrovascular disease : cerebral hemorrhage 、 subarachnoid hemorrhage 。

29
5. 脑寄生虫病 (cerebral parasitosis) : 6. 颅脑先天性疾病 (congenital disease of brain) : 7. 良性颅内压增高 (benign intracranial hypertension) : 8. 脑缺氧 (cerebral anoxia)
 : 8. 脑缺氧 (cerebral anoxia).")
30
Influence factors of intracranial hypertension 1. 年龄 ( Age ) : characteristics of Infants and the elderly
 : characteristics of Infants and the elderly.")
32
Influence factors of intracranial hypertension 2. 病变扩张的速度 ( Outstretched velocity of the disease ) :
 :.")
33
Influence factors of intracranial hypertension 3. 病变部位 ( Position of the disease ) : the midline, posterior fossa and filling sinus near lesions
 : the midline, posterior fossa and filling sinus near lesions.")
34
4. 伴发脑水肿的程度 ( Degree of hydrocephalus ): Lesions of the inflammatory response may be associated with obvious cerebral edema, such as cerebral abscess
: Lesions of the inflammatory response may be associated with obvious cerebral edema, such as cerebral abscess.")
35
Influence factors of intracranial hypertension 5. 全身情况 ( General conditions ) : Liver and kidney function obstacle, and pulmonary infection, acid-base imbalances the secondary brain edema
 : Liver and kidney function obstacle, and pulmonary infection, acid-base imbalances the secondary brain edema.")
36
Acute cerebral hernia Anatomical: the whole cranial cavity was separated into three each other mutually cavity by brain sickle and cerebellum tent. The cavity above the cerebellum tent were divided into control two cavity, respectively hold about cerebral hemisphere, The cavity under the tent accommodate cerebellum, bridge brain and the medulla oblongata.

37
The causes of the formation of cerebral hernia When a certain cavity has the intracranial lesions, this cavity pressure is greater than adjacent cavity pressure, and brain from high to low pressure area shift and lead to brain tissue, vascular and cranial nerves, and other important structure compression and shift, resulting in a series of serious clinical symptoms and signs, called "the cerebral hernia".

38
Brain herniation Brain herniation 1.infrafalx cerebri herniation 2.transtentorial herniation 3.Foramen magnum herniation

39
Management of cerebral hernia Principle of management 1.Rapid intravenous input permeability liquid, reduce intracranial pressure to alleviate temporarily condition. Commonly used medicines for mannitol 125 ~ 20% 250ml rapid static drops. 2.Early clear lesions properties and parts, seasonable purify for. 3.Causes difficult to express or lack of effective healer, can choose some palliative operation to alleviate increase intracranial pressure. Such as hydrocephalus can choose ventricle external drainage, cerebrospinal fluid diversion decompression, The cerebellum curtain cut trace hernia feasible temporal component decompression, Foramen magnum hernia feasible suboccipital decompression.

40
Summary 1 、 Summary 1 、 the content of the cranial cavity 2 、 ICP,ICP value 3 、 the vicious cycle of ICP and CPP 4 、 the relation between CBF 、 CPP and CVR 5 、 the relation between CPP 、 ICP and MAP 6 、 Intracranial hypertension 7 、 Clinical manifestations of Intracranial hypertension 8 、 pseudotumor cerebri 9 、 brain herniation

Similar presentations