Download presentation
Presentation is loading. Please wait.

2
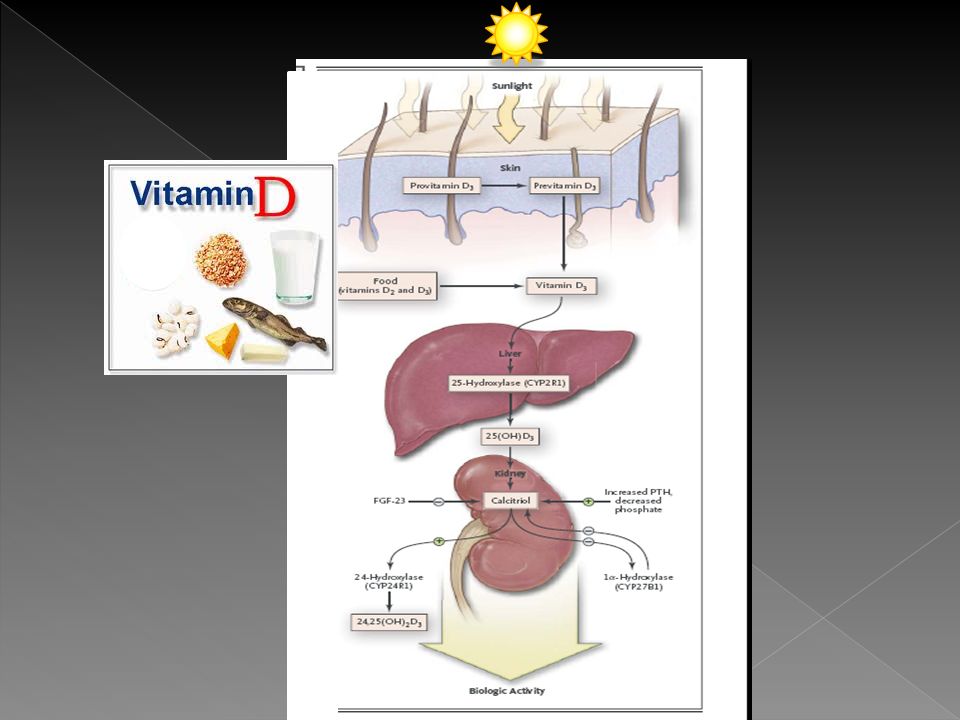
Hormone: › from Greek “impetus” chemical released by a cell that affect cells in other parts › is a chemical released by a cell in one part of an organism, that sends out messages that affect cells in other parts of the organism Vitamin: external source, food › essential organic micronutrient that can only be obtained from an external source, food

4
25(OH)D or calcidiol › Inactive form › 2-3 week ½-life › Major circulating form of Vitamin D › best indicator of status 1,25(OH) 2 D or calcitriol › Active form › 4 hour ½-life › Regulated by serum levels of PTH, Ca, PO4 › Levels normal or elevated in 2’hyperPTH › Does not reflect Vitamin D stores
D or calcidiol › Inactive form › 2-3 week ½-life › Major circulating form of Vitamin D › best indicator of status 1,25(OH) 2 D or calcitriol › Active form › 4 hour ½-life › Regulated by serum levels of PTH, Ca, PO4 › Levels normal or elevated in 2’hyperPTH › Does not reflect Vitamin D stores")
5
Vitamin D status by blood levels of 25(OH)D Vitamin D status25(OH)D ng/mL Sufficient ≥ 30 Insufficient 20 to 29 Optimal30-60 Side effects 88 Moyad, MA. (2008). Vitamin d: a rapid review. Urol Nurs, Oct 28(5), 343-349. Potentially harmful/ intoxication >150 Holick MF. (2007). Vitamin d deficiency. NEJM, 357(3), 266–80.
. Vitamin d: a rapid review. Urol Nurs, Oct 28(5), Potentially harmful/ intoxication >150 Holick MF. (2007). Vitamin d deficiency. NEJM, 357(3), 266–80..")
6
Adults: INSUFFICIENT/DEFICIENT: 11-50% of healthy adults Age, season, location Peds/Adolescents: › INSUFFICIENT: 61% › DEFICIENT: 9% Kumar, et al. (2009). Prevalence and Associations of 25-Hydroxyvitamin D Deficiency in US Children: NHANES 2001-2004 Pediatrics, 124(3), 362-370. Tangpricha, V. et al. (2002). Vitamin d insufficiency among free-living healthy young adults. Am J Med., 112(8), 659-62.
. Prevalence and Associations of 25-Hydroxyvitamin D Deficiency in US Children: NHANES Pediatrics, 124(3), Tangpricha, V. et al. (2002). Vitamin d insufficiency among free-living healthy young adults. Am J Med., 112(8),")
7
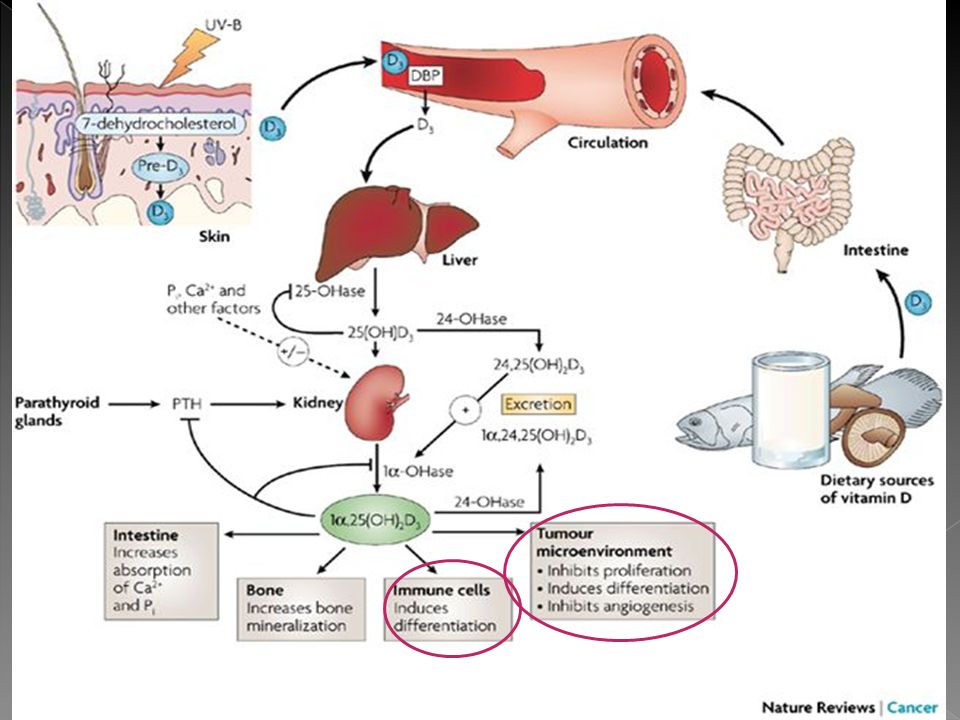
Reduces intestinal absorption of calcium and phosphorus; increases PTH Secondary Hyperparathyroidism: mineralization defect Osteopenia/Osteoporosis Low skeletal calcium Rickets/Osteomalacia Low phosphorus Muscle weakness Standing/walking/falls

9
› Cancer › CV disease › Diabetes › Autoimmune disorders › Infectious Diseases › more

10
IOM: › At least 14 scientists, broad range expertise › Assisted by experienced IOM staff members › Public input Endo Soc Task Force: › Dr Michael Holick, MD › 6 additional experts › 1 methodologist › Medical writer › Member review

11
IOM Prevalence OVERESTIMATED Potential harm from overtreatment ENDO SOC Prevalence UNDERESTIMATED, everyone at risk IOM report is a POPULATION model, not intended to direct treatment Both agree that there is NOT ENOUGH DATA to support beyond BONE HEALTH

13
Biomarker of EXPOSURE › Reflection of SUPPLY › use to evaluate INTAKE Biomarker of EFFECT › Using level as CAUSE and/or PREDICTOR for health outcomes

14
Factors Affecting Vitamin D levels: › Diet intake (food/supplements) › Dose size/frequency › Sun exposure Time of day, season, skin pigment, latitude, sunscreen use, clothing, pollution, cloud cover, altitude › Adiposity › Ancestry, especially African
 › Dose size/frequency › Sun exposure Time of day, season, skin pigment, latitude, sunscreen use, clothing, pollution, cloud cover, altitude › Adiposity › Ancestry, especially African")
15
PTH is inconsistent marker › Affected by renal function, exercise level, time of day, diet › No consensus of optimal level to reduce PTH or to prevent rise The interrelation of Vitamin D & calcium › Can we truly separate/differentiate?

16
Assay used › Different types of assays Radioimmunoassay high-performance liquid chromatography liquid chromatography tandem mass spectroscopy › What is being measured? › Results not standardized, different parameters of “normal” 20-100 ng/mL

17
No systematic, evidenced-based process currently exists for determining 25(OH)D cut points that clearly define Vitamin D DEFICIENCY › Use of higher than appropriate cut points will artificially increase the estimated prevalence of Vitamin D deficiency and increase the risk for harm.
D cut points that clearly define Vitamin D DEFICIENCY › Use of higher than appropriate cut points will artificially increase the estimated prevalence of Vitamin D deficiency and increase the risk for harm.")
18
Based on the available data …

19
Scientifically proven, cause-effect relationship: SKELETAL HEALTH

20
INSTITUTE OF MEDICINE 2010 Sufficient: ~ 20 (97.5%) Insufficient: 12 - < 20 Deficient: < 12 SEs/toxicity/pot harm: > 50 >30 is NOT consistently associated with increased benefits U-shaped curve ENDOCRINE SOCIETY 2011 Sufficient: ≥ 30 Insufficient: 20-29 Deficient: <20 Optimal: 40-60
 Insufficient: 12 - < 20 Deficient: < 12 SEs/toxicity/pot harm: > 50 >30 is NOT consistently associated with increased benefits U-shaped curve ENDOCRINE SOCIETY 2011 Sufficient: ≥ 30 Insufficient: Deficient: <20 Optimal: 40-60")
21
0-12 months: 400 IU 1 year -70 years: 600 IU >70 years: 800 IU Pregnant/breastfeeding: 600 IU

22
0-12 months: ≥400 IU 1-18 yrs: ≥ 600 IU (1000) ≥19 yrs: ≥ 1000 IU (1500-2000) Pregnant/breastfeeding: ≥ 1000 IU (≥ 1500)
 ≥19 yrs: ≥ 1000 IU ( ) Pregnant/breastfeeding: ≥ 1000 IU (≥ 1500)")
23
Selected food sources of vitamin D Food Sources Vitamin D (IU) 1 Egg 20 Salmon, 3.5 ounces 360 farmed 1000 wild Mackerel, 3.5 ounces 345 Tuna, canned, 3.5 ounces 200 Mushrooms, 100 gm 100 Milk, fortified, 8 ounces100 Breakfast cereals, fortified, 1 serving40–100 Orange juice, fortified, 8 ounces100 Source: Office of Dietary Supplements, National Institutes of Health
 1 Egg 20 Salmon, 3.5 ounces 360 farmed 1000 wild Mackerel, 3.5 ounces 345 Tuna, canned, 3.5 ounces 200 Mushrooms, 100 gm 100 Milk, fortified, 8 ounces100 Breakfast cereals, fortified, 1 serving40–100 Orange juice, fortified, 8 ounces100 Source: Office of Dietary Supplements, National Institutes of Health")
24
Arms and legs for 5-30 minutes › Depends on time of day, season, pigmentation, latitude 10 am – 3 pm Twice a week 20,000 IU Tanning beds SKIN CANCER RISK!

25
Daily Dosage (IU)Expected serum level increase after 3 months (ng/mL) 1001 2002 4004 8008 1,00010 2,00020 D3 preferred (chemically similar, more effective) BUT D2 is acceptable Fat soluble, take with meal/snack containing fat
Expected serum level increase after 3 months (ng/mL) , ,00020 D3 preferred (chemically similar, more effective) BUT D2 is acceptable Fat soluble, take with meal/snack containing fat")
26
0-18 yrs › 2000 IU/day or 50K IU/week x 6 weeks >18 yrs: › 6000 IU/day or 50K IU/week x 8 weeks Obese, malabsorption, meds › 2-3x MORE › 4000-10,000 IU/day

27
Elderly Reduced sun exposure › Darker Skin › Institutionalized/Homebound › Sunscreeen use Breastfed infants Renal & Liver Disease GBP/malabsorption Drugs (PTN, phenobarb, glucocorticoids, etc) Overweight/obese ALMOST EVERYONE SHOULD BE SCREENED!
 Overweight/obese ALMOST EVERYONE SHOULD BE SCREENED!")
29
Large-scale, RCT Health outcomes/related conditions Adverse effects/toxicity/safety Physiology and molecular pathways Synthesis of evidence and research methodology Dose-response relationships Sun exposure Intake assessments (assays)
")
30
Until then …

31
Counsel patients › Not to self-treat › Take per your CLEAR instructions › Limited supplies, no automatic refills › Careful with calcium intake Monitor › Labs periodically After 6-8 weeks therapy Seasonal late fall/early winter

Similar presentations