Download presentation
Presentation is loading. Please wait.

1
Pharmacology RHPT-365 Chapter 4: CardioVascular Pharmacology
By Majid Ahmad Ganaie M. Pharm., Ph.D. Assistant Professor Department of Pharmacology E mail:

2
Heart & Blood Circulation
Blood leaves each of the ventricles via a single artery, the pulmonary trunk from the right ventricle, and the aorta from the left ventricle. Blood enters the right atrium via two large veins, the superior vena cava and inferior vena cava; it enters the left atrium via four pulmonary veins.

3
Path of blood flow through the entire cardiovascular system

4
Drugs Acting on the Cardiovascular System
Anti-hypertensive drugs for treatment of hypertension (high blood pressure) Anti-arrhythmic drugs for treatment of arrhythmia Anti-anginal drugs for treatment of angina Cardiotonic drugs (e.g., digoxin) for treatment of heart failure
 Anti-arrhythmic drugs for treatment of arrhythmia. Anti-anginal drugs for treatment of angina. Cardiotonic drugs (e.g., digoxin) for treatment of heart failure.")
5
Antihypertensive drugs, Hypertension - Introduction
Hypertension is a condition that afflicts almost 1 billion people worldwide and is a leading cause of morbidity and mortality. More than 20% of Americans are hypertensive, and one-third of these Americans are not even aware they are hypertensive. Therefore, this disease is sometimes called the "silent killer" SBP: systolic blood pressure DBP: diastolic blood pressure When the left ventricle ejects blood into the aorta, the aortic pressure rises. The maximal aortic pressure following ejection is termed the systolic blood pressure (SBP) As the left ventricle is relaxing and refilling, the pressure in the aorta falls. The lowest pressure in the aorta, which occurs just before the ventricle ejects blood into the aorta, is termed the diastolic blood pressure (DBP) Hypertension may defined as an abnormal elevation of either SBP or DBP *Arterial pressures less than 90/60 mmHg are considered hypotension, and therefore not normal Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident
 As the left ventricle is relaxing and refilling, the pressure in the aorta falls. The lowest pressure in the aorta, which occurs just before the ventricle ejects blood into the aorta, is termed the diastolic blood pressure (DBP) Hypertension may defined as an abnormal elevation of either SBP or DBP. *Arterial pressures less than 90/60 mmHg are considered hypotension, and therefore not normal. Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident.")
6
Antihypertensive drugs, Hypertension - Introduction
Causes of Hypertension: The are two basic types of hypertension: Primary (essential) hypertension: The majority of patients (90-95%) have essential hypertension, which is a form with no identifiable underlying cause. This form of hypertension is commonly treated with drugs in addition to lifestyle changes (e.g., exercise, proper nutrition, weight reduction, stress reduction). Secondary hypertension: A smaller number of patients (5-10%) have secondary hypertension that is caused by an identifiable underlying condition such as renal artery disease, thyroid disease, primary hyperaldosteronism, pregnancy, etc. Patients with secondary hypertension are best treated by controlling or removing the underlying disease or pathology, although they may still require antihypertensive drugs Some causes of secondary hypertension: Renal artery stenosis Chronic renal disease Primary hyperaldosteronism Stress Hyper- or hypothyroidism Pheochromocytoma Pre-eclampsia Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident
 hypertension: The majority of patients (90-95%) have essential hypertension, which is a form with no identifiable underlying cause. This form of hypertension is commonly treated with drugs in addition to lifestyle changes (e.g., exercise, proper nutrition, weight reduction, stress reduction). Secondary hypertension: A smaller number of patients (5-10%) have secondary hypertension that is caused by an identifiable underlying condition such as renal artery disease, thyroid disease, primary hyperaldosteronism, pregnancy, etc. Patients with secondary hypertension are best treated by controlling or removing the underlying disease or pathology, although they may still require antihypertensive drugs. Some causes of secondary hypertension: Renal artery stenosis. Chronic renal disease. Primary hyperaldosteronism. Stress. Hyper- or hypothyroidism. Pheochromocytoma. Pre-eclampsia. Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident.")
7
Cardiac Output X Peripheral Resistance
Antihypertensive drugs, Introduction Blood Pressure = Cardiac Output X Peripheral Resistance Each time the heart beats, a volume of blood (stroke volume “SV”) is ejected. This stroke volume (SV), times the number of beats per minute (heart rate “HR”), equals the cardiac output (CO); i.e., CO = SV x HR Thus cardiac output is the volume of blood being pumped by the heart, in particular by a ventricle in a minute. Stroke volume is expressed in ml/beat and heart rate in beats/minute. Therefore, cardiac output is in ml/minute Peripheral resistance (PR) refers to the resistance to blood flow offered by all of the systemic vasculature, excluding the pulmonary vasculature. Mechanisms that cause vasoconstriction increase PR, and those mechanisms that cause vasodilatation decrease PR. Therefore, patients with primary hypertension are generally treated with drugs that: reduce blood volume (which reduces central venous pressure and cardiac output) reduce peripheral resistance, or reduce cardiac output by depressing heart rate and stroke volume Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident
 is ejected. This stroke volume (SV), times the number of beats per minute (heart rate HR ), equals the cardiac output (CO); i.e., CO = SV x HR. Thus cardiac output is the volume of blood being pumped by the heart, in particular by a ventricle in a minute. Stroke volume is expressed in ml/beat and heart rate in beats/minute. Therefore, cardiac output is in ml/minute. Peripheral resistance (PR) refers to the resistance to blood flow offered by all of the systemic vasculature, excluding the pulmonary vasculature. Mechanisms that cause vasoconstriction increase PR, and those mechanisms that cause vasodilatation decrease PR. Therefore, patients with primary hypertension are generally treated with drugs that: reduce blood volume (which reduces central venous pressure and cardiac output) reduce peripheral resistance, or. reduce cardiac output by depressing heart rate and stroke volume. Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident.")
8
Antihypertensive drugs, Classes, the most important ones
Diuretics Angiotensin Converting Enzyme Inhibitors (ACE inhibitors) Angiotensin Receptor blockers Renin Inhibitors Calcium Channel Blockers Potassium Channel openers a1-adrenoceptor antagonists (a1-blockers) Beta Blockers a2-adrenoceptor agonists Peripheral Vasodilators Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident
 Angiotensin Receptor blockers. Renin Inhibitors. Calcium Channel Blockers. Potassium Channel openers. a1-adrenoceptor antagonists (a1-blockers) Beta Blockers. a2-adrenoceptor agonists. Peripheral Vasodilators. Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident.")
9
Antihypertensive drugs, Classes, the most important ones
Diuretics: Mechanism of action. Diuretics act on the kidney to enhance sodium and water excretion urine output by the kidney (i.e., promote diuresis) blood volume Reducing blood volume not only reduces central venous pressure, but even more importantly, reduces cardiac output Examples: chlorothiazide, furosemide, amiloride ACE inhibitors Mechanism of action. Dilate arteries and veins by blocking formation of angiotensin II (AII, a vasoconstrictor) vasodilatation, thus reduces arterial pressure, preload and afterload on the heart Promote renal excretion of sodium and water. This reduces blood volume, venous pressure and arterial pressure Examples: captopril, enalapril This is accomplished by altering how the kidney handles sodium. If the kidney excretes more sodium, then water excretion will also increase. Most diuretics produce diuresis by inhibiting the re-absorption of sodium at different segments of the renal tubular system.
 blood volume. Reducing blood volume not only reduces central venous pressure, but even more importantly, reduces cardiac output. Examples: chlorothiazide, furosemide, amiloride. ACE inhibitors. Mechanism of action. Dilate arteries and veins by blocking formation of angiotensin II (AII, a vasoconstrictor) vasodilatation, thus reduces arterial pressure, preload and afterload on the heart. Promote renal excretion of sodium and water. This reduces blood volume, venous pressure and arterial pressure. Examples: captopril, enalapril. This is accomplished by altering how the kidney handles sodium. If the kidney excretes more sodium, then water excretion will also increase. Most diuretics produce diuresis by inhibiting the re-absorption of sodium at different segments of the renal tubular system.")
10
Antihypertensive drugs, Classes, the most important ones
Angiotensin Receptor blockers (ARBs) Mechanism of action: ARBs are receptor antagonists that block type 1 angiotensin II receptors on bloods vessels and other tissues such as the heart These drugs have similar effects to ACE inhibitors and are used for the same indications (hypertension, heart failure) Examples: losartan, valsartan Renin Inhibitors Mechanism of action: Renin inhibitors produce vasodilation by inhibiting the activity of renin, which is responsible for stimulating angiotensin II formation These drugs have similar effects to ACE inhibitors and ARBs and are used for the same indications (hypertension, heart failure) Example: aliskiren This is accomplished by altering how the kidney handles sodium. If the kidney excretes more sodium, then water excretion will also increase. Most diuretics produce diuresis by inhibiting the re-absorption of sodium at different segments of the renal tubular system.
 Mechanism of action: ARBs are receptor antagonists that block type 1 angiotensin II receptors on bloods vessels and other tissues such as the heart. These drugs have similar effects to ACE inhibitors and are used for the same indications (hypertension, heart failure) Examples: losartan, valsartan. Renin Inhibitors. Mechanism of action: Renin inhibitors produce vasodilation by inhibiting the activity of renin, which is responsible for stimulating angiotensin II formation. These drugs have similar effects to ACE inhibitors and ARBs and are used for the same indications (hypertension, heart failure) Example: aliskiren. This is accomplished by altering how the kidney handles sodium. If the kidney excretes more sodium, then water excretion will also increase. Most diuretics produce diuresis by inhibiting the re-absorption of sodium at different segments of the renal tubular system.")
11
Membrane Potential An electrical potential difference, or membrane potential, can be recorded across the plasma membrane of living cells The potential of unstimulated muscle and nerve cells, or resting potential, amounts to – 50 to – 100mV (cell interior is negative) A resting potential is caused by a slightly unbalanced distribution of ions between the intracellular fluid and extracellular fluid anionic proteins and phosphates present in high concentrations in the cytosol are virtually unable to leave the cell All living cells have a (resting) membrane potential, but only excitable cells such as nerve and muscle cells are able to greatly change the ion conductance of their membrane in response to a stimulus, as in an action potential
 A resting potential is caused by a slightly unbalanced distribution of ions between the intracellular fluid and extracellular fluid. anionic proteins and phosphates present in high concentrations in the cytosol are virtually unable to leave the cell. All living cells have a (resting) membrane potential, but only excitable cells such as nerve and muscle cells are able to greatly change the ion conductance of their membrane in response to a stimulus, as in an action potential.")
12
Action Potential Definition: an action potential (also known as a nerve impulse) is a pulse-like wave of voltage that passes on through an axon or along a muscle fiber that influences other neurons or induces muscle contraction During depolarization: Opening of sodium channels and influx of sodium ions is usually associated with cell stimulation During repolarization: Inactivation of sodium channels and repolarizing efflux of potassium ions is usually associated with cell inhibition Depolarization Repolarization The normal ratio of ion concentrations across the membrane is maintained by the continual action of the sodium–potassium pump, which transports three sodium ions out of the cell and two potassium ions in Cathode Ray Oscilloscope (CRO) The few ions that do cross are pumped out again by the continual action of the sodium–potassium pump, which, with other ion transporters, maintains the normal ratio of ion concentrations across the membrane The action potential stops at the end of the neuron, but usually causes the secretion of neurotransmitters at the synapses that are found there These neurotransmitters bind to receptors on adjacent cells
 is a pulse-like wave of voltage that passes on through an axon or along a muscle fiber that influences other neurons or induces muscle contraction. During depolarization: Opening of sodium channels and influx of sodium ions is usually associated with cell stimulation. During repolarization: Inactivation of sodium channels and repolarizing efflux of potassium ions is usually associated with cell inhibition. Depolarization. Repolarization. The normal ratio of ion concentrations across the membrane is maintained by the continual action of the sodium–potassium pump, which transports three sodium ions out of the cell and two potassium ions in. Cathode Ray Oscilloscope (CRO) The few ions that do cross are pumped out again by the continual action of the sodium–potassium pump, which, with other ion transporters, maintains the normal ratio of ion concentrations across the membrane. The action potential stops at the end of the neuron, but usually causes the secretion of neurotransmitters at the synapses that are found there. These neurotransmitters bind to receptors on adjacent cells.")
13
Cardiac Action Potential
The cardiac action potential differs from the neuronal action potential by having an extended plateau, in which the membrane is held at a high voltage for a few hundred milliseconds prior to being repolarized by the potassium current as usual This plateau is due to the action of slower Ca2+ channels opening even after the Na2+ channels have inactivated The cardiac action potential plays an important role in coordinating the contraction of the heart The cardiac cells of the sinoatrial node provide the pacemaker potential that synchronizes the heart The action potentials of those cells propagate to and through the atrioventricular node (AV node), then from the AV node travel through the bundle of His and thence to the Purkinje fibers. Phases of a cardiac action potential The sharp rise in voltage ("0") corresponds to the influx of sodium ions, whereas the two decays ("1" and "3", respectively) correspond to the sodium-channel inactivation and the repolarizing efflux of potassium ions The characteristic plateau ("2") results from the opening of voltage-sensitive calcium channels Action potentials in cardiac muscle are of much longer duration than those in skeletal muscle (!p. 59 A) because gK temporarily decreases and gCa increases for 200 to 500ms after rapid inactivation of Na+ channels. This allows the slow influx of Ca2+, causing the action potential to reach a plateau. As a result, the refractory period does not end until a contraction has almost subsided (!p. 59 A). Therefore, tetanus cannot be evoked in cardiac muscle. This plateau is due to the action of slower Ca2+ channels opening and holding the membrane voltage near their equilibrium potential even after the Na2+ channels have inactivated منظم القلب Pacemaker:
, then from the AV node travel through the bundle of His and thence to the Purkinje fibers. Phases of a cardiac action potential. The sharp rise in voltage ( 0 ) corresponds to the influx of sodium ions, whereas the two decays ( 1 and 3 , respectively) correspond to the sodium-channel inactivation and the repolarizing efflux of potassium ions. The characteristic plateau ( 2 ) results from the opening of voltage-sensitive calcium channels. Action potentials in cardiac muscle are of much longer duration than those in skeletal muscle (!p. 59 A) because gK temporarily. decreases and gCa increases for 200 to 500ms after rapid inactivation of Na+ channels. This allows the slow influx of Ca2+, causing the action potential to reach a plateau. As a result, the refractory period does not end until a contraction has almost subsided (!p. 59 A). Therefore, tetanus cannot be evoked in cardiac muscle. This plateau is due to the action of slower Ca2+ channels opening and holding the membrane voltage near their equilibrium potential even after the Na2+ channels have inactivated. منظم القلب Pacemaker:")
14
Cardiac Action Potential
The cardiac action potential differs from the neuronal action potential by having an extended plateau, in which the membrane is held at a high voltage for a few hundred milliseconds prior to being repolarized by the potassium current as usual This plateau is due to the action of slower Ca2+ channels opening even after the Na2+ channels have inactivated The cardiac action potential plays an important role in coordinating the contraction of the heart The cardiac cells of the sinoatrial node provide the pacemaker potential that synchronizes the heart The action potentials of those cells propagate to and through the atrioventricular node (AV node), then from the AV node travel through the bundle of His and thence to the Purkinje fibers Cardiac Cycle The resting heart rate is 60–80 beats per minute. A cardiac cycle (!A) therefore takes roughly 1 s. It can be divided into four distinct phases: (I) contraction phase and (II) ejection phase, both occurring in systole; (III) relaxation phase and filling phase (IV), both occurring in diastole. At the end of phase IV, the atria contract (phase IVc). Electrical excitation of the atria and ventricles precedes their contraction.
, then from the AV node travel through the bundle of His and thence to the Purkinje fibers. Cardiac Cycle. The resting heart rate is 60–80 beats per minute. A cardiac cycle (!A) therefore takes roughly 1 s. It can be divided into four distinct. phases: (I) contraction phase and (II) ejection phase, both occurring in systole; (III) relaxation phase and filling phase (IV), both occurring in. diastole. At the end of phase IV, the atria contract (phase IVc). Electrical excitation of the atria and ventricles precedes their contraction.")
15
Antihypertensive drugs, Classes, the most important ones
Diuretics Angiotensin Converting Enzyme Inhibitors (ACE inhibitors) Angiotensin Receptor blockers Renin Inhibitors Calcium Channel Blockers Potassium Channel openers a1-adrenoceptor antagonists (a1-blockers) Beta Blockers a2-adrenoceptor agonists Peripheral Vasodilators Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident
 Angiotensin Receptor blockers. Renin Inhibitors. Calcium Channel Blockers. Potassium Channel openers. a1-adrenoceptor antagonists (a1-blockers) Beta Blockers. a2-adrenoceptor agonists. Peripheral Vasodilators. Stroke: sudden diminution or loss of consciousness, sensation, and voluntary motion caused by rupture or obstruction (as by a clot) of a blood vessel of the brain —called also apoplexy, brain attack, cerebrovascular accident.")
16
Antihypertensive drugs, Classes, the most important ones
Calcium Channel Blockers (CCBs): Mechanism of action. These drugs bind to calcium channels located on the vascular smooth muscle, cardiac myocytes, and cardiac nodal tissue (sinoatrial and atrioventricular nodes). These channels are responsible for regulating the influx of calcium into muscle cells, which in turn stimulates smooth muscle contraction and cardiac myocyte contraction. In cardiac nodal tissue, calcium channels play an important role in pacemaker currents and in phase 0 of the action potentials. Therefore, by blocking calcium entry into the cell, CCBs cause vascular smooth muscle relaxation (vasodilation), decreased myocardial force generation, decreased heart rate, and decreased conduction velocity within the heart, particularly at the atrioventricular node. Examples: nifedipine, verapamil Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from opening
: Mechanism of action. These drugs bind to calcium channels located on the vascular smooth muscle, cardiac myocytes, and cardiac nodal tissue (sinoatrial and atrioventricular nodes). These channels are responsible for regulating the influx of calcium into muscle cells, which in turn stimulates smooth muscle contraction and cardiac myocyte contraction. In cardiac nodal tissue, calcium channels play an important role in pacemaker currents and in phase 0 of the action potentials. Therefore, by blocking calcium entry into the cell, CCBs cause vascular smooth muscle relaxation (vasodilation), decreased myocardial force generation, decreased heart rate, and decreased conduction velocity within the heart, particularly at the atrioventricular node. Examples: nifedipine, verapamil. Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation. This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from. opening.")
17
Antihypertensive drugs, Classes, the most important ones
Potassium Channel openers: Mechanism of action. These are drugs that activate (open) ATP-sensitive K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium, leadings to muscle relaxation and vasodilation, decreasing systemic vascular resistance and lowering blood pressure. Examples: Nicorandil, minoxidil sulphate a1-adrenoceptor antagonists (a1-blockers) Mechanism of action. These drugs block the effect of sympathetic nerves on blood vessels by binding to a-adrenoceptors located on the vascular smooth muscle. Most of these drugs acts as competitive antagonists to the binding of norepinephrine to the smooth muscle receptors a--blockers dilate both arteries and veins because both vessel types are innervated by sympathetic adrenergic nerves; however, the vasodilator effect is more pronounced in the arterial resistance vessels. Thus they decrease systemic vascular resistance and lower blood pressure. Examples: prazosin, doxazosin Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from opening
 ATP-sensitive K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium, leadings to muscle relaxation and vasodilation, decreasing systemic vascular resistance and lowering blood pressure. Examples: Nicorandil, minoxidil sulphate. a1-adrenoceptor antagonists (a1-blockers) Mechanism of action. These drugs block the effect of sympathetic nerves on blood vessels by binding to a-adrenoceptors located on the vascular smooth muscle. Most of these drugs acts as competitive antagonists to the binding of norepinephrine to the smooth muscle receptors. a--blockers dilate both arteries and veins because both vessel types are innervated by sympathetic adrenergic nerves; however, the vasodilator effect is more pronounced in the arterial resistance vessels. Thus they decrease systemic vascular resistance and lower blood pressure. Examples: prazosin, doxazosin. Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation. This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from. opening.")
18
Antihypertensive drugs, Classes, the most important ones
b-blockers : Mechanism of action. Beta-blockers are drugs that bind to b-adrenoceptors and thereby block the binding of norepinephrine and epinephrine to these receptors. This inhibits normal sympathetic effects that act through these receptors. Thus, drugs decrease heart rate, conduction velocity and force of contraction The first generation of b-blockers were non-selective, meaning that they blocked both b1 and b2 adrenoceptors. Second generation b-blockers (b1-blockers) are more cardioselective in that they are relatively selective for b1 adrenoceptors. Examples: For non-selective b blockers: propranolol For selective b1 blockers: atenolol a2-adrenoceptor agonists (centrally acting sympatholytics) Mechanism of action. Centrally acting sympatholytics block sympathetic activity by binding to and activating a2-adrenoceptors inhibition of NE release. This reduces sympathetic outflow to the heart thereby decreasing cardiac output by decreasing heart rate and contractility Reduced sympathetic output to the blood vessels decreases sympathetic vascular tone, which causes vasodilation and reduced systemic vascular resistance, which decreases arterial pressure Examples: clonidine Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from opening
 are more cardioselective in that they are relatively selective for b1 adrenoceptors. Examples: For non-selective b blockers: propranolol. For selective b1 blockers: atenolol. a2-adrenoceptor agonists (centrally acting sympatholytics) Mechanism of action. Centrally acting sympatholytics block sympathetic activity by binding to and activating a2-adrenoceptors inhibition of NE release. This reduces sympathetic outflow to the heart thereby decreasing cardiac output by decreasing heart rate and contractility. Reduced sympathetic output to the blood vessels decreases sympathetic vascular tone, which causes vasodilation and reduced systemic vascular resistance, which decreases arterial pressure. Examples: clonidine. Mechanism of action. Potassium-channel openers are drugs that activate (open) K+-channels in vascular smooth muscle. Opening these channels hyperpolarizes the smooth muscle, which closes voltage-gated calcium channels and decreases intracellular calcium. With less calcium available to combine with calmodulin, there is less activation of myosin light chain kinase and phosphorylation of myosin light chains. This leads to relaxation and vasodilation. This promotes K+ efflux and the cell hyperpolarizes, thereby preventing voltage-operated Ca2+ channels (VOCs) from. opening.")
19
Anti-arrhythmic drugs
Generation & propagation of normal cardiac impulse 1 SA node 2 AV node Bundle of Hiss 3 Right & left bundle branch 4 Purkinje system Na Ca Na Na K K K Ca Mechanisms of cardiac arrhythmias: Abnormal impulse formation: From SA node or abnormal pacemaker Abnormal impulse conduction: AV node, purkinje system or myocardium

20
Clinical aspects of cardiac arrhythmias
Incidence: 10 % patients in hospital have abnormal cardiac rhythm Causes: CVS or other diseases, drugs, electrolyte changes Types: Ectopic beats: atrial, AV-nodal or ventricular Bradycardias: Sinus bradycardia, heart block (AV block) Tachycardias: Sinus tachycardia Atrial tachycardia, flutter & fibrillation Ventricular tachycardia, flutter & fibrillation Effects: cardiac output & tissue blood perfusion
 Tachycardias: Sinus tachycardia. Atrial tachycardia, flutter & fibrillation. Ventricular tachycardia, flutter & fibrillation. Effects: cardiac output & tissue blood perfusion.")
21
Anti-arrhythmic drugs (Cont.)
Class I: Sodium Channel blockers Further sub-divided into IA, IB & IC Class II: Beta Blockers Class III: Potassium Channel Blockers Class IV: Calcium Channel Blockers Class V: Miscellaneous

22
Class IA (Quinidine, procainamide)
Mechanism of action: Block Na-channel in SA node & ventricles ↓ rate of rise of phase 0 in pacemaker cells ↑ effective refractory period (ERP) & QT interval Prolong repolarization due to ↓ in K eflux Prolonged repolarization Slow rise of phase 0
 & QT interval. Prolong repolarization due to ↓ in K eflux. Prolonged. repolarization. Slow rise. of phase 0.")
23
Quinidine (Cont.) Other actions:
Anti-cholinergic (vagolytic effect), ↑ AV-conduction This increases ventricular rate in atrial flutter Propranolol or verapamil is added to reduce this effect Uses: Supra-ventricular & ventricular tachycardia (given oral & IV) Adverse effects: CVS: Bradycardia & cardiac depression Quinidine syncope (a-blocking effect) Thrombocytopenia (immune reaction) GI: nausea, vomiting & diarrhea Cinchonism: tinnitis, vertigo & headache Drug interaction: ↑ toxicity of digoxin, due to ↓ renal excretion
, ↑ AV-conduction. This increases ventricular rate in atrial flutter. Propranolol or verapamil is added to reduce this effect. Uses: Supra-ventricular & ventricular tachycardia (given oral & IV) Adverse effects: CVS: Bradycardia & cardiac depression. Quinidine syncope (a-blocking effect) Thrombocytopenia (immune reaction) GI: nausea, vomiting & diarrhea. Cinchonism: tinnitis, vertigo & headache. Drug interaction: ↑ toxicity of digoxin, due to ↓ renal excretion.")
24
Procainamide (Cont.) Use:
ventricular arrhythmia after MI (given oral & IV) Adverse effects: Hypotension reversible systemic lupus erythematosis (SLE) like effects: skin rash, arthritis, pleuritis & pericarditis
 Adverse effects: Hypotension. reversible systemic lupus erythematosis (SLE) like effects: skin rash, arthritis, pleuritis & pericarditis.")
25
Class IB (lidocaine & phenytoin)
Mechanism of action: Block Na-channel, particularly in ischemic myocardium less effect on rate of rise of phase 0 ↓ effective refratory period (ERP) & QT interval Less effect on phase 0 Shortened repolarization
 & QT interval. Less effect. on phase 0. Shortened. repolarization.")
26
Lidocaine (Cont.) Other properties:
Short half-life (20 minutes) given by IV infusion Metabolized in liver (↑ toxicity with enzyme inhibitors) Use: Ventricular tachycardia in ischemic heart disease (MI) Also used as local anesthetic (also named lignocaine) Adverse effects: Less cardiac depression Confusion, dizziness, slurred speech & seizures
 given by IV infusion. Metabolized in liver (↑ toxicity with enzyme inhibitors) Use: Ventricular tachycardia in ischemic heart disease (MI) Also used as local anesthetic (also named lignocaine) Adverse effects: Less cardiac depression. Confusion, dizziness, slurred speech & seizures.")
27
Class IC (flecainide & propafenone)
Mechanism of action: Block Na-channel, in SA node & ventricles Marked ↓ of rate of rise of phase 0 of action potential No effect on effective refractory period (ERP) & QT Minimal effect on the duration of action potenial Marked effect on phase 0 Minimal effect on repolarization
 & QT. Minimal effect on the duration of action potenial. Marked effect. on phase 0. Minimal effect. on repolarization.")
28
Flecainide (Cont.) Uses: Paroxysmal supra-ventricular tachycardia
Premature ventricular contractions Ventricular tachycardia Reserved for resistant cases (because of chances of cardiac depression) Adverse effect: Cardiac depression, prolonged PR & QRS interval Nausea, dizziness & blurred vision
 Adverse effect: Cardiac depression, prolonged PR & QRS interval. Nausea, dizziness & blurred vision.")
29
Class II (β-blockers-Propranolol & esmolol)
Mechanism of action: Competitively block β receptors & inhibit the effect of catecholamines on cardiac β receptors Propranolol also ↓ Na-channel like class I drugs Decreased slope of phase 4 in SA node Prolonged repolarization at AV node Decreased slope of phase 4 in SA node Prolonged repolarization at AV node

30
Propranolol & esmolol (Cont.)
Uses: Supraventricular tachycardia to control ventricular rate Adverse effects: Bradycardia, hypotension, broncho-constriction, muscle pain, fatigue & hypoglycemia, nightmares & depression Esmolol: Very short acting, given IV in ventricular arrhythmias during surgery

31
Class III (Amiodarone & sotalol)
Mechanism of action (amiodarone): Block K-channels ( also blocks Na-channels) Prolong re-polarization & action potential Prolong effective refratory period (ERP) Also possess some β adrenergic & Ca-channel blocking effects Prolonged repolarization
: Block K-channels ( also blocks Na-channels) Prolong re-polarization & action potential. Prolong effective refratory period (ERP) Also possess some β adrenergic & Ca-channel blocking effects. Prolonged. repolarization.")
32
Amiodarone (Cont.) Uses: Supra-ventricular & ventricular tachycardias
IV for acute episode & oral for chronic recurrent arrhythmias Adverse effects: May cause bradycardia, AV-block & hypotension Risk of induction of arrhythmias (torsade de pointes) Pulmonary fibrosis, hepatic damage, photodermatitis Blocks conversion of T4 to T3 (hypothyroidism)
 Pulmonary fibrosis, hepatic damage, photodermatitis. Blocks conversion of T4 to T3 (hypothyroidism)")
33
Class IV (Verapamil & diltiazem)
Mechanism of action: Block ‘L - type’ of Ca-channels in cardiac tissue ↓ inward Ca-current, in SA-node & AV-node ↓ conduction velocity & ↑ effective refractory period Prolonged repolarization Slow rise of phase 0

34
Verapamil & diltiazem (Cont.)
Use: Supra-ventricular tachycardia (to control ventricular rate) Also used in angina and hypertension Adverse effects: Bradycardia, hypotension, edema, constipation ↑ plasma digoxin levels by ↓ in renal excretion
 Also used in angina and hypertension. Adverse effects: Bradycardia, hypotension, edema, constipation. ↑ plasma digoxin levels by ↓ in renal excretion.")
35
Miscellaneous anti-arrhythmic drugs
Adenosine Mechanism of action: Stimulates P-1 purinergic receptors & opens K channels ↓ conduction at SA node, atria & AV node Also ↓ cAMP-induced Ca influx Use: Paroxysmal supra-ventricular tachycardia Rapid onset (few seconds) & short half life (10-20 seconds) Adverse effects: Sinus bradycardia & AV block, initial rise & then fall in BP Bronchoconstriction, headache, flushing & chest pain
 & short half life (10-20 seconds) Adverse effects: Sinus bradycardia & AV block, initial rise & then fall in BP. Bronchoconstriction, headache, flushing & chest pain.")
36
Miscellaneous anti-arrhythmic drugs (Cont.)
Potassium: Hypokalemia causes after depolarizations & ectopic beats Hyperkalemia causes slow conduction & cardiac arrest Correction of serum K levels controls these arrhythmias For hypokalemia: K supplements; oral or IV For hyperkalemia: Insulin with glucose & in severe cases hemodialysis Magnesium: Mg sulfate oral, IM or IV can be used for refractory ventricular tachycardia Digoxin: May be used in supraventricular tachycardia.

37
Ischemic Heart Disease
Angina pectoris Chronic condition, episodic chest discomfort Occurs during transient coronary ischemia Myocardial infarction Acute and complete occlusion of a coronary artery Due to coronary thrombosis 37

38
increased demand for oxygen evoked by physical exertions
Angina- episodic chest pains as a result of transient coronary ischemia (as opposed to myocardial infarction which is acute and complete occlusion of a coronary artery . angina (heavy weight or pressure or pain in the chest) occurs when blood (oxygen, nutrient) supply to the heart is limited as a result of : disruption of coronary blood flow because of vasospasm or platelet aggregation increased demand for oxygen evoked by physical exertions a combination of both 38
 occurs when blood (oxygen, nutrient) supply to the heart is limited as a result of : disruption of coronary blood flow because of vasospasm or platelet aggregation. increased demand for oxygen evoked by physical exertions. a combination of both. 38.")
39
ANGINA PECTORIS Angina pectoris develops as a result of an imbalance between the oxygen supply and the oxygen demand of the myocardium. It is a symptom of myocardial ischemia. When the increase in coronary blood flow is unable to match the increased oxygen demand, angina develops. It has become apparent that spasm of the coronary arteries is important in the production of angina. 39

40
Vasospasm at rest or during sleep
If the frequency and severity increases- forerunner to a MI If symptoms remains the same and angina occurs under similar circumstances 40

41
Drugs used in Angina pectoris:
Organic nitrates e.g. Nitro-glycerine, isosorbide Dinitrate, etc. Beta adrenergic blocking agents e.g. Propranolol, Atenolol, etc. Calcium channel blocking agents e.g. Verapamil, nifedipine, etc. Miscellaneous drugs e.g. Aspirin, Heparin, Dipyridamole. 41

42
Drugs employed: Antianginal drugs : Typical Variant MI
Stable Unstable Organic nitrite and nitrates Ca2+-channel blockers to - adrenergic Antagonists Aspirin Fibrinolytic drugs Antianginal drugs : -O2 increase supply and/or lower demand Myocardial O2 supply: Coronary blood flow, regional flow distribution Myocarial O2 –demand: amount of energy required to support the work of the heart Cardiac work influenced by: heart rate, heart contractility, myocardial wall tension 42

43
Mechanism of Action: 43

44
Vasodilators- organic compounds containing ONO or ONO2 (prodrugs) all release NO upon interacting with serum components. these are converted intracellularly to nitrite ions and then No (Nitric oxide) which in turn activate guanylate cyclase that lead to increase the cyclic GMP and to dephosphorylation of the myosin light chain which result in relaxation of vascular smooth muscle.
 which in turn activate guanylate cyclase that lead to increase the cyclic GMP and to dephosphorylation of the myosin light chain which result in relaxation of vascular smooth muscle.")
45
HEART FAILURE Congestive heart failure occurs when there is an inability of the heart to maintain a cardiac out put sufficient to meet the requirements of the metabolising tissues. Heart failure is usually caused by one of the following: Ischaemic heart disease, Hypertension, Heart muscle disorders, and Valvular heart disease. Drug management aims to provide symptomatic relief for the patient while also preventing further deterioration in cardiac function 45

46
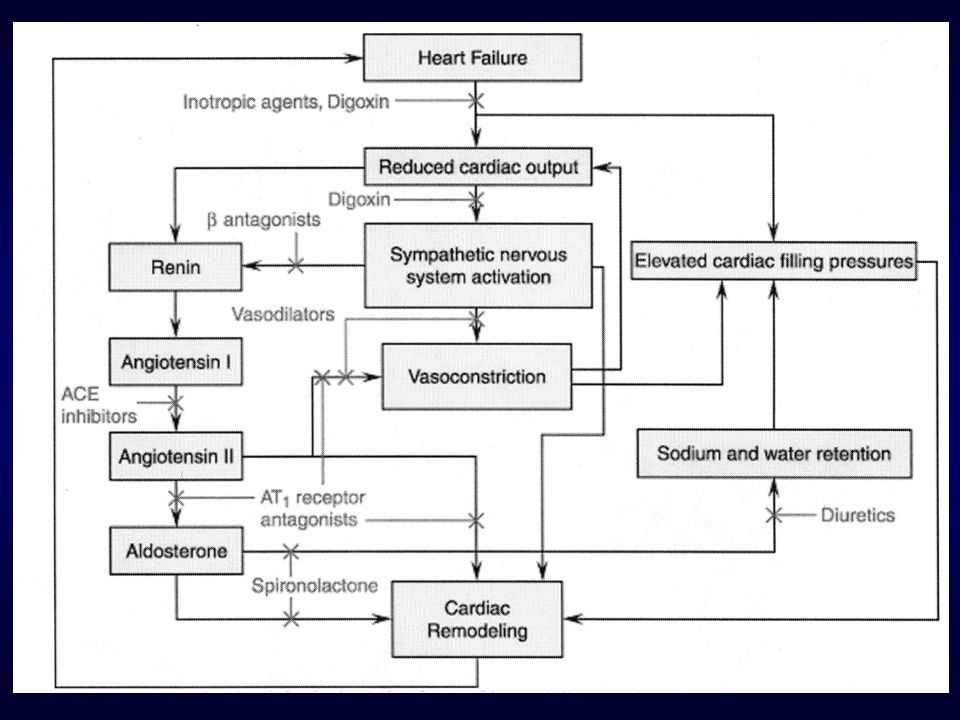
The Vicious Cycle of Heart Failure
CARDIAC INJURY Pump failure Vasoconstriction Na+ H2O retention Neurohormonal Activation Renin Angiotensin, Aldosterone system Sympathetic Nervous system Others e.g. Natriuetic peptides

47
Background of Heart Failure:
Normal cardiac output needed to adequately perfuse peripheral organs Provide O2, nutrients, etc Remove CO2, metabolic wastes, etc Maintain fluid flow from capillaries into interstitium and back into venous system if flow reduced or pressure increased in venous system build up of interstitial fluid = edema Because CO is a function of Heart Rate – determined by pacemaker cells in the sinoatrial node Stroke volume – determined by fill rate and contractile force Atrial/ventricular/valvular coordination Any negative change on above can lead to inadequate perfusion and development of the syndrome of heart failure 47

48
Drugs used to treat Heart Failure:
A. Drugs with positive inotropic effect:- Drugs with positive inotropic effect increase the force of contraction of the heart muscle. These include: Cardiac glycosides, e.g. digoxin and digitoxin Bipyridine derivatives e.g. amrinone, milrinone. Sympathomimetics e.g. dobutamine, dopamine Methylxanthines e.g. aminophylline B. Drugs without positive inotropic effect. These include: Diuretics, e.g. hydrochlorothiazide, furosemide Vasodilators, e.g. hydralazine, sodium nitroprusside Angiotensin converting enzyme inhibitors e.g. captopril, enalapril 48

50
Digoxin: Mechanism of Action
Na-K ATPase Na-Ca Exchange Na+ K+ Na+ Ca++ Myofilaments K+ Na+ Ca++ Contractility Digoxin: Mechanism of Action Digoxin inhibits the Na+/K+ ATPase, which causes an increase in intracellular sodium concentration. This leads to accumulation of intracellular calcium in the heart via Na+/Ca++ exchange. Increased intracellular calcium promotes calcium release by the sarcoplasmic reticulum. Increased calcium binds troponin-C, leading to increased contractility. Digoxin also increases vagal activity to the heart, resulting in reduced chronotropy (heart rate) and dromotropy (conduction velocity).
 and dromotropy (conduction velocity).")
51
THANK YOU Any Questions?

Similar presentations





 Drug Therapy (Antihypertensives) ACEi B.B CCB D iuretics. Centrally acting agents: alphametyldopa, HTN + pregnancy.>")



. CARDIOVASCULAR DISEASE AND DRUGS ► Basic cardiovascular physiology and pathology depends on the control of heart.>")









