Download presentation
Presentation is loading. Please wait.

1
Control of Cardiovascular Function, Disorders of Blood Flow and Blood Pressure, Hyperlipidemia, and Artherosclerosis 1

2
INTRODUCTION 2

3
Sympathetic Nervous System 3

4
4 LocationResponse to agonist or neurotransmitter Alpha-1 – activated with norepi Arteries and veinsConstriction Bladder neck (internal sphincter)Constriction Alpha-2 – activated with norepi Central nervous systemInhibits sympathetic outflow Beta-1 – activated with norepi Heart, SA nodeIncreases heart rate (positive chronotropic effect) Heart, AV nodeIncreases speed of conduction (positive dromotropic effect) Heart, ventricular muscleIncreased contractility (positive inotropic effect) KidneyRelease of renin - Leads to thicker blood and vasoconstriction (through angiotensin II) - ultimately leads to increased blood pressure - do not need to pee Beta-2 – activated with only epi Arterioles in skeletal muscle bedsDilation to bring more blood to muscles BronchiDilation UterusRelaxation
Constriction Alpha-2 – activated with norepi Central nervous systemInhibits sympathetic outflow Beta-1 – activated with norepi Heart, SA nodeIncreases heart rate (positive chronotropic effect) Heart, AV nodeIncreases speed of conduction (positive dromotropic effect) Heart, ventricular muscleIncreased contractility (positive inotropic effect) KidneyRelease of renin - Leads to thicker blood and vasoconstriction (through angiotensin II) - ultimately leads to increased blood pressure - do not need to pee Beta-2 – activated with only epi Arterioles in skeletal muscle bedsDilation to bring more blood to muscles BronchiDilation UterusRelaxation")
5
Alpha-1 Receptors 5

6
Norepinephrine and epinephrine Vasoconstriction of arterioles and veins Vasoconstriction of the bladder – Prevents urination 6

7
Alpha-2 Receptors 7

8
Norepinephrine and epinephrine Inhibits sympathetic outflow 8

9
Beta-1 Receptors 9

10
Norepinephrine and epinephrine Increases heart rate Increases speed of conduction Increases heart contractility Activates the RAAS to increase blood pressure 10

11
Beta-2 Receptors 11

12
Beta-2 Receptors Epinephrine only Arterial dilation Bronchodilation Relaxation of the uterus 12

13
Outline of the Lecture 13

14
Outline of the Lecture Review of Hemodynamics – Blood vessel structure, function – Regulation of cardiac output – Mechanisms of blood pressure regulation Disorders of blood pressure – Hypertension – Orthostatic hypotension Drugs that affect blood pressure Disorders of arterial circulation – Hyperlipidemia, atherosclerorosis Drugs that lower LDL cholesterol 14

15
Pulmonary and Systemic Circulation Description 15

16
Pulmonary and Systemic Circulation Description Likes this diagram a lot Depicts the circulatory system as two systems that are in tandem and are connected to each other in the heart Left ventricle – aorta – systemic circulation – right atria – right ventricle – pulmonary artery – pulmonary circulation 16

17
Pulmonary and Systemic Circulation Diagram 17

18
Pulmonary and Systemic Circulation Diagram 18 Baxter Corp. (1999)
")
19
Differences in the Pulmonary and the Systemic Systems 19

20
Differences in the Pulmonary and the Systemic Systems PULMONARY Low pressure system (MPAP 12 mmHg) Good for gas exchange SYSTEMIC High pressure system (MAP 90-100 mmHg) Good for distant transport, against gravity so the pressure needs to be higher 20
 Good for gas exchange SYSTEMIC High pressure system (MAP mmHg) Good for distant transport, against gravity so the pressure needs to be higher 20")
21
How Does Blood Get Back to the Heart? Diagram 21

22
How Does Blood Get Back to the Heart? 22 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p 461

23
How Does Blood Get Back to the Heart? Description 23

24
How Does Blood Get Back to the Heart? Description Pressure is high in the aorta, low in the large arteries, even lower in the arterioles, there is a big drop in capillaries, and gets even lower as it returns into the right atria – It is good to have a negative pressure in the right atria because you will be sucking the blood into the heart, which is a good thing 24

25
Principles of Blood Flow 25

26
Principles of Blood Flow Hemodynamics Heart is an intermittent pump, blood flow is pulsatile – This is not true if the person has a continuous heart pump 26

27
Factors Governing the Function of the Cardiovascular System 27

28
Factors Governing the Function of the Cardiovascular System Volume Pressure Resistance Flow 28

29
Determinants of Blood Pressure 29

30
Determinants of Blood Pressure BP = CO X Peripheral vascular resistance CO = SV X HR What determines peripheral vascular resistance? 30

31
Resistance of a Tube Description 31

32
Resistance of a Tube Description Peripheral vascular resistance – the resistance to flow in the vascular tree The radius of the tube is a huge factor in delivering flow because it is done to the fourth power!!! – Changing the radius of the tube just a little bit greatly changes the resistance of the flow and thus the flow itself 32

33
Resistance of a Tube Diagram 33

34
Resistance of a Tube Diagram 34 Porth, Pathophysiology, Concepts of Altered Health States, 7 th ed., 2005, Lippincott, p. 452. Also see p 322, point 2 in Porth, Essentials Big factor!

35
Volume and Pressure Distribution Description 35

36
Volume and Pressure Distribution Description When we get to the arterioles, there is a huge drop in pressure – The degree of constriction of the arterioles determines the peripheral vascular resistance, which then makes it important in determining blood pressure 4% of blood is in the left ventricle, 16% in the arteries, 4% in the capillaries, and 64% in the veins Veins are capacitance vessels – The veins serve as a storage place for the blood – If we want to increase cardiac output quickly, the veins can constrict and return the blood to the heart, sending a bolus to the heart to increase the stroke volume and thus the cardiac output 36

37
Volume and Pressure Distribution Diagram 37

38
Volume and Pressure Distribution Diagram 38 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 321. Arteriolar tone determines systemic vascular resistance

39
Pulmonary and Circulatory Systems Diagram, Lehne 39

40
Pulmonary and Circulatory Systems Diagram, Lehne 40 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p 461

41
Layers of the Blood Vessels 41

42
Layers of the Blood Vessels Intima- elastic layer Media- smooth muscle for diameter control (innervated by the SNS with alpha receptors) – Alpha receptors cause constriction of the vessels – The arteries have more smooth muscle than the veins Externa- fibrous and connective tissue for support 42 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 338

43
Resistance Arterioles Maintain Blood Pressure 43

44
Resistance Arterioles Maintain Blood Pressure Arteries have abundant smooth muscle. The diameter of the artery/arteriole is determined by the degree of contraction of the smooth muscle, which is mediated by the SNS (alpha receptors). The SNS maintains tone in the arteries 44 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 338
. The SNS maintains tone in the arteries 44 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p")
45
Blood Vessels and the Peripheral Circulation 45

46
Blood Vessels and the Peripheral Circulation Blood vessels are not pipes – Pipes cannot change their diameters, while blood vessels can Blood vessels are dynamic structures – They constrict and relax to adjust blood flow to meet varying needs of tissues/organs The heart, brain, liver, and kidney require large continuous flow – There are no alpha receptors on blood vessels going to the brain because we do not want to ever constrict then Skin and skeletal muscle require varying flow of blood, depending on the situation – Ex. if you just ate, you will need a lot of blood going to your digestive tract 46

47
Arteries and Arterioles 47

48
Arteries and Arterioles Elasticity allows for stretching during systole Arterioles have abundant smooth muscle Arterioles are the major resistance vessels for circulatory the system and basically determine the systemic vascular resistance Sympathetic fibers innervate arterioles cause them to constrict/relax as needed to maintain BP (alpha receptors) 48
 48")
49
Veins and Venules 49

50
Veins and Venules Collect blood from capillaries and carry it back to the heart Enlarge and store large quantities of blood and are then able to return the stored blood to the heart when needed Contract/expand to accommodate varying amounts Innervated by SNS (alpha receptors) Venous constriction can increase the preload to the heart by conducting stored blood into the vena cava – This will increase the cardiac output 50
 Venous constriction can increase the preload to the heart by conducting stored blood into the vena cava – This will increase the cardiac output 50")
51
Veins 51

52
Veins Valves prevent retrograde flow – Incompetent valves in venous varicosities – As we age, the valves may become incompetent Skeletal muscles help compress veins in “milking manner” up to heart Low pressure system – Pressure in venules is ~10 mm Hg and in the vena cava ~0 mmHg 52 Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 339.

53
Endothelial Cells 53

54
Endothelial Cells 54 Endothelial cells line all blood vessels. They are normally quite smooth and permit laminar (uninterrupted) blood flow. They also form a tight barrier in larger vessels Capillaries are more permissive of small molecules exiting and entering the vascular system because they possess fenestrations
 blood flow. They also form a tight barrier in larger vessels Capillaries are more permissive of small molecules exiting and entering the vascular system because they possess fenestrations.")
55
Capillaries 55

56
Capillaries Single cell-thick vessels that connect arterial and venous segments Wall composed of a single layer of endothelial cells surrounded by a basement membrane – Do not have smooth muscle In most vascular beds, capillaries have fenestrations that allow passage of water and small molecules but not large proteins. The basement membrane between the endothelial cells and the outside of the capillaries is very important 56 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 341.

57
Vascular Smooth Muscle and Sympathetic Nervous System 57

58
Vascular Smooth Muscle and Sympathetic Nervous System Norepinephrine-activated alpha receptors cause calcium channels in vascular smooth muscle to open, which produces vasoconstriction In some vascular beds, beta-2 receptors promote vasodilation by decreasing calcium. Calcium Causes Contraction in vascular smooth muscle – The more calcium that is present inside the cell, the more contraction is present Calcium channel blockers prevent vasoconstriction – Prevents calcium from going through the calcium channel so the calcium cannot cause contraction 58

59
Perfusion of Organs 59

60
Perfusion of Organs Tissue blood flow to a given organ is regulated on a minute-to-minute basis in relation to tissue needs Neural mechanisms regulate cardiac output and systemic vascular resistance (BP) to support local mechanisms Local control includes preferential vasoconstriction or vasodilation mediated by the SNS or by intrinsic mechanisms within the organ. 60

61
Tissue Factors Contributing to Local Control of Blood Flow 61

62
Tissue Factors Contributing to Local Control of Blood Flow Factors are released from an organ when it has too much or too little blood flow. In order to increase blood flow – Histamine Would cause dilation of the vessel Decrease blood flow – Serotonin Would cause constriction of the vessel Are these correct?* 62

63
Endothelial Control of Vascular Smooth Muscle 63

64
Endothelial Control of Vascular Smooth Muscle The endothelium produces factors that act on smooth muscle to produce vasoconstriction or vasodilation Vasodilating substances – Nitric Oxide Vasoconstricting substances – Angiotensin II, Prostaglandins, Endothelins The circulatory system is a dynamic structure that works to send blood to different organs that need more or less blood 64

65
Functional Anatomy of the Heart 65

66
66 Functional Anatomy of the Heart Pericardium: Sac around heart Normally, has a little bit of fluid in it in order to make movement easier Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 328. A “virtual space” which can become fluid or blood-filled (pericardial effusion).
..")
67
Contraction: Actin and Myosin Binding Description 67

68
Contraction: Actin and Myosin Binding Description Actin and myosin overlap and grab onto each other Calcium is what makes this process work 68

69
Contraction: Actin and Myosin Binding Diagram 69

70
Contraction: Actin and Myosin Binding Diagram 70 http://www.sci.sdsu.edu/movies/actin_myosin_gif.html Spirito et al., NEJM 336, pg 775, 1997

71
Heart Valves Keep Blood Flow Unidirectional Diagram 71

72
72 Heart Valves Keep Blood Flow Unidirectional Semilunar valves A-V valves Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 329.

73
Function of Heart Valves 73

74
Function of Heart Valves Major function of heart valves: Forward direction of blood flow Open and shut in order to keep blood moving forward in an unidirectional manner 74

75
Semilunar Valves 75

76
Semilunar Valves Control blood flow out of ventricles Aortic valve Pulmonic valve 76

77
Atroventricular Valves 77

78
Atroventricular Valves Control blood flow between atria and ventricles Tricuspid valve Mitral valve 78

79
Cardiac Conduction System 79

80
Cardiac Conduction System The conduction system stimulates the myocardium to contract and pump blood The conduction system controls the rhythm of the heart. Heart has two conduction systems – One controls atrial activity – One that controls ventricular activity – The two systems communicate when the impulse that causes atrial contraction travels to the ventricular system via the A-V node 80

81
Conduction System Diagram 81

82
Conduction System Diagram 82

83
SA Node 83

84
SA Node Pacemaker of the heart – Spontaneously depolarizes Impulses originate here Located in posterior wall RA Causes the atria to contract Fires at 60 -100 bpm if it is not innervated by anything – Can be influenced by the SNS and PNS Rate is determined by the autonomic nervous system – Increase HR: Sympathetic nervous system---NE---beta-1 receptors – Decrease HR: Parasympathetic nervous system ---acetylcholine--- muscarinic receptors 84

85
AV Node 85

86
AV Node Connects the atria and ventricles, provides one way conduction The speed of conduction of the AV node is much slower than the fibers in the atria or the ventricle At the AV node, the signal stops – Promotes filling of the ventricles before ejection Speed of conduction in the AV node is determined by the ANS – The SNS can speed up conduction and make the pause shorter (beta-1) – The PNS can slow conduction down and make the pause longer (muscarinic receptor) Can assume pacemaker function if SA fails to discharge – Can depolarize on its own and cause the ventricles to contract – Fires at 40 -60 bpm 86
 – The PNS can slow conduction down and make the pause longer (muscarinic receptor) Can assume pacemaker function if SA fails to discharge – Can depolarize on its own and cause the ventricles to contract – Fires at bpm 86")
87
Purkinje Fibers 87

88
Purkinje Fibers Supply the ventricles – Spread the impulse throughout the ventricular muscle Large fibers, rapid conduction for swift and efficient ejection of blood from heart Assume pacemaker of ventricles if AV fails – Intrinsic rate is 15-40 bpm 88 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 331.

89
ECG 89

90
ECG Electrical events recorded – Transmitted to the skin via conduction Electrical events precede mechanical events; know what they represent! – P Atrial depolarization – Pause caused by the AV node – QRS Ventricular depolarization – T Ventricular repolarization – U wave The repolarization of the atria 90 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p.331 & 333.

91
Cardiac Cycle 91

92
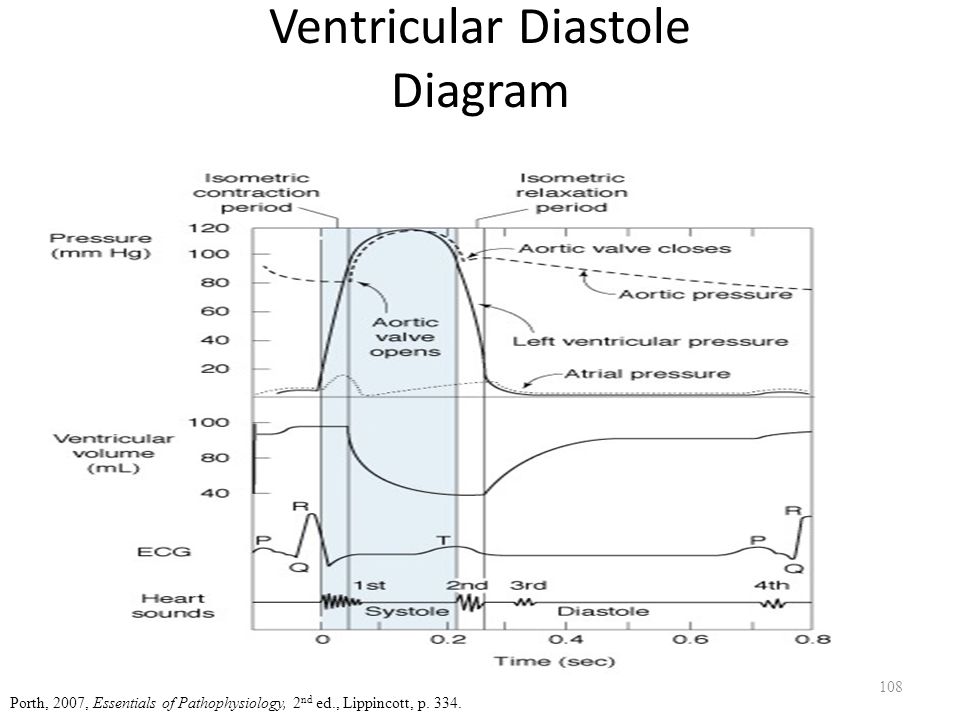
Cardiac Cycle Term used to describe the rhythmic pumping action of heart Cycle divided into 2 parts – Systole: period during which ventricles are contracting – Diastole: period during which ventricles are relaxed, filling with blood Simultaneous changes occur in pressure (LA,LV, aorta), ventricular volume, ECG, heart sounds during cardiac cycle 92
, ventricular volume, ECG, heart sounds during cardiac cycle 92")
93
The Wiggers Diagram 93

94
94 Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 334. The Wiggers Diagram

95
The Wiggers Diagram Description of Pressure 95

96
The Wiggers Diagram Description of Pressure At the beginning of systole, the pressure in the left ventricle is low, starts to contract (at this point, the aortic and the mitral valve are both closed), as the ventricle is contracting, pressure builds in the ventricle (isovolumetric contraction) The dotted line at the beginning is the aortic pressure The pressure in the ventricle and aorta are the same Pressure in the ventricle forces the aorta to open Pressure in the ventricle rises further until it is maximally contracted Pressure in the aortic route and in the ventricle are equal at this time because the pressure is the same When the ventricle pressure is lower than in the aorta, the aortic valve closes As the ventricle is relaxing, pressure in the ventricle drops a lot Isometric relaxation period – Pressure in low Diastole – The ventricle is relaxed – Ventricle pressure is staying low – Volume is increasing because the ventricle is filling Fills passively because the mitral valve opens Pressure between the atria and the ventricle are the same – The atria contracts to force more blood into the ventricle 96
, as the ventricle is contracting, pressure builds in the ventricle (isovolumetric contraction) The dotted line at the beginning is the aortic pressure The pressure in the ventricle and aorta are the same Pressure in the ventricle forces the aorta to open Pressure in the ventricle rises further until it is maximally contracted Pressure in the aortic route and in the ventricle are equal at this time because the pressure is the same When the ventricle pressure is lower than in the aorta, the aortic valve closes As the ventricle is relaxing, pressure in the ventricle drops a lot Isometric relaxation period – Pressure in low Diastole – The ventricle is relaxed – Ventricle pressure is staying low – Volume is increasing because the ventricle is filling Fills passively because the mitral valve opens Pressure between the atria and the ventricle are the same – The atria contracts to force more blood into the ventricle 96")
97
The Wiggers Diagram Other Elements 97

98
The Wiggers Diagram Other Elements The electrical stimuli come before the contractions or relaxations because the stimulation causes the contraction The little increase in atrial volume at the end is called the atrial kick – Contributes very little to the volume in the left ventricle May be important if the heart rate is really fast so the diastole is slow – May be important to end more to the volume Important in people with heart rate who need the kick to help the ventricles fill more At the middle is volume EKG Heart sounds 98

99
Ventricular Systole Diagram 99

100
Ventricular Systole Diagram 100 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 334.

101
Ventricular Systole Description 101

102
Ventricular Systole Description Isovolumic (isometric) contraction Ejection period. 102
 contraction Ejection period. 102")
103
Ventricular Systole Isovolumic (metric) Contraction 103
 Contraction 103")
104
Ventricular Systole Isovolumic (metric) Contraction Closure of AV valves (S1), all valves closed. No change in ventricular volume Ventricles contract When ventricular pressures > aortic and pulmonary pressures, semilunar valves open, leading to the ejection period 104

105
Ventricular Systole Ejection Period 105

106
Ventricular Systole Ejection Period Stroke volume ejected. Ventricles contract, then relax. Intraventricular pressures and become less than pressures in aorta and pulmonary arteries Blood from large arteries flows back toward ventricles and aortic/pulmonic valves shut (S2). 106
")
107
Ventricular Diastole Diagram 107

108
Ventricular Diastole Diagram 108 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 334.
109
Ventricular Diastole Description 109

110
Ventricular Diastole Description Ventricular relaxation and filling Isovolumic (isometric) relaxation Rapid filling period 110
 relaxation Rapid filling period 110")
111
Ventricular Diastole Isovolumic (metric) Relaxation 111
 Relaxation 111")
112
Ventricular Diastole Isovolumic (metric) Relaxation Semilunar valves closed Ventricles relaxed No change in ventricular volume, but ventricular pressure until it is less than atrial pressures. AV valves open, blood from atria enters ventricles, leading to rapid filling phase 112

113
Ventricular Diastole Rapid Filling Phase 113

114
Ventricular Diastole Rapid Filling Phase Most ventricular filling in first third of diastole (S3) During the last third, atria contract (atrial kick). 114

115
Atrial Contraction 115

116
Atrial Contraction Last third of ventricular diastole Gives additional thrust to ventricular filling Important during tachycardia or when heart disease impairs ventricular filling – May not be important in a person with a normal heart, especially at physiologic heart rates. Fourth heart sound (S4), when present, occurs when atria contract – Cannot always hear the S4 heart sound 116
, when present, occurs when atria contract – Cannot always hear the S4 heart sound 116.")
117
Cardiac Output 117

118
Cardiac Output Cardiac output (CO) – Amount of blood the heart pumps/minute – 3.5 - 8.0 L/minute In athletes, this could be much higher Stroke volume (SV) – Amount of blood the heart pumps each beat – 70 ml/beat CO = SV x HR CO varies with body activities. – Ex. sleeping vs. exercise CO varies by changes in SV and/or HR – SV – when veins contract – HR – more beats lead to more blood being pumped out 118

119
Heart Rate 119

120
Heart Rate Frequency with which blood is ejected from heart – One way to increase the cardiac output As HR → CO HR is increased by activation of beta-1 receptors and decreased by activation of muscarinic receptors on the SA node. BUT as HR → diastolic filling time – This occurs when heartrate increases too fast or too much diastolic filling time may SV and CO Tachycardia can be dangerous because the heart may not have time to fill adequately → CO 120

121
Equation for Cardiac Output 121

122
122

123
Stroke Volume Components 123

124
Stroke Volume Components Preload – the amount of blood that is returned to the heart from the veins – Ventricular filling (volume) Afterload – the pressure that the heart must press against in order to get the blood out – Pumping function – Resistance to ejection of blood from heart Contractility – how hard is the heart contracting – Pumping function of heart 124
 Afterload – the pressure that the heart must press against in order to get the blood out – Pumping function – Resistance to ejection of blood from heart Contractility – how hard is the heart contracting – Pumping function of heart 124")
125
Preload (“Volume”) 125
 125")
126
Preload (“Volume”) Represents the volume of blood the heart must pump with each beat – Ex. if the veins return 100mL to the heart and the heart does not pump out 100mL, the blood must stay in the heart, which is bad What the veins return to the heart is what the heart must pump out Largely determined by venous return and stretch of muscle fibers Venous return – 64% of blood volume in veins – Venous constriction mediated by alpha-1 receptors 126

127
Preload: Frank-Starling Law of the Heart 127

128
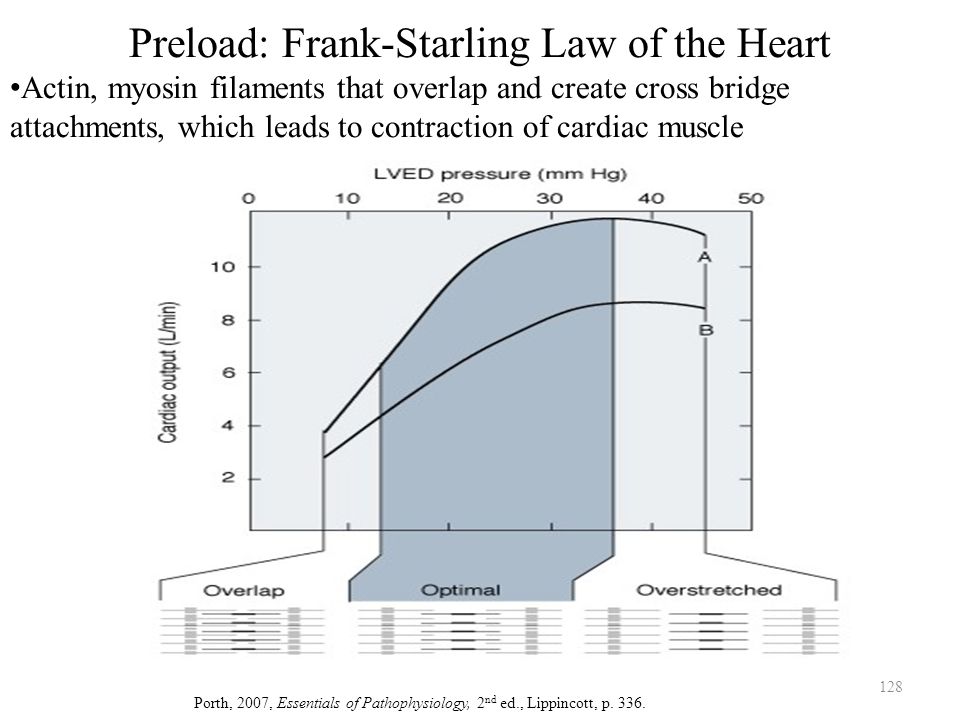
128 Preload: Frank-Starling Law of the Heart Actin, myosin filaments that overlap and create cross bridge attachments, which leads to contraction of cardiac muscle Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 336.
129
Preload: Frank-Starling Law of the Heart Description 129

130
Preload: Frank-Starling Law of the Heart Description An intrinsic property of the heart The actin and myosin filaments must overlap in order for the contraction of cardiac muscle – They may overlap a little, optimally, or too much Law – there is an optimal degree of overlap – This is determined by the end diastolic filling of the heart – If there is a little bit of volume in the heart, there is a lot of overlap and good contractility, but once the filaments slide, they cannot slide any more This means that there is not a lot of extra space to end into, so filaments cannot contract a lot – Optimal overlap leads to the best contractility – If you overfill the heart and overstretch the filaments, then cardiac output declines because the filaments cannot touch Not affected by the SNS – Has to do with the filling that the heart gets from the veins Optimal overlap leads to increased SV beyond what we would expect from the increased filling 130

131
Implications of the Frank-Starling Law 131

132
Implications of the Frank-Starling Law At normal volumes, as preload increases, stretch increases, which increases contractility. – CO goes up both because of the increased volume and increased contractility – The increase in contractility is independent of the SNS – it is an intrinsic property of the heart. At high volumes, the cardiac muscle is overstretched and contractility decreases. – This is usually seen only in patients with heart failure (covered in CVII) who have fluid overload. 132
 who have fluid overload")
133
Afterload (“Resistance”) 133
 133")
134
Afterload (“Resistance”) The heart must develop a pressure equal to the aortic pressure in order to open the valve Afterload - the amount of pressure the heart must develop during the period of isovolumic contraction to open the aortic and pulmonic valves. Without valve disease, afterload = diastolic pressure 134

135
Major Sources of Resistance 135

136
Major Sources of Resistance Arterial pressures are the major sources of resistance – Right ventricle: Pulmonary arterial pressure (low) – Left ventricle: Systemic arterial pressure (high – equal to the diastolic BP in the absence of valve disease) 136
 – Left ventricle: Systemic arterial pressure (high – equal to the diastolic BP in the absence of valve disease) 136")
137
Diseases of the Semilunar Valves 137

138
Diseases of the Semilunar Valves Disease of the aortic or pulmonic valves resistance – Stenosis/narrowing of the valve – This means that the heart has to develop an increased pressure to open the diseased valve. The decrease in the valve will have a big impact on resistance, flow, and afterload because the radius is done to the fourth power – Diastolic hypertension also increases the pressure necessary to open the aortic valve. 138

139
Effect of Afterload on CO Diagram 139

140
Effect of Afterload on CO Diagram 140 Guyton, 2006, Textbook of Medical Physiology, 11th ed.,Saunders, p. 114.

141
Effect of Afterload on CO Description 141

142
Effect of Afterload on CO Description In normal people without disease, afterload has little impact on cardiac output – The ventricle can develop the pressures – Most important thing in determining CO is the preload The heart pumps what it receives from the venous system In a person with impaired contractility, this curve is shifted back to the left – At normal aortic pressures, there may be a decrease in cardiac output – With impaired contractility, afterload becomes important 142

143
Contractility 143

144
Contractility Ability of the heart to change its force of contraction – The heart can contract harder when it is needed Strongly influenced by number of calcium ions that are available to participate in the contractile process. – Determined by biochemical and biophysical properties that govern actin and myosin interactions in myocardial cells (Frank-Starling mechanism). – Activation of beta-1 receptors in the ventricles by norepinephrine (SNS) increases the availability of calcium ions and increases contractility. The heart’s contractility can be stimulated by the sympathetic nervous system 144
. – Activation of beta-1 receptors in the ventricles by norepinephrine (SNS) increases the availability of calcium ions and increases contractility. The heart’s contractility can be stimulated by the sympathetic nervous system 144.")
145
Determinants of Blood Pressure 145

146
Determinants of Blood Pressure BP = CO X Peripheral vascular resistance CO = SV X HR 146

147
Mechanisms of BP Regulation Arterial Pressure 147

148
Mechanisms of BP Regulation Arterial Pressure Arterial pressure must remain relatively constant as blood flow shifts from one area of body to another – Feedback mechanisms are short-term and long-term to regulate the blood pressure to remain constant Method by which arterial pressure is regulated depends on whether short-term or long-term adaptation is needed 148

149
Mechanisms of BP Regulation ANS, RAAS, Kidneys 149

150
Mechanisms of BP Regulation ANS, RAAS, Kidneys Autonomic nervous system – short-term regulation RAAS (Renin-angiotensin-aldosterone system) – longer term regulation of blood pressure Kidneys – control blood volume as well as the RAAS – a long-term mechanism of blood pressure control. – The kidneys are very important in long-term regulation of blood pressure 150

151
The Baroreceptor Reflex Diagram 151

152
The Baroreceptor Reflex Diagram 152 Baroreceptors in the aortic arch and carotid artery Autonomic centers in the brainstem Cardiac muscle, cardiac conduction system, and vascular smooth muscle.

153
The Baroreceptor Reflex Description 153

154
The Baroreceptor Reflex Description Baroreceptors sense pressure in the aortic arch and the carotid artery Send information to the medulla in the autonomic centers in the brainstem Send impulses to the heart and vessels to lower the blood pressure (if stimulation is too high) or to raise the blood pressure (if stimulation is too low) 154
 or to raise the blood pressure (if stimulation is too low) 154")
155
The Sensory Components of the Baroreceptor Reflex – Chemo and Stretch Receptors 155

156
The Sensory Components of the Baroreceptor Reflex – Chemo and Stretch Receptors 156 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 364.

157
ANS Regulation of BP – the Baroreceptor Reflex 157

158
ANS Regulation of BP – the Baroreceptor Reflex 158 *Be sure you know which receptors are where!!! McCance & Heuther, 2002, Pathophysiology: The Biologic Basis for Disease in Adults & Children, Mosby, p.961

159
ANS Regulation of BP – the Baroreceptor Reflex Description 159

160
ANS Regulation of BP – the Baroreceptor Reflex Description Vagus nerve sends signals to the SA node to slow down the heart SNS increases CO by increasing HR and contractility SNS innervates arterioles to cause them to constrict (alpha) to raise blood pressure SNS innervates veins to cause them to constrict to increase preload to increase CO Baroreceptor reflex is happening all of the time If blood pressure is too low, medulla instructs SNS centers in spinal cord to send information to the SA node through beta-1 receptors and the AV node to speed up the heart 160
 to raise blood pressure SNS innervates veins to cause them to constrict to increase preload to increase CO Baroreceptor reflex is happening all of the time If blood pressure is too low, medulla instructs SNS centers in spinal cord to send information to the SA node through beta-1 receptors and the AV node to speed up the heart 160")
161
Neurotransmitters 161

162
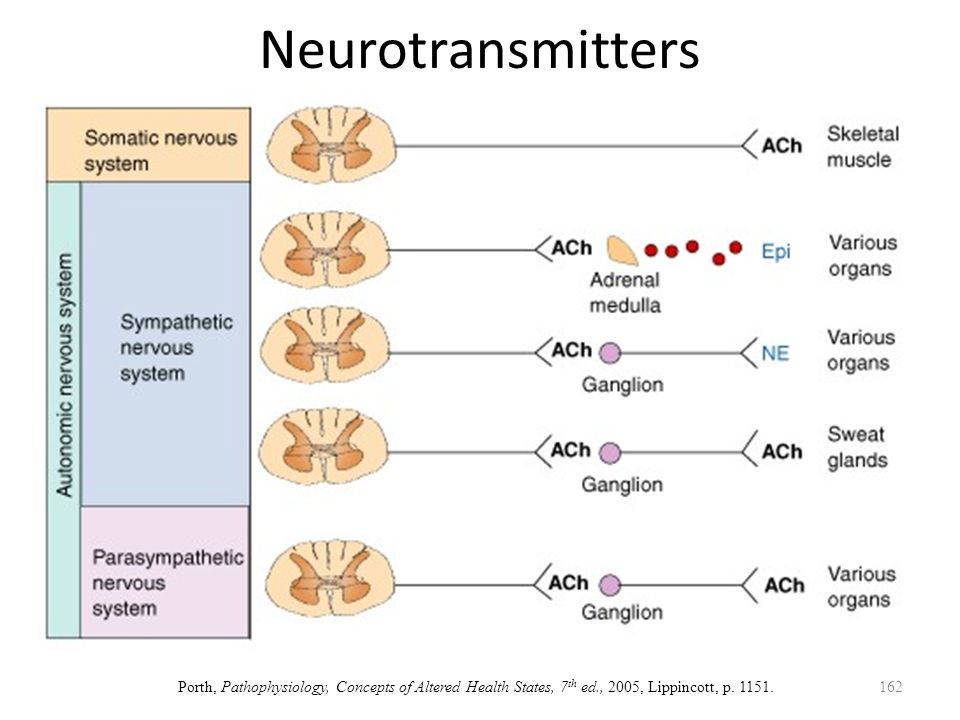
Neurotransmitters 162 Porth, Pathophysiology, Concepts of Altered Health States, 7 th ed., 2005, Lippincott, p. 1151.
163
Long-term Regulation of Blood Pressure 163

164
Long-term Regulation of Blood Pressure Primarily controlled by kidneys Neural mechanisms act rapidly, but cannot maintain their effectiveness over time so the kidneys are used Kidneys’ control in long term is through regulation of Na + and H 2 0 balance – RAAS – Vasopressin 164

165
Renin-Angiotensin-Aldosterone System Diagram 165

166
Humoral Mechanisms: Renin- angiotensin- aldosterone system 166 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 365. MUST KNOW THIS!

167
Renin-Angiotensin-Aldosterone System Description 167

168
Renin-Angiotensin-Aldosterone System Description When renal blood pressure falls, juxtaglomerular cells of the kidney acts on renin Renin works on angiotensinogen Angiotensinogen is converted to angiotensin I Angiotensin I becomes angiotensin II – Angiotensin II constricts arteries and causes the adrenal cortex to release aldosterone Aldosterone increases Na reabsorption, which increases water reabsorption 168

169
Vasopressin (Antidiuretic Hormone (ADH)) Diagram 169
) Diagram 169")
170
170 Vasopressin (Antidiuretic Hormone (ADH)) Porth, Pathophysiology, Concepts of Altered Health States, 7 th ed., 2005, Lippincott, p. 756.

171
Vasopressin (Antidiuretic Hormone (ADH)) Description 171
) Description 171")
172
Vasopressin (Antidiuretic Hormone (ADH)) Description ADH is released in result to changes in serum osmolality strength – When dehydrated, the serum osmolalitiy goes up, which stimulates the hypothalamus 172
) Description ADH is released in result to changes in serum osmolality strength – When dehydrated, the serum osmolalitiy goes up, which stimulates the hypothalamus 172")
173
The ANS and RAAS Systems Work in Concert to Maintain Blood Pressure 173

174
174 Porth, Pathophysiology, Concepts of Altered Health States, 7 th ed., 2005, Lippincott, p. 756. The ANS and RAAS systems work in concert to maintain blood pressure

175
Which of the following is an important determinant of cardiac output in a normal person? 175

176
Which of the following is an important determinant of cardiac output in a normal person? 1.Afterload. 2.Heart rate. 3.Venous return (preload) 4.Total peripheral resistance. - Component of afterload 176
 4.Total peripheral resistance. - Component of afterload 176.")
177
You assess a patient’s pulse to be 40 bpm. He is not an athlete. Given this HR, the electrical impulses in the heart are probably originating from: 177

178
You assess a patient’s pulse to be 40 bpm. He is not an athlete. Given this HR, the electrical impulses in the heart are probably originating from: 1.SA Node 2.AV Node - Could be originating in the AV node 3.An ectopic atrial focus - This leads lead to increased heartrate 4.Purkinje Fibers - Could be originating from here as well 178

179
Angiotensin II causes 179

180
Angiotensin II causes 1.Release of aldosterone 2.Vasoconstriction of arterioles 3.Increased arterial blood pressure 4.All of the above 180

181
DISORDERS OF BLOOD PRESSURE REGULATION: HYPERTENSION AND ORTHOSTATIC HYPOTENSION 181

182
Orthostatic Hypotension 182

183
Orthostatic Hypotension Abnormal drop in BP on assumption of the standing position – People can actually faint from this Defined as a drop in systolic pressure > 20 mm Hg or drop in diastolic pressure > 10 mm Hg when going from lying to standing In absence of normal circulatory reflexes and/or if blood volume is decreased, blood pools in lower part of the body when the standing position is assumed (decreased venous return), CO and blood flow to the brain is inadequate dizziness, syncope (fainting), or both Occurs when the baroreceptor is not working properly or the person is dehydrated 183
, CO and blood flow to the brain is inadequate dizziness, syncope (fainting), or both Occurs when the baroreceptor is not working properly or the person is dehydrated 183")
184
Orthostatic Hypotension Diagram 184

185
185 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 374 Orthostatic Hypotension Diagram

186
Compensatory Mechanisms of Orthostatic Hypotension 186

187
Compensatory Mechanisms of Orthostatic Hypotension Stand up, drop in blood pressure, compensated by increased venous return and increased heart rate – If you are taking a beta blocker is would prevent the heart rate from increasing – Alpha blocker would prevent the vasoconstriction Dehydration is a big cause of people fainting 187

188
Causes of Orthostatic Hypotension 188

189
Causes of Orthostatic Hypotension Reduced blood volume (dehydration) (reduced preload) – This is the most common cause of dizziness and fainting, especially in young, health people. Drug-induced orthostatic hypotension – Impairment of venous return (reduced preload) (Ca 2+ channel blockers) – Impairment of the baroreceptor reflex (beta blockers, alpha-1 blockers) – Diuretics (reduced preload) Aging – sluggish reflexes, including the baroreceptor reflex Bedrest – deconditioning Disorders of the autonomic nervous system – Autonomic neuropathy – neuropathy of all of the nerves The autonomic ones may be affected 189
 (Ca 2+ channel blockers) – Impairment of the baroreceptor reflex (beta blockers, alpha-1 blockers) – Diuretics (reduced preload) Aging – sluggish reflexes, including the baroreceptor reflex Bedrest – deconditioning Disorders of the autonomic nervous system – Autonomic neuropathy – neuropathy of all of the nerves The autonomic ones may be affected 189.")
190
Treatment of Orthostatic Hypotension 190

191
Treatment of Orthostatic Hypotension Address the alleviating cause – Rehydrate, change medications Help cope with disorder, prevent falls, injury – Gradual ambulation (sit on edge of bed, move legs) – Avoid venodilation (drinking ETOH; exercise in warm environment) – Maintain hydration 191
 – Avoid venodilation (drinking ETOH; exercise in warm environment) – Maintain hydration 191")
192
Hypertension Description 192

193
Hypertension Description Common health problem in adults A leading risk factor for cardiovascular disorders (myocardial infarction, heart failure, stroke, vascular disease) More common in young men than young women, blacks compared with whites, in persons from lower socioeconomic groups, and with increasing age Diabetics are more likely to have hypertension and it is more likely to lead to cardiovascular disease than in nondiabetics. 193

194
Primary Hypertension 194

195
Primary Hypertension “Essential hypertension” Chronic elevation of BP occurs without evidence of other disease 90-95% of hypertension – Much more common than secondary hypertension 195

196
Secondary Hypertension 196

197
Secondary Hypertension Elevation of BP occurs from some other disorder – Kidney disease – Chronic renal failure Kidney thinks that it does not have enough blood flow, which activates the RAAS – Disorders of adrenocorticoid hormones (pheochromocytoma) 197
 197")
198
Hypertension Definitions 198

199
Hypertension Definitions JNC-VII * (June 2003) – “Prehypertension” (120-139/80-89) – Stage I (140-159/90-99) – Stage II (160-179/100-109) – Stage III (>180/>110) * 7th Report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure 199
 – Prehypertension ( /80-89) – Stage I ( /90-99) – Stage II ( / ) – Stage III (>180/>110) * 7th Report of the Joint National Committee on Detection, Evaluation and Treatment of High Blood Pressure 199")
200
Constitutional Risk Factors 200

201
Constitutional Risk Factors Family history – Hereditary pattern unclear, genes not identified Age related changes – BP higher with advancing age Insulin resistance, metabolic syndrome, diabetes (especially type II) Race – African Americans more prevalent, early onset, more severe; greater renal, CV damage – Less known about other races 201
 Race – African Americans more prevalent, early onset, more severe; greater renal, CV damage – Less known about other races 201")
202
Lifestyle Risk Factors 202

203
Lifestyle Risk Factors Diet high in Na + and saturated fats Obesity – When people lose weight, a lot of times it result in their blood pressure decreasing Physical inactivity Excessive alcohol consumption Oral contraceptives in predisposed women 203

204
Consequences of Hypertension 204

205
Consequences of Hypertension Usually related to long term effects of HTN on other organs, “target organ damage”. HTN seems to accelerate atherosclerotic vascular disease (covered later today) – Heart Left ventricular hypertrophy (the heart muscle has to increase in size to pump blood against the aortic resistance) Coronary artery disease (angina, myocardial infarction) Heart failure – Brain Stroke or transient ischemic attack – Chronic kidney disease – Peripheral vascular disease – Hypertensive retinopathy Usually does not have any symptoms 205
 – Heart Left ventricular hypertrophy (the heart muscle has to increase in size to pump blood against the aortic resistance) Coronary artery disease (angina, myocardial infarction) Heart failure – Brain Stroke or transient ischemic attack – Chronic kidney disease – Peripheral vascular disease – Hypertensive retinopathy Usually does not have any symptoms 205.")
206
Consequences of HTN Heart 206

207
Consequences of HTN Heart Heart: LV Hypertrophy – workload of LV ( afterload); LV tries to compensate for workload. – LV hypertrophy is major risk factor for ischemic heart disease (myocardial infarction), dysrhythmias, heart failure, sudden death 207
, dysrhythmias, heart failure, sudden death 207.")
208
Consequences of HTN Vascular Damage 208

209
Consequences of HTN Vascular Damage Coronary arteries – myocardial infarction (CVII) Peripheral blood vessels – peripheral vascular disease Kidney – renal failure Cerebral blood vessels – stroke 209
 Peripheral blood vessels – peripheral vascular disease Kidney – renal failure Cerebral blood vessels – stroke 209")
210
Diagnosis of Hypertension 210

211
Diagnosis of Hypertension Repeated BP measurements – Average of > 2 readings taken at > 2 visits after an initial screening visit; over several months Laboratory tests, x-rays looking for target organ damage – There is no specific test for hypertension, but you can look at the target organs – ECG, Urinalysis, Hb (erythropoietin in kidneys- anemic due to kidney disease), Hct, Na +, K +, Cr (major indicator of kidney function), glucose, triglycerides (tells about other factors that may influence disease), cholesterol 211
, Hct, Na +, K +, Cr (major indicator of kidney function), glucose, triglycerides (tells about other factors that may influence disease), cholesterol 211")
212
Treatment of Hypertension 212

213
Treatment of Hypertension Lifestyle modification is the first line of treatment – Weight reduction, regular physical exercise, DASH eating plan (a lot of fruits and vegetables, very little meat), reduction of dietary sodium intake, moderation of alcohol intake Pharmacologic treatment Goal: To achieve and maintain systolic BP below 140 mm Hg and diastolic BP below 90 mm Hg – The better people control their blood pressure, the less likely they are to suffer the negative effects of the hypertension on target organs 213
, reduction of dietary sodium intake, moderation of alcohol intake Pharmacologic treatment Goal: To achieve and maintain systolic BP below 140 mm Hg and diastolic BP below 90 mm Hg – The better people control their blood pressure, the less likely they are to suffer the negative effects of the hypertension on target organs 213")
214
Sites of Action of Hypertension Diagram 214

215
215 Lehne, 2009, Pharmacology for Nursing Care, 6 7h ed., Elsevier, p. 500

216
Pharmacologic Treatment of Hypertension 216

217
Pharmacologic Treatment of Hypertension Diuretics Sympatholytics Act on RAAS Others 217 Adapted from Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, Table 46-5, p. 502

218
Sympatholytics 218

219
Sympatholytics Interfere with the sympathetic nervous system Beta-adrenergic blockers Alpha-1 adrenergic blockers Centrally-acting alpha-2 agonists Drugs that block norepinephrine release 219

220
Drugs that Act on the RAAS 220

221
Drugs that Act on the RAAS Renin inhibitor ACE inhibitors Angiotensin II receptor blockers Aldosterone antagonists 221

222
Other Drugs 222

223
Other Drugs Ca +2 channel blockers Direct-acting vasodilators 223

224
Pharmacologic Treatment Compliance 224

225
Pharmacologic Treatment Compliance Compliance is a huge issue – Lifetime treatment – Many of the drugs have unpleasant side effects – Many are expensive 225

226
Algorithm for Treating Hypertension 226

227
Algorithm for Treating Hypertension 227 Lifestyle modifications - Increase exercise (aerobic, decrease weight) Goal BP not met Stage 1 – thiazide diuretic /consider ACEI, ARB, beta blocker, CCB or combination Stage 2 – 2-drug combo (usually a thiazide + ACEI, ARB, beta blocker or CCB) Goal BP not met Optimize dosage or add a drug from a different class Continue adding drugs from other classes until goal is achieved Goal BP not met Adapted from Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 507

228
Classes of Antihypertensive Drugs Recommended for Initial Therapy in Patients with High-Risk Comorbid Conditions 228

229
Classes of Antihypertensive Drugs Recommended for Initial Therapy in Patients with High-Risk Comorbid Conditions 229 ConditionDrug Classes Recommended for Initial Therapy of HTN DiureticBeta Blocker ACEIARBCCBAldosterone Antagonist Heart FailureXXXXX Post MIXXX Coronary Artery Disease Risk XXXX DiabetesXXXXX Chronic Kidney Disease XX Recurrent Stroke Prevention XX Adapted from Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 508

230
Drugs That Affect BP: Diuretics Diagram 230

231
Drugs That Affect BP: Diuretics Diagram 231 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 500

232
Classification of Diuretics 232

233
Classification of Diuretics Thiazide diuretics – Hydrochlorothiazide (HCTZ®) and chlorthalidone – Most common High-ceiling (loop)– Furosemide (Lasix®) K + sparing: – Non-aldosterone antagonists - Triamterene (Dyrenium®) – Aldosterone receptor antagonists – Spironolactone (Aldactone) Osmotic diuretics – Mannitol All diuretics indirectly prevent the re- absorption of water in the kidneys!, most of them by preventing the reabsorption of sodium 233
 and chlorthalidone – Most common High-ceiling (loop)– Furosemide (Lasix®) K + sparing: – Non-aldosterone antagonists - Triamterene (Dyrenium®) – Aldosterone receptor antagonists – Spironolactone (Aldactone) Osmotic diuretics – Mannitol All diuretics indirectly prevent the re- absorption of water in the kidneys!, most of them by preventing the reabsorption of sodium 233")
234
Thiazides 234

235
235 Thiazides Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 445 Prevent re-absorption of sodium in the distal tubule.

236
Thiazides Hydrochlorthiazide and Chlorthalidone Uses 236

237
Thiazides Hydrochlorthiazide and Chlorthalidone Uses Uses: Essential hypertension – Often first drug used – May be part of multiple-drug therapy Edema – Preferred drugs for mobilizing edema associated with incompetent, premenstrual fluid retention, or mild, moderate heart failure 237

238
Thiazide Diuretics Adverse Effects 238

239
Thiazide Diuretics Adverse Effects Hypokalemia Hyponatremia, hypochloremia, dehydration Orthostatic hypotension due to the dehydration Avoid in pregnancy if possible – May reduce placental perfusion (not for routine use in pregnancy) Nocturia if taken at night 239
 Nocturia if taken at night 239")
240
Thiazide Diuretics Drug Interactions 240

241
Thiazide Diuretics Drug Interactions Digoxin→digoxin toxicity (ALL K + -LOSING DIURETICS) Lithium→lithium toxicity (ALL DIURETICS!!!) – Increase the blood levels of lithium because they rid the body of water – Diuretics are contraindicated for people on lithium NSAIDS→ Reduced natriuresis/diuresis Will reduce the diuretics’ ability to cause diuresis 241
 Lithium→lithium toxicity (ALL DIURETICS!!!) – Increase the blood levels of lithium because they rid the body of water – Diuretics are contraindicated for people on lithium NSAIDS→ Reduced natriuresis/diuresis Will reduce the diuretics’ ability to cause diuresis 241")
242
Loop Diuretics 242

243
Loop Diuretics 243 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 445 Prevent the re-absorption of sodium from the ascending Loop of Henle.

244
Furosemide (Lasix®) 244
 244")
245
Furosemide (Lasix®) A second-line diuretic for hypertension but has many other uses. Used primarily for pulmonary edema associated with congestive heart failure Edema of hepatic, cardiac, or renal origin unresponsive to less efficacious diuretics – Promotes diuresis in renal impairment 245

246
Loop Diuretics Adverse Effects 246

247
Loop Diuretics Adverse Effects Hypokalemia Hyponatremia, hypochloremia, dehydration Orthostatic hypotension Ototoxicity, especially in large doses Avoid in pregnancy if possible Nocturia if taken at night 247

248
Loop Diuretics Drug Interactions 248

249
Loop Diuretics Drug Interactions Digoxin – hypokalemia is dangerous with digoxin with potassium levels are very important with the way that digoxin works Nitrates/other antihypertensives – increased hypotensive effects Other ototoxic drugs (aminoglycoside antibiotics) Lithium – lithium toxicity – ALL diuretics are contraindicated for people on lithium NSAIDS can attenuate the diuretic effect of furosemide 249
 Lithium – lithium toxicity – ALL diuretics are contraindicated for people on lithium NSAIDS can attenuate the diuretic effect of furosemide 249")
250
Potassium-Sparing Diuretics 250

251
251 Potassium-Sparing Diuretics Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 445 Prevent the re-absorption of sodium from the collecting tubule and duct.

252
Spironolactone - Aldactone 252

253
Spironolactone - Aldactone® Hypertension Edema Commonly used in combination with thiazide or loop diuretics Effects are delayed – Takes about one day or so to work 253

254
Spironolactone (Aldactone®) Adverse Effects 254
 Adverse Effects 254")
255
Spironolactone (Aldactone®) Adverse Effects Hyperkalemia – Avoid the use of potassium supplements Avoid salt supplements because they are made of potassium chloride – Synergistic with ACE inhibitors and ARBs Spironolactone blocks the effects of aldosterone ACE inhibitors and ARBs block the secretion of aldosterone – Can be extremely dangerous Can stop your heart!! Endocrine effects – Spironolactone has a steroid structure and can cause a variety of effects similar to steroid hormones, such as gynecomastia and impotence in men, menstrual irregularities, hirsutism, and deepening of the voice in women 255

256
Spironolactone (Aldactone®) Drug Interactions 256
 Drug Interactions 256")
257
Spironolactone (Aldactone®) Drug Interactions Potassium supplements and salt substitutes are contraindicated ACE inhibitors or ARBs may exacerbate the tendency to hyperkalemia Pregnancy category D because of steroid- like effects on the fetus 257
 Drug Interactions Potassium supplements and salt substitutes are contraindicated ACE inhibitors or ARBs may exacerbate the tendency to hyperkalemia Pregnancy category D because of steroid- like effects on the fetus 257")
258
Triamterene 258

259
Triamterene Often given in combination with a thiazide – Dyazide = hydrochlorothiazide + triamterene Hydrochlorothiazide causes hypokalemia and triamterene causes hyperkalemia, so the two drugs kind of balance each other out 259

260
Triamterene Adverse Effects 260

261
Triamterene Adverse Effects Hyperkalemia – AVOID K + supplements 261

262
Triamterene Drug Interactions 262

263
Triamterene Drug Interactions ACE Inhibitors/ARBs: Hyperkalemia potential NSAIDS may blunt diuretic effect and indomethacin may precipitate renal failure Take after meals in AM Avoid potassium rich diet items -- bananas, orange juice, salt substitutes (which are likely to be KCl) 263
 263")
264
Osmotic Diuretics - Mannitol 264

265
Osmotic Diuretics - Mannitol 265 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 445 Prevents re-absorption of water from the proximal tubule.

266
Mannitol 266

267
Mannitol Must be given parenterally Therapeutic uses – Prophylaxis of renal failure – Reduction of intracranial pressure Draws water out of the brain – Increased intra-ocular pressure When mannitol is in the bloodstream, before it gets into the renal tubules, it increases the osmotic pressure of the blood and draws edema fluid into the vascular system. Mannitol is filtered into the glomerulus, drawing the excess water with it and holding it in the renal tubules for excretion. 267

268
Osmotic Diuretics Adverse Effects 268

269
Osmotic Diuretics Adverse Effects Edema (caused by mannitol leaving the circulation and drawing water into the tissues with it) – Administer with extreme caution in heart failure because of its ability to increase vascular volume and overload the heart. Dehydration Orthostatic hypotension 269

270
Osmotic Diuretics Drug Interactions 270

271
Osmotic Diuretics Drug Interactions Mannitol is not metabolized, very inert. It has no significant drug interactions 271

272
Drugs Acting on RAAS Diagram 272

273
Drugs Acting on RAAS Diagram 273 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 500 Renin inhibitor

274
Renin Inhibition Diagram 274

275
Renin Inhibition Diagram 275

276
Renin Inhibitor Description 276

277
Renin Inhibitor Description Renin inhibition should prevent all activation of the renin-angiotensin aldosterone system. Only one such drug, aliskiren (Tekturna), is approved for use as monotherapy or in combination with hydrochlorothiazide. Like other drugs that target the RAAS, aliskiren is pregnancy category D because of evidence of fetal harm. Not used a lot yet 277
, is approved for use as monotherapy or in combination with hydrochlorothiazide. Like other drugs that target the RAAS, aliskiren is pregnancy category D because of evidence of fetal harm. Not used a lot yet 277.")
278
ACE Inhibitors (ACEI) 278
 278")
279
279 Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 365. ACE Inhibitors (ACEI) Introduced in the late 1980s Angiotensin converting enzyme inhibitors Work in the lung Captopril, lisinopril, enalapril, and others - All end in -pril
 Introduced in the late 1980s Angiotensin converting enzyme inhibitors Work in the lung Captopril, lisinopril, enalapril, and others - All end in -pril.")
280
280 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 469

281
Therapeutic Uses of ACEI 281

282
Therapeutic Uses of ACEI Hypertension Heart failure Protective effects in diabetic nephropathy – Protect the kidneys Post MI prophylaxis – Prevent a second heart attack in people who have had one heart attack Prevention of MI, stroke, and death in patients at risk 282

283
Therapeutic Uses of ACEIs Hypertension 283

284
Therapeutic Uses of ACEIs Hypertension Initial responses: reduced formation of angiotensin II Prolonged therapy: additional reduction in BP due to reduced formation of angiotensin II REDUCE THE RISK OF CV MORTALITY CAUSED BY HEART FAILURE – People who are having heart failure, should be on an ACE inhibitor or an ARB REDUCE THE RISK OF RENAL FAILURE IN DIABETICS 284

285
Things Not Caused by ACE Inhibitors 285

286
Things Not Caused by ACE Inhibitors Do not interfere with cardiovascular reflexes – Do not cause orthostatic hypotension because they do not interfere with the baroreceptors Do not cause hypokalemia but may contribute to the tendency to hyperkalemia if given with potassium- sparing diuretics. Do not induce lethargy, weakness, sexual dysfunction as other antihypertensives may. 286

287
ACE Inhibitors Adverse Effects 287

288
ACE Inhibitors Adverse Effects Bilateral renal artery stenosis is a contraindication because these drugs can precipitate acute renal failure in these patients – These people need their high blood pressure in order to get the blood past the stenotic valve and into the kidney Dry cough – an effect of increased bradykinin First dose hypotension – Most prominent in patients with very high BP or those on diuretics. – Should start with a lower dose Teratogenic – contraindicated in pregnancy Angioedema – due to increased bradykinin, may be very serious – Can be very serious if it is present in the mouth of throat 288

289
Angioedema Diagram 289

290
290 Westra S and de Jager C. N Engl J Med 2006;355:295 A 75-year-old man presented to the emergency department with diffuse swelling of his tongue that had begun a few hours earlier. He had been taking 25 mg of captopril twice daily for the past 3 years because of hypertension. He was treated with epinephrine, corticosteroids, and antihistamines and the swelling resolved over a three-hour period. The angioedema was likely due to the angiotensin-converting enzyme inhibitor.

291
ACE Inhibitors Drug Interactions 291

292
ACE Inhibitors Drug Interactions Digoxin Increased digoxin levels Lithium Increased lithium levels/toxicity K + sparing diuretics hyperkalemia Potassium supplements hyperkalemia 292

293
ACE Inhibitors Additional Information 293

294
ACE Inhibitors Additional Information Can be combined with a thiazide diuretic All are oral except for enalaprilat, which is IV only Patients with renal impairment may need dosage reduction 294

295
Angiotensin II Receptor Blockers (ARBs) 295
 295")
296
296 Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 365. Angiotensin II Receptor Blockers (ARBs) Losartan, valsartan, candesartan, and others - End in sartan
 Losartan, valsartan, candesartan, and others - End in sartan.")
297
ARB Therapeutic Uses 297

298
ARB Therapeutic Uses Widely used – Not as widely used as the ACE inhibitors Hypertension – Reductions in BP = ACEI Heart failure – prevent the progression and improve outcomes Diabetic nephropathy – prevents progression Post-MI prophylaxis Stroke prevention 298

299
ARBs Adverse Effects 299

300
ARBs Adverse Effects Well tolerated Do not cause cough Angioedema – Much more rare than ACE inhibitors Fetal harm – contraindicated in pregnancy Renal failure 300

301
ARBs Drug Interactions 301

302
ARBs Drug Interactions Hypotensive effects are additive with other anti-HTN drugs Do not cause hyperkalemia but may contribute if given with potassium-sparing diuretics 302

303
Aldosterone Antagonists 303

304
304 Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 365. Aldosterone Antagonists Spironolactone Eplerenone (Inspra) Potassium-sparing diuretics (covered previously as diuretics) Block the aldosterone receptor Promote Na + and H 2 0 excretion in the collecting tubule and duct
 Potassium-sparing diuretics (covered previously as diuretics) Block the aldosterone receptor Promote Na + and H 2 0 excretion in the collecting tubule and duct.")
305
Sympatholytics (Antiadrenergics) Outline 305
 Outline 305")
306
Sympatholytics (Antiadrenergics) Outline Beta blockers Alpha-1 blockers Alpha/beta blockers Centrally acting alpha-2 agonists Adrenergic neuron blockers (inhibit synthesis or release of norepinephrine) Ganglionic blockers (not used, we will not cover) 306
 Outline Beta blockers Alpha-1 blockers Alpha/beta blockers Centrally acting alpha-2 agonists Adrenergic neuron blockers (inhibit synthesis or release of norepinephrine) Ganglionic blockers (not used, we will not cover) 306")
307
Sympatholytics (Antiadrenergics) Diagram 307
 Diagram 307")
308
Sympatholytics (Antiadrenergics) Diagram 308 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 500 Sites of Action

309
Beta-Adrenergic Blockers 309

310
Beta-Adrenergic Blockers Widely used anti-hypertensive drugs Actions in hypertension – Blockade of cardiac beta-1 receptors→↓HR and contractility → ↓CO – Suppress reflex tachycardia caused by vasodilators – Blockade of beta-1 receptors in JG cells in kidney → ↓ renin release → ↓ RAAS mediated vasoconstriction (angiotensin II) and volume expansion (aldosterone) – Long-term use peripheral vascular resistance 310 *Recall from Dr McLeskey’s lecture; Lehne Chapter 18
 and volume expansion (aldosterone) – Long-term use peripheral vascular resistance 310 *Recall from Dr McLeskey’s lecture; Lehne Chapter 18")
311
Beta-Adrenergic Blockers Affinity for Receptors 311

312
Beta-Adrenergic Blockers Affinity for Receptors Some block both beta-1 and beta-2 receptors (nonselective) Some have greater affinity for beta-1 than beta-2 (“cardioselective”) – but the selectivity is not absolute Some are partial agonists – they are said to have “intrinsic sympathomimetic activity” or ISA 312
 Some have greater affinity for beta-1 than beta-2 ( cardioselective ) – but the selectivity is not absolute Some are partial agonists – they are said to have intrinsic sympathomimetic activity or ISA 312")
313
Clinical Pharmacology of Some Beta Blockers 313

314
314 Generic/trade nameISA Cardioselective (beta 1 > beta 2 ) Acebutolol/Sectal®+ Atenolol/Tenormin®0 Esmolol/Brevibloc®0 Metolprolol/Lopressor® Slow release/Toprol XL 0 Nonselective (beta 1 = beta 2 ) Pindolol/Visken®+++ Propranolol/Inderal® Slow release/Inderal LA® 0 Nonselective alpha/beta blockers Carvedilol/Coreg®0 Labetolol/Normodyne® or Trandate®0 Clinical Pharmacology of Some Beta Blockers Adapted from Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 167

315
Therapeutic Uses of Beta- Adrenergic Blockers 315

316
Therapeutic Uses of Beta-Adrenergic Blockers 316 DrugHTNAnginaDysrrhy- thmias MIMigraineStage Fright Heart Failure Cardioselective AcebutololAIA AtenololAAIAII EsmololIA MetolprololAAIAIA Nonselective PindololAII PropranololAAAAAI Nonselective alpha/beta blockers CarvedilolAIAA LabetololA Adapted from Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p.168 A – approved; I - investigational

317
Sympatholytics Alpha-1 Antagonists 317

318
318 Sympatholytics Alpha-1 Antagonists Sites of Action Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 500

319
Alpha-1 Antagonists 319

320
Alpha-1 Antagonists 320 Doxazosin, terazosin, prazosin and others End in -azosin Block alpha-1 receptors on arterioles and veins prevent SNS-mediated vasoconstriction vasodilation peripheral resistance, venous return to heart Doxazosin, terazosin and tamsulosin (Flomax) used for BPH. May actually be used more frequently for this than for hypertension

321
Alpha-1 Antagonists Adverse Effects 321

322
Alpha-1 Antagonists Adverse Effects Not used as first line therapy for hypertension –Orthostatic hypotension is a big problem –Sexual side effects are big reasons for noncompliance 322

323
Centrally Acting Alpha-2 Agonists 323

324
324 Centrally Acting Alpha-2 Agonists Sites of Action Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 500

325
Centrally Acting Alpha-2 Agonists Clonidine Methyldopa (agent of choice for chronic hypertension in pregnancy – not for pre-eclampsia) – The only drug that is approved for hypertension in pregnancy Act within brainstem (alpha-2 receptors) to suppress sympathetic outflow to the heart and blood vessels → vasodilation, CO BP 325
 – The only drug that is approved for hypertension in pregnancy Act within brainstem (alpha-2 receptors) to suppress sympathetic outflow to the heart and blood vessels → vasodilation, CO BP 325")
326
Centrally Acting Alpha-2 Agonists Adverse Effects 326

327
Centrally Acting Alpha-2 Agonists Adverse Effects Dry mouth Sedation Hemolytic anemia Liver disorders Rebound hypertension if abruptly stopped – Could result in a stroke 327

328
Calcium Channel Blockers 328

329
Calcium Channel Blockers Dihydropyridines Non-dihydropyridines 329

330
Calcium Channel Blockers Dihydropyridines 330

331
Calcium Channel Blockers Dihydropyridines Nifedipine Amlodipine (Norvasc) Used for hypertension – Promote dilation of arterioles, little effect on veins 331
 Used for hypertension – Promote dilation of arterioles, little effect on veins 331")
332
Calcium Channel Blockers Non-dihydropyridines 332

333
Calcium Channel Blockers Non-dihydropyridines Verapamil, diltiazem Can be used for hypertension – Promote dilation of arterioles, little effect on veins Also act on heart to slow conduction and decrease contractility – May be good or bad 333

334
Calcium Channels in the Heart Diagram 334

335
335 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 481 Calcium Channels in the Heart Diagram

336
Calcium Channels in the Heart Description 336

337
Calcium Channels in the Heart Description NE – beta receptor – increased activity at calcium channels – heart – increased HR (SA node), conduction velocity (AV node), and contraction (myocardium) 337
, conduction velocity (AV node), and contraction (myocardium) 337")
338
Verapamil 338

339
Verapamil Blocks Ca +2 channels in arterioles, heart – Dilation of peripheral vessels BP – Dilation of coronary arteries coronary perfusion – Blockade at SA node HR – Blockade at AV node nodal conduction – Blockade in myocardium contractile force Indications – Angina pectoris, hypertension, dysrhythmias (A- fibrillation, PSVT) 339
 339")
340
Verapamil Adverse Effects 340

341
Verapamil Adverse Effects Constipation (why?) – Block calcium channels in the smooth muscle of the GI tract, leading to constipation Dizziness, facial flushing, headache, edema of ankles, feet (why?) – Because of the effect on veins Bradycardia, conduction defects (why?) – Due to effects on the heart rate 341
 – Block calcium channels in the smooth muscle of the GI tract, leading to constipation Dizziness, facial flushing, headache, edema of ankles, feet (why ) – Because of the effect on veins Bradycardia, conduction defects (why ) – Due to effects on the heart rate 341")
342
Nifedipine and Amlodipine (Dihydropyridines) 342
 342")
343
Nifedipine and Amlodipine (Dihydropyridines) Block Ca +2 channels in arterioles – Do not have the effects on the heart that verapamil does – Used mainly for hypertension – Dilation of peripheral vessels → BP – Dilation of coronary arteries → coronary perfusion Do NOT block cardiac Ca +2 channels at therapeutic doses 343
 Block Ca +2 channels in arterioles – Do not have the effects on the heart that verapamil does – Used mainly for hypertension – Dilation of peripheral vessels → BP – Dilation of coronary arteries → coronary perfusion Do NOT block cardiac Ca +2 channels at therapeutic doses 343")
344
Nifedipine and Amlodipine Indirect (Reflex) Effects 344
 Effects 344")
345
Nifedipine and Amlodipine Indirect (Reflex) Effects Lowering BP baroreceptor reflex → stimulate the medulla -- firing of SNS to beta receptors in the heart --- increased heart rate and increases contractility – Stimulating the heart may not be desirable in somebody with heart disease – Can use a beta blocker along with this in order to decrease heart rate But, nifedipine lacks direct cardiosuppressant actions, cardiac stimulation is unopposed → HR, contractility Net effect is the sum of the direct effect (vasodilation) and the indirect effect (reflex cardiac stimulation) 345
 Effects Lowering BP baroreceptor reflex → stimulate the medulla -- firing of SNS to beta receptors in the heart --- increased heart rate and increases contractility – Stimulating the heart may not be desirable in somebody with heart disease – Can use a beta blocker along with this in order to decrease heart rate But, nifedipine lacks direct cardiosuppressant actions, cardiac stimulation is unopposed → HR, contractility Net effect is the sum of the direct effect (vasodilation) and the indirect effect (reflex cardiac stimulation) 345")
346
Nifedipine and Amlodipine Uses 346

347
Nifedipine and Amlodipine Uses Angina pectoris – Vasospastic angina, angina of effort Hypertension – Essential hypertension – Nifedipine – only use sustained-release formulation for hypertension Take whole, do not crush or chew – Amlodipine has a longer half-life than nifedipine and does not have a sustained- release formulation 347

348
Nifedipine and Amlodipine Adverse Effects 348

349
Nifedipine and Amlodipine Adverse Effects Flushing, dizziness, headache, edema Gingival hyperplasia Constipation – This is a big deal – People have to be on a bowel regimen of stool softeners and fiber Do not exacerbate conduction abnormalities because they do not affect the conduction system of the heart Do cause reflex tachycardia → cardiac oxygen demand → angina – Give with a beta blocker to counteract this in patients with angina 349

350
Nifedipine blocks Ca +2 channels in arterioles. This results in: 350

351
Nifedipine blocks Ca +2 channels in arterioles. This results in: 1.Vasoconstriction of peripheral vessels 2.Vasoconstriction of coronary arteries 3.Decrease in HR 4.Dilation of peripheral vessels - Because you are blocking calcium channels, so contraction cannot occur 351

352
Hypertensive Emergencies 352

353
Hypertensive Emergencies (SBP >200 mm Hg or DBP >120 mm Hg) Symptoms of actual or impending end-organ damage – Neurological – Cardiovascular – Other 353
 Symptoms of actual or impending end-organ damage – Neurological – Cardiovascular – Other 353")
354
Hypertensive Emergencies Neurological Symptoms 354

355
Hypertensive Emergencies Neurological Symptoms Hypertensive encephalopathy - the brain does not work well, person is not oriented Cerebral vascular accident/cerebral infarction – May have an aortic dissection where the lining of the aorta separates from the other layers, preventing the blood from going forward Subarachnoid hemorrhage Intracranial hemorrhage 355

356
Hypertensive Emergencies Cardiological Symptoms 356

357
Hypertensive Emergencies Cardiological Symptoms Myocardial ischemia/infarction Acute left ventricular dysfunction Acute pulmonary edema Aortic dissection 357

358
Hypertensive Emergencies Other Symptoms 358

359
Hypertensive Emergencies Other Symptoms Acute renal failure/insufficiency Retinopathy Eclampsia Microangiopathic hemolytic anemia 359

360
Sodium Nitroprusside-Nitropress 360

361
Sodium Nitroprusside-Nitropress® A very powerful arterial vasodilator No reflex tachycardia Overshoot hypotension is possible but can be correctly quickly by stopping or slowing the infusion Titrate to blood pressure – An infusion pump is essential. An arterial line or an automatic blood pressure cuff must be used to check BP continuously. 361

362
Sodium Nitroprusside-Nitropress Adverse Effects 362

363
Sodium Nitroprusside-Nitropress Adverse Effects Cyanide poisoning Thiocyanate Toxicity 363 Lehne, 2009, Pharmacology for Nursing Care, 7 th ed., Elsevier, p. 492

364
Adverse Effects Cyanide Poisoning 364

365
Adverse Effects Cyanide Poisoning Likely in patients with liver disease Avoid prolonged rapid infusion because of the risk of cyanide poisoning 365

366
Adverse Effects Thiocyanate Toxicity 366

367
Adverse Effects Thiocyanate Toxicity Likely when drug given over days CNS effects (disorientation, delirium) Avoid infusions > 3 days; monitor plasma thiocyanate 367
 Avoid infusions > 3 days; monitor plasma thiocyanate 367")
368
IV Calcium Channel Blockers 368

369
IV Calcium Channel Blockers Can be used for hypertensive emergencies Fenoldepam – long half-life Nicardipine – long half life Clevidipine – short half-life, easy to titrate Titrate similarly to sodium nitroprusside All can cause reflex tachycardia and hypotension. 369

370
How do diuretics decrease blood pressure? 370

371
How do diuretics decrease blood pressure? 1.Block beta adrenergic receptors – beta blockers 2.Inhibit angiotensin converting enzyme – ACE inhibitors 3.Act on renal tubules to promote water excretion 4.Act as a vasodilator 371

372
DISORDERS OF ARTERIAL CIRCULATION Hyperlipidemia Leading to Atherosclerosis 372

373
Types of Biological Lipids 373

374
Types of Biological Lipids Triglycerides, phospholipids, cholesterol classified as lipids Lipids are chemical substances that are insoluble in water but soluble in alcohol. Three types of biological lipids Triglycerides Used as sources for energy metabolism Phospholipids Structural components of lipoproteins, clotting components, myelin sheath, cell membranes Cholesterol Basis of steroid hormones and an important cell membrane component 374

375
Lipoproteins 375

376
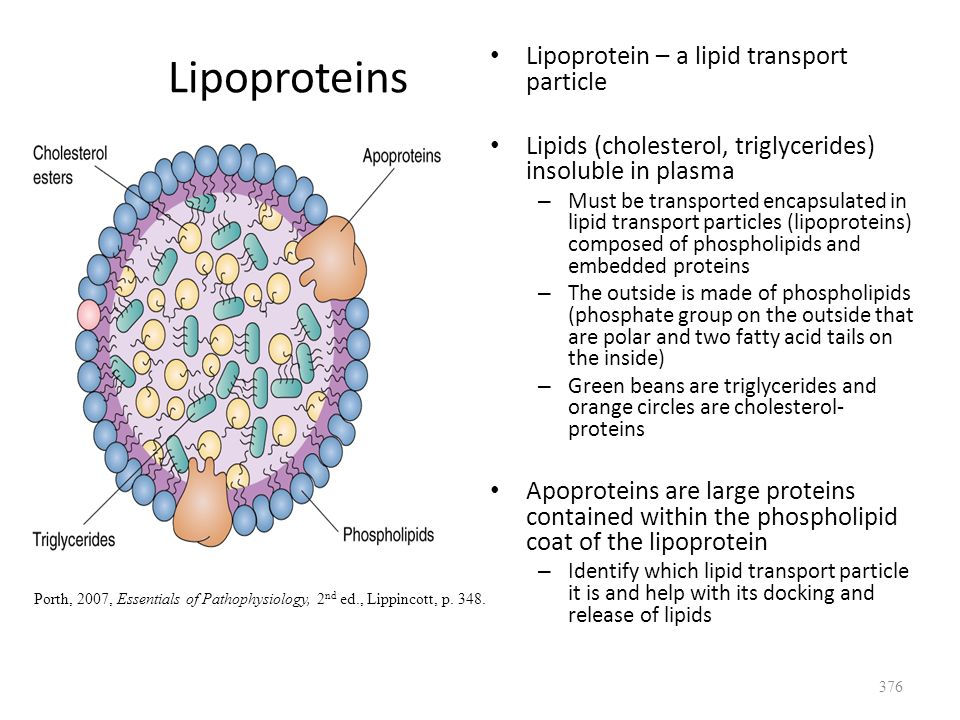
Lipoproteins Lipoprotein – a lipid transport particle Lipids (cholesterol, triglycerides) insoluble in plasma – Must be transported encapsulated in lipid transport particles (lipoproteins) composed of phospholipids and embedded proteins – The outside is made of phospholipids (phosphate group on the outside that are polar and two fatty acid tails on the inside) – Green beans are triglycerides and orange circles are cholesterol- proteins Apoproteins are large proteins contained within the phospholipid coat of the lipoprotein – Identify which lipid transport particle it is and help with its docking and release of lipids 376 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 348.
377
Types of Lipoproteins Description 377

378
Types of Lipoproteins Description Of the five types of lipoproteins, LDLs and HDLs are the most important As the density of the lipoprotein increases, the proportion of triglycerides decreases and the proportion of cholesterol increases (except LDLs have more cholesterol than HDLs) Chylomicrons Come from the GI tract Dietary lipids VLDL Smaller, heavier, more compact, circulate in the blood LDL Smaller, more compact, heavier, circulate HDL Smaller, most compact and dense 378
 Chylomicrons Come from the GI tract Dietary lipids VLDL Smaller, heavier, more compact, circulate in the blood LDL Smaller, more compact, heavier, circulate HDL Smaller, most compact and dense 378")
379
Types of Lipoproteins 379 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 348.

380
Lipoprotein Synthesis and Transport Description 380

381
Lipoprotein Synthesis and Transport Description Synthesized in small intestine, liver Liver is important in LDL metabolism – Removes LDL via LDL receptors – Place where the HDLs bring the lipids back Lipids are transported all over the body Chylomicrons in the liver are changed into VLDLs and then into LDLs Circulating to body tissues HDLs are bringing the lipids back to the liver 381

382
Lipoprotein Synthesis and Transport 382 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 349.

383
HDL 383

384
HDL “Good cholesterol” Carries cholesterol FROM tissues back TO the liver – This is why there are good Prevent atherosclerosis High HDL prevents atherosclerosis – HDLs are scavengers, picking up cholesterol from deposits in the arteries and bringing it back to the liver for disposal HDL inhibits uptake of LDLs into cells Heredity, exercise, moderate ETOH (1-2 drinks per day for women) HDLs Smoking, diabetes or metabolic syndrome (sort of a diabetic prodrome) HDLs 384
 HDLs Smoking, diabetes or metabolic syndrome (sort of a diabetic prodrome) HDLs 384")
385
LDL 385

386
LDL “bad cholesterol” Familial defects in LDL receptor – “familial hypercholesterolemia” – Inadequate, or defective hepatic uptake of LDL circulating LDL – Have heart attacks and strokes at very early ages “Receptor disease” 386

387
LDL Receptors in Liver Remove LDLs from the Blood 387

388
LDL Receptors in Liver Remove LDLs from the Blood 388 Robbins & Cotran Pathologic Basis of Disease (7th ed), 2005, Elsevier, p.158
, 2005, Elsevier, p.158")
389
Hypercholesterolemia 389

390
Hypercholesterolemia 390 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 350. Xanthomas (deposits of cholesterol) develop in certain areas, including the knuckles. - Not very common
 develop in certain areas, including the knuckles. - Not very common.")
391
Hypercholesterolemia Primary 391

392
Hypercholesterolemia Primary Develops independent of other causes Defective synthesis of apoproteins Lack of receptors Defective receptors Defects in handling of cholesterol in cell that are genetically determined Familial hypercholesteremia 392

393
Hypercholesterolemia Secondary 393

394
Hypercholesterolemia Secondary Associated with other health problems and behaviors (high fat diet, obesity, diabetes mellitus) 394
 394")
395
Diagnosis Screening 395

396
Diagnosis Screening All adults 20 years of age and older should have a fasting lipoprotein profile done every 5 years – Total cholesterol, LDL, HDL, TG 396 See Porth, text on page 350-351 for specific recommendations Also Table 49.4 in Lehne

397
Classification of LDL, Total, and HDL Cholesterol 397

398
Classification of LDL, Total, and HDL Cholesterol Cholesterol Level (mg/dL) Classification HDL cholesterol <40Low >60High 398 Cholesterol Level (mg/dL) Classification Total <200Optimal 200-239Borderline high >240High LDL cholesterol <100Optimal 100-129Above optimal 130-159Borderline high 160-189High >190Very high Adapted from Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 350.

399
Why are Increased Blood Lipids so Bad? 399

400
Why are Increased Blood Lipids so Bad? Increased blood lipids, particularly cholesterol, increase the risk of a vascular disease called atherosclerosis. – Fatty deposits form in arterial walls This increases the risk of clot formation and occlusion of an artery. – Occluded arteries cause myocardial infarctions, stroke, and peripheral vascular disease, which may lead to necrosis of part of the extremity. Atherosclerosis leads to arteriosclerosis (hardening of the arteries) caused by calcium deposits in the walls of the arteries – Increases the risk of aneurysms and other vessel wall problems. 400
 caused by calcium deposits in the walls of the arteries – Increases the risk of aneurysms and other vessel wall problems")
401
Atherosclerosis 401

402
Atherosclerosis Atheros (glue/paste) Sclerosis (hardening) Formation of fibrofatty lesions (atheromas) in the intimal lining of large and medium sized arteries (aorta, coronaries, carotids, and many others) – Not present in the veins 402
 Sclerosis (hardening) Formation of fibrofatty lesions (atheromas) in the intimal lining of large and medium sized arteries (aorta, coronaries, carotids, and many others) – Not present in the veins 402")
403
Atherosclerotic Lesions 403

404
Atherosclerotic Lesions Fatty streak – Thin, flat, yellow discolorations that progressively enlarge by becoming thicker and more elevated. Present in children. Precursors to atheromata Atheroma Fibrous plaque – Increases in smooth muscle and collagen Complicated lesions – A complicated lesion has a lot of smooth muscle vessels that have proliferated – Macrophages eat up the lipids – This type of lesion can serve as the focus of a clot and represents a weakness in the artery that may cause problems – Characterized by thrombosis, fissure, and hematoma formation 404

405
Atheromatous Plaque 405

406
406 Atheromatous Plaque Porth, 2007, Essential of Pathophysiology, 2 nd ed., Lippincott, p. 353 PlaqueComplicated Lesion

407
Definitions Thrombus, Embolus, Stenosis, Mural 407

408
Definitions Thrombus, Embolus, Stenosis, Mural Thrombus = clot Embolus = a clot that breaks off from its initial location and travels through the vascular system. Stenosis = narrowing or closing off of a vessel (or a heart valve). Mural = wall (a mural thrombus is a clot in the wall of a vessel or a chamber of the heart) 408
. Mural = wall (a mural thrombus is a clot in the wall of a vessel or a chamber of the heart) 408.")
409
Atherosclerosis Timeline 409

410
410

411
Progression of Atherosclerosis 411

412
412 Robbins & Cotran Pathologic Basis of Disease (7th ed), Elsevier, 2005, p.517
, Elsevier, 2005, p.517")
413
Atheromatous Lesion Diagram 413

414
414

415
Atheromas 415

416
416 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 352. Atheromas tend to develop at sites of turbulent flow – near branch points and arteries As the artheroma develops, it creates more of a constriction, which produces more turbulent flow and more atheromas. See Figure 17.8 in Porth!

417
Laminar and Turbulent Flow 417

418
Laminar and Turbulent Flow 418 Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 323.
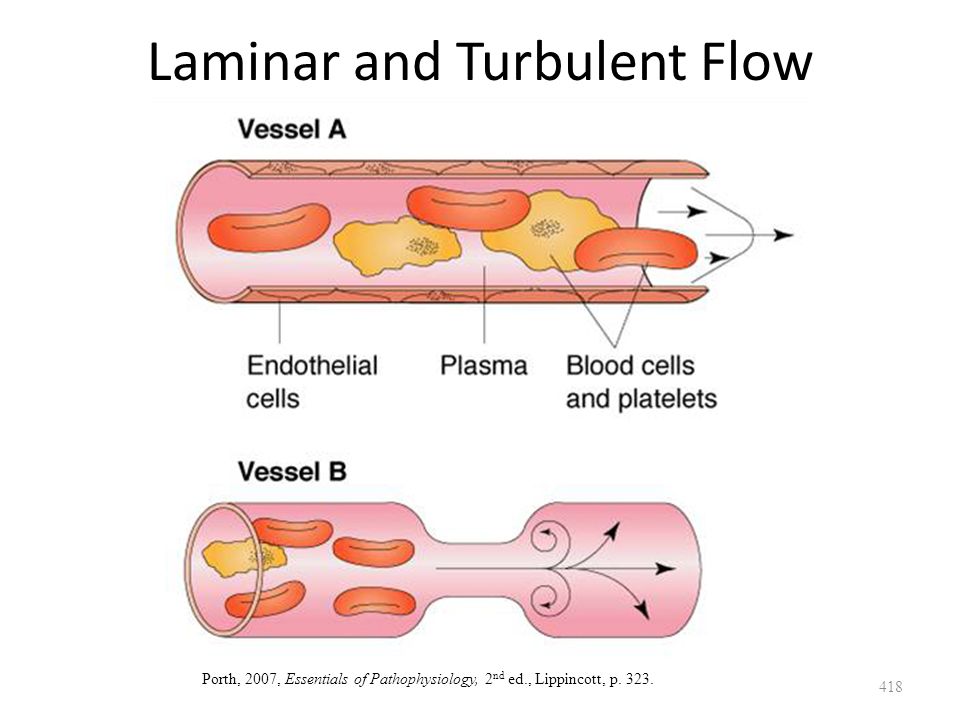
419
Lifestyle Risk Factors for Atherosclerosis 419

420
Lifestyle Risk Factors for Atherosclerosis Many people have more than one of these risk factors Age – Men > 45 y.o.; women > 55 y.o. (or premature menopause) Removing ovaries at an earlier age, will accelerate women’s risk of atherosclerosis Family History – MI before 55 y.o. in father or before 65 y.o. mother Current cigarette smoking – If you stop smoking, the risk decreases quickly Hypertension (BP > 140/90) Hyperlipidemia – Low HDL (< 40 mg/dL) – High LDL Diabetes mellitus 420
 Removing ovaries at an earlier age, will accelerate women’s risk of atherosclerosis Family History – MI before 55 y.o. in father or before 65 y.o. mother Current cigarette smoking – If you stop smoking, the risk decreases quickly Hypertension (BP > 140/90) Hyperlipidemia – Low HDL (< 40 mg/dL) – High LDL Diabetes mellitus 420.")
421
Risk Factors Markers 421

422
Risk Factors Markers C-reactive protein (CRP) – Marker of inflammation; may be a better than LDL? – Not very specific because you can have inflammation for many different reasons Homocysteine – Inhibits coagulation, causes endothelial damage, important in initial phases? – It is good to be elevated and bad to be low – Not a great predictor of athlerosclerosis Serum lipoprotein (a) – Part of the LDL; promotes foam cells – If it is elevated, it is a risk factor Infectious agents – Chlamydia pneumoniae 422
 – Part of the LDL; promotes foam cells – If it is elevated, it is a risk factor Infectious agents – Chlamydia pneumoniae 422.")
423
Clinical Manifestations of Vascular Disease 423

424
Clinical Manifestations of Vascular Disease 424 Cotran (1999) pg. 499
 pg. 499")
425
Management of Hyperlipidemia 425

426
Management of Hyperlipidemia Reduction in LDL is primary target for cholesterol-lowering therapy, particularly for people at risk for CHD* – It is not as easy to raise the HDL as it is to lower the LDL – Age, family history of premature CHD, cigarette smoker, hypertension, low HDL, diabetes mellitus Some evidence that when lipids are lowered, at least with statin drugs, that atheromatous changes regress. – This is a very good thing Dietary changes* – calories, saturated fats, cholesterol Lifestyle changes – physical activity, smoking cessation, weight loss Pharmacologic treatment 426 *See Porth, Table 17-1, page 351 and Lehne, Table 49-4, p. 551 * See Lehne, Table 49-6, pg. 556

427
Lipid-Lowering Drugs Diagram 427

428
428 Lipid-Lowering Drugs Diagrams Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 349.

429
Mechanisms of Lipid-Lowering Drugs 429

430
Mechanisms of Lipid-Lowering Drugs Mechanisms: 1.Affect cholesterol production by the liver 2.Remove cholesterol from bloodstream 3. LDL receptors 4. Cholesterol absorption from intestine 5. intravascular conversion of VLDL and IDL to LDL 430

431
Classes of Drugs Used in Treatment of Hypercholesterolemia 431

432
Classes of Drugs Used in Treatment of Hypercholesterolemia HMG-CoA reductase inhibitors (statins) Bile acid-binding resins Cholesterol absorption inhibitor agents Niacin and its congeners Fibric acid derivatives 432
 Bile acid-binding resins Cholesterol absorption inhibitor agents Niacin and its congeners Fibric acid derivatives 432")
433
Types of Statins 433

434
Types of Statins All end in -statin Atorvastatin [Lipitor] Fluvastatin [Lescol] Lovastatin [Mevacor] - generic Provastatin [Pravachol] Rosuvastatin [Crestor] Simvastatin [Zocor] - generic 434
![Types of Statins All end in -statin Atorvastatin [Lipitor] Fluvastatin [Lescol] Lovastatin [Mevacor] - generic Provastatin [Pravachol] Rosuvastatin [Crestor] Simvastatin [Zocor] - generic 434](http://images.slideplayer.com/33/6551720/slides/slide_434.jpg "Types of Statins All end in -statin Atorvastatin [Lipitor] Fluvastatin [Lescol] Lovastatin [Mevacor] - generic Provastatin [Pravachol] Rosuvastatin [Crestor] Simvastatin [Zocor] - generic 434")
435
Statins Beneficial Actions 435

436
Statins Beneficial Actions Reduce cholesterol synthesis in liver LDL receptors (most important) – LDLs from the circulation, which is desirable HDLs TG 436
 – LDLs from the circulation, which is desirable HDLs TG 436")
437
Statins Timing 437

438
Statins Timing Results within 2 weeks; maximal 4-6 weeks If drug is stopped, serum cholesterol returns to pretreatment levels (lifelong treatment), unless the person has lost substantial weight 438
, unless the person has lost substantial weight 438")
439
Statins LDL Receptors in Liver -> LDLs 439

440
Statins LDL Receptors in Liver -> LDLs 440 Robbins & Cotran Pathologic Basis of Disease (7th ed), 2005, Elsevier, p.158
, 2005, Elsevier, p.158")
441
Statins Actions 441

442
Statins Actions Cardiovascular actions – Reduce inflammation at plaque sites – Improve endothelial cell function – Enhance blood vessel dilation – Reduce the risk of thrombosis Increased bone formation – Enhance osteoblast activity risk of osteoporosis and fractures 442

443
Statins Therapeutic Uses 443

444
Statins Therapeutic Uses Hypercholesterolemia Prevention of cardiovascular events – MI, stroke, angina Diabetes – ADA: Pts > 40 y.o. with total cholesterol > 135 mg/dL- regardless of LDL – ACP: All pts with type 2 diabetes with coronary artery disease, even if they don’t have high cholesterol; all adults with type 2 diabetes plus one CV risk factor - even if they don’t have high cholesterol 444

445
Statins Side Effects 445

446
Statins Side Effects Myopathy (inflammation of the muscle)/rhabdomyolysis (total muscle breakdown) – Report unexplained muscle weakness, tenderness – Rhabdomyolysis can be fatal – Rosuvastatin higher risk Hepatotoxicity – Monitor liver enzymes every 6-12 months – Avoid use for patients with viral or alcoholic hepatitis 446
/rhabdomyolysis (total muscle breakdown) – Report unexplained muscle weakness, tenderness – Rhabdomyolysis can be fatal – Rosuvastatin higher risk Hepatotoxicity – Monitor liver enzymes every 6-12 months – Avoid use for patients with viral or alcoholic hepatitis 446")
447
Statins Drug Interactions 447

448
Statins Drug Interactions Fibrates and ezetimibe – Also cholesterol, so their activity might be additive to statins – Can also cause myopathy, so the danger from that would also be increased Inhibitors of cytochrome P450 like ketoconazole, erythromycin, HIV protease inhibitors, etc., inhibit the metabolism of statins and raise blood levels risk of adverse effect 448

449
Bile Acid Sequestrants 449

450
Bile Acid Sequestrants Cholestyramine, colestipol, and colesevelam Biologically inert, insoluble in water, cannot be absorbed from GI tract, simply pass through intestine, excreted in feces 450

451
Bile Acid Sequestrants Actions 451

452
Bile Acid Sequestrants Actions Absorb bile acids in the intestine and keep them from being reabsorbed into the bloodstream. – New bile acids must be synthesized, which requires cholesterol. – LDLs are internalized into liver cells as a source of cholesterol. – This lowers LDLs. Reduce LDL cholesterol – Maximal reduction within one month (20%) – LDL levels return to pre-treatment levels when drug is discontinued 452
 – LDL levels return to pre-treatment levels when drug is discontinued 452.")
453
Bile Acid Sequestrants Diagram 453

454
454 Bile Acid Sequestrants Diagram Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 349. Prevent the absorption of cholesterol in the intestine

455
Bile acid reabsorption (GI) synthesis in liver need for cholesterol LDL receptors 455
 synthesis in liver need for cholesterol LDL receptors 455")
456
456 Bile acid reabsorption (GI) synthesis in liver need for cholesterol LDL receptors Robbins & Cotran Pathologic Basis of Disease (7th ed), 2005, Elsevier, p.158
 synthesis in liver need for cholesterol LDL receptors Robbins & Cotran Pathologic Basis of Disease (7th ed), 2005, Elsevier, p.158")
457
Bile Acid Sequestrants Therapeutic Use 457

458
Bile Acid Sequestrants Therapeutic Use Reduce LDL cholesterol – Drug plus diet -> LDL by 15-30% Usually combined with statin – LDL by 50% 458

459
Bile Acid Sequestrants Adverse Effects 459

460
Bile Acid Sequestrants Adverse Effects Devoid of systemic effects because they are not absorbed GI symptoms (except colesevelam) because it swells up in the GI tract (drink it) – Constipation – Bloating – Indigestion – Nausea 460
 because it swells up in the GI tract (drink it) – Constipation – Bloating – Indigestion – Nausea 460")
461
Bile Acid Sequestrants Drug Interactions 461

462
Bile Acid Sequestrants Drug Interactions Cannot take a lot of medications because it will absorb medications and keep them from being absorbed Decreased absorption of: – Warfarin-Acetaminophen – Thiazides-Beta blockers – Digoxin-Corticosteroids – Iron-Thyroid hormones – Fat-soluble vitamins A, D, E, and K (except colesevelam) – Take oral medications 1 hour before or 4 hours after the bile acid sequestrant. 462

463
Cholesterol Absorption Inhibitors Ezetimibe (Zetia®) 463
 463")
464
Ezetimibe (Zetia®) Mechanism of Action 464
 Mechanism of Action 464")
465
Ezetimibe (Zetia®) Mechanism of Action Mechanism of action Acts on cells in the brush border of the intestine and inhibits cholesterol absorption – Does not actually absorb the cholesterol like the previous drug Blocks absorption of dietary cholesterol and cholesterol secreted in bile Lowers total cholesterol, LDLs, TG and raises HDLs 465
 Mechanism of Action Mechanism of action Acts on cells in the brush border of the intestine and inhibits cholesterol absorption – Does not actually absorb the cholesterol like the previous drug Blocks absorption of dietary cholesterol and cholesterol secreted in bile Lowers total cholesterol, LDLs, TG and raises HDLs 465")
466
Ezetimibe (Zetia®) Use 466
 Use 466")
467
Ezetimibe (Zetia®) Use Used as adjunct to diet modification Can be used as monotherapy or with a statin – Recent evidence that the combo of ezetimibe and simvastin (Vytorin) actually worsened plaques rather than making them better. 467

468
Ezetimibe (Zetia) Drug Interactions 468
 Drug Interactions 468")
469
Ezetimibe (Zetia) Drug Interactions Statins - risk of liver damage Fibrates – both the concentration of cholesterol in the bile the risk of gallstones, which is precipitated solid cholesterol Bile-acid sequestrants- impair the absorption of ezetimibe Cyclosporine- inhibits metabolism of ezetimibe its concentration. 469

470
Nicotinic Acid (Niacin) [Niacor, Niaspan] 470
![Nicotinic Acid (Niacin) [Niacor, Niaspan] 470](http://images.slideplayer.com/33/6551720/slides/slide_470.jpg "Nicotinic Acid (Niacin) [Niacor, Niaspan] 470")
471
471 Nicotinic Acid (Niacin) [Niacor, Niaspan] Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 349. Decreases production of VLDLs by inhibiting lipolysis in adipose tissue LDL
![471 Nicotinic Acid (Niacin) [Niacor, Niaspan] Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p.](http://images.slideplayer.com/33/6551720/slides/slide_471.jpg "349. Decreases production of VLDLs by inhibiting lipolysis in adipose tissue LDL.")
472
Nicotinic Acid (Niacin) 472
 472")
473
Nicotinic Acid (Niacin) Effect on plasma lipoproteins: – Reduces triglycerides (20 – 50%) and LDLs (5-25%) – Raises HDLs (15-35%) – Drug of choice to lower triglyceride levels in patients at risk for pancreatitis. – More effective when combined with statin – Triple therapy (nicotinic acid, statin, bile-acid sequestrant) LDL 70% Nicotinic acid is also a B-vitamin, but doses as a vitamin are much smaller than as a lipid-lowering drug. 473
 LDL 70% Nicotinic acid is also a B-vitamin, but doses as a vitamin are much smaller than as a lipid-lowering drug")
474
Nicotinic Acid Adverse Effects 474

475
Nicotinic Acid Adverse Effects Intense flushing of the head and neck in nearly all patients– diminishes in several weeks, attenuated with aspirin GI upset – take with food Hepatotoxic – follow liver enzymes Raises blood levels of homocysteine, a substance thought to increase cardiovascular risk. To counteract this, add folic acid supplements. Hyperglycemia – use with caution in diabetics 475

476
Fibric Acid Derivatives (Fibrates) 476
 476")
477
477 Fibric Acid Derivatives (Fibrates) Porth, 2007, Essentials of Pathophysiology, 2 nd ed., Lippincott, p. 349. -Gemfibrozil [Lopid] -Fenofibrate [Tricor] 1.Increase lipoprotein lipase → VLDLs and TG storage in adipose tissue ( serum TG) 2.Also HDL 3.No effect on LDL
 2.Also HDL 3.No effect on LDL.")
478
Fibric Acid Derivatives Adverse Effects 478

479
Fibric Acid Derivatives Adverse Effects Gallstones – Increase biliary cholesterol saturation → increase risk of gallstones Myopathy – like the statins, can cause myopathy Hepatotoxicity – like the statins, fibric acid derivatives are hepatotoxic; Monitor liver enzymes Because of overlapping adverse effects, the combo of a statin and a fibric acid derivative should be used with great caution. Pregnancy category C 479

480
Fibric Acid Derivatives Drug Interactions 480

481
Fibric Acid Derivatives Drug Interactions Warfarin – Gemfibrozil increases the efficacy of warfarin by displacing it from protein binding sites. – Follow INR closely Use with caution in statins because of the increase in risk of myopathy 481

482
Which of the following drugs are insoluble in water, cannot be absorbed from the GI tract and pass through the intestine? 482

483
Which of the following drugs are insoluble in water, cannot be absorbed from the GI tract and pass through the intestine? 1.Bile acid sequestrants 2.HMG Co-A reductase inhibitors 3.Fibric acid derivatives 4.Nicotinic acid 483

484
Which of the following drug classes has been shown to reverse atherosclerotic changes? 484

485
Which of the following drug classes has been shown to reverse athrosclerotic changes? 1.Statins 2.Fibric acid derivatives 3.Bile acid sequestrants 4.Niacin 485

486
Questions? 486

Similar presentations



















