Download presentation
Presentation is loading. Please wait.

1
Shahla Chaichian Associate Professor of Ob& Gyn Fellowship of Gynecology Laparoscopy Deputy director of minimally invasive surgery research center of IUMS

2
Surgical approaches to ovulation induction have developed from the traditional wedge resection in 30 th decade by Stein& lovental to modern day minimal access techniques, usually employing laparoscopic ovarian diathermy or laser. Multiple ovarian puncture performed either by diathermy or by laser is known as ‘‘ovarian drilling’’ Gjonnaess H. Polycystic ovarian syndrome treated by ovarian electrocautery through the laparoscope. Fertil Steril 1984;41:20–5.

3
The main indication for performing LOS is CC resistance. The surgery also may be recommended for persistently LH hypersecretion, either during natural cycles or in response to CC, because it may reduce LH secretion. In addition, LOS may be useful in women with PCOS who need laparoscopic assessment of their pelvis or who live too far away from the hospital for the intensive monitoring required during gonadotropin therapy.

4
Extensive ovarian diathermy is not indicated to prevent hyper responsiveness to exogenous gonadotropins (115). In addition, ovarian surgery has been suggested for non fertility indications such as management of menstrual irregularity or hyperandrogenism. Because of the inherent risks of LOS and the lack of long-term evidence from RCTs, it cannot be recommended in these circumstances (116).
..")
5
Commonly employed methods for LOS include monopolar electrocautery (diathermy) and laser. There does not appear to be a difference in outcomes between the two modalities (117). Ovarian surgery may also be performed transvaginally by hydrolaparoscopy (118), but no large RCTs are yet available. It has been proposed that the degree of thermal stromal damage should be determined by the size of the ovary (119).
. Ovarian surgery may also be performed transvaginally by hydrolaparoscopy (118), but no large RCTs are yet available. It has been proposed that the degree of thermal stromal damage should be determined by the size of the ovary (119)..")
6
There is no evidence that any surgical technique is superior, but as few as four punctures have been shown to be effective. Most investigators use between 4 and 10 punctures; more punctures have been associated with premature ovarian failure (120–122). As in all surgical procedures, an important issue of successful outcome is the expertise of the surgeon. There are no data regarding repeated application of LOS, and such use should not be encouraged.
. As in all surgical procedures, an important issue of successful outcome is the expertise of the surgeon. There are no data regarding repeated application of LOS, and such use should not be encouraged..")
9
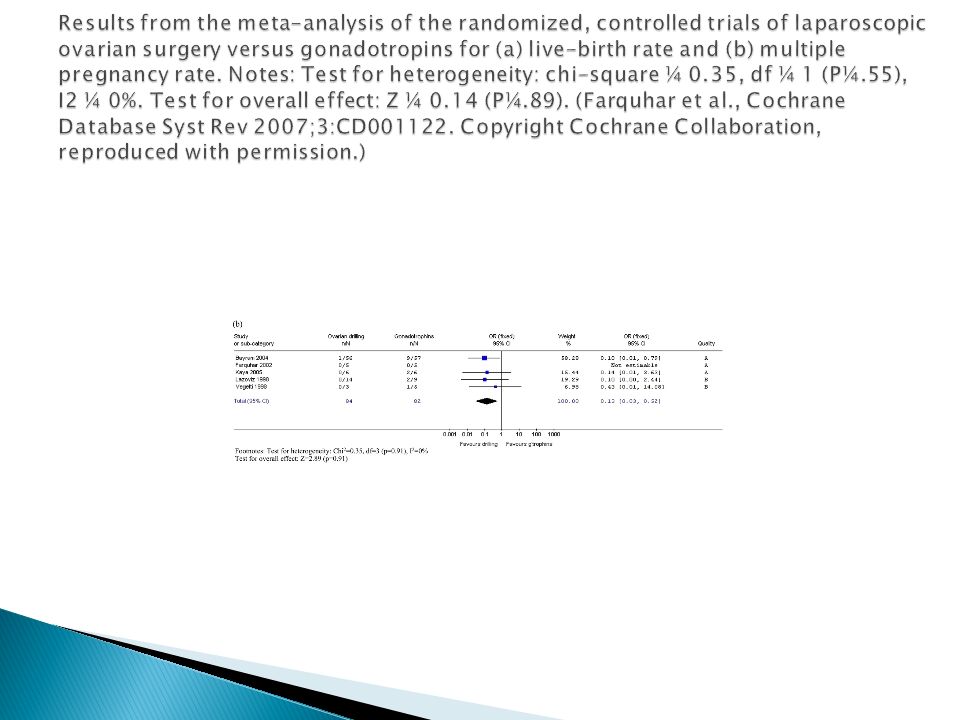
In approximately 50% of LOS-treated women, adjuvant therapy will be required. In these women, the addition of CC can be considered after 12 weeks if no ovulation is detected (123). The addition of FSH should be considered after 6 months. Five RCTs that compared the effectiveness of LOS with that of Gn for women with CC resistant PCOS did not show a difference in ongoing pregnancy rate or live-birth rate (117, 123–127).
. The addition of FSH should be considered after 6 months. Five RCTs that compared the effectiveness of LOS with that of Gn for women with CC resistant PCOS did not show a difference in ongoing pregnancy rate or live-birth rate (117, 123–127)..")
10
Multiple pregnancy rates were significantly higher in the gonadotropin arms of the five trials compared with LOS. On the other hand, miscarriage rates did not differ between the LOS group and gonadotropin- treated women. No cases of OHSS were observed in LOS arm of the two most recent studies. LOS treatment of women with CC-resistant PCOS resulted in reduced direct and indirect costs. Predictors of success have included LH level >10 IU/L, normal BMI, and shorter duration of infertility (12, 130, 131).
..")
11
Immediate complications of the surgery are rare, and include hemorrhage requiring laparotomy, bowel perforation have been reported (132). Long-term adverse events potentially include adhesion formation and premature menopause(133). In a second study of eight patients, all of the women had ovarian adhesions on second look after LOS despite the application of an adhesion barrier to one ovary as part of a study protocol (134). Premature ovarian failure is a concern with ovarian drilling, especially when a large number of punctures is used (135, 136).
. In a second study of eight patients, all of the women had ovarian adhesions on second look after LOS despite the application of an adhesion barrier to one ovary as part of a study protocol (134). Premature ovarian failure is a concern with ovarian drilling, especially when a large number of punctures is used (135, 136)..")
12
Techniques Four to six punctures per ovary using either electrocautery (diathermy) or laser vaporization Mechanism of action Poorly understood but believed to be via destruction of ovarian androgen-producing thecal cells leading to local and systemi reduction in androgen levels thus promoting follicular growth and ovulation Indications Anovulatory PCOS women with CCR, particularly when there are other indications for laparoscopy Results at 6 months Spontaneous ovulation rate: 54–76% Pregnancy rate: 28–56% Results at 12 months Spontaneous ovulation rate: 33–88% Pregnancy rate: 54–70%
 or laser vaporization Mechanism of action Poorly understood but believed to be via destruction of ovarian androgen-producing thecal cells leading to local and systemi reduction in androgen levels thus promoting follicular growth and ovulation Indications Anovulatory PCOS women with CCR, particularly when there are other indications for laparoscopy Results at 6 months Spontaneous ovulation rate: 54–76% Pregnancy rate: 28–56% Results at 12 months Spontaneous ovulation rate: 33–88% Pregnancy rate: 54–70%")
13
Predictors of poor success Morbid obesity (BMI >35) Marked biochemical hyperandrogenism (serum T ≥4.5 nmol/l) Duration of infertility >3 years LH/FSH ratio <2.0 (i.e., low basal LH levels) Advantages No requirement for monitoring as no increased risk of multiple pregnancy Disadvantages Possible short-term effect Surgical risks of laparoscopy, general anesthesia and ovarian damage including (rarely) ovarian atrophy, failure and adhesion formation
 Marked biochemical hyperandrogenism (serum T ≥4.5 nmol/l) Duration of infertility >3 years LH/FSH ratio <2.0 (i.e., low basal LH levels) Advantages No requirement for monitoring as no increased risk of multiple pregnancy Disadvantages Possible short-term effect Surgical risks of laparoscopy, general anesthesia and ovarian damage including (rarely) ovarian atrophy, failure and adhesion formation")
14
The prevalence of obesity in pcod ranging between 35% and 60%. Obesity predisposes to chronic anovulation in at least three distinct ways: 1. Increased peripheral aromatization of androgens, resulting in chronically elevated estrogen concentrations. 2. Decreased levels of hepatic SHBG production, resulting in increased circulating concentrations of free estradiol and testosterone. 3. Insulin resistance, leading to a compensatory increase in insulin levels that stimulates androgen production in the ovarian stroma, resulting in high local androgen concentrations that impair follicular development. Combined, these effects can be difficult to overcome, but even modest weight loss, which results in decreased circulating insulin and androgen concentrations, frequently restores ovulatory function and normal menstrual cyclicity.

15
We clearly are in a new era in our understanding and management of women with pcos. In the past, we treated the specific problems of infertility, dysfunctional uterine bleeding, and hirsutism effectively. We now have the opportunity, indeed the obligation, to offer interventions that can help prevent or reverse some of the metabolic consequences of the disorder that have an important impact on overall health and on the quality and quantity of life.

16
Bariatric or weight-loss surgery in the general population results in approximately 15–30% weight loss that is sustained in the long term [12]. A Cochrane review of bariatric surgery in the general population found that such surgery resulted in greater weight loss than conventional treatment in obesity (BMI >30 kg/m2) and a reduction in comorbidities such as diabetes and hypertension based on three RCTs and three prospective cohort studies [13]. However, this review did not assess fertility outcomes.
![ Bariatric or weight-loss surgery in the general population results in approximately 15–30% weight loss that is sustained in the long term [12].](http://images.slideplayer.com/22/6406592/slides/slide_16.jpg " A Cochrane review of bariatric surgery in the general population found that such surgery resulted in greater weight loss than conventional treatment in obesity (BMI >30 kg/m2) and a reduction in comorbidities such as diabetes and hypertension based on three RCTs and three prospective cohort studies [13]. However, this review did not assess fertility outcomes..")
17
Another systematic review of bariatric surgery in the general population assessed reproductive outcomes and reported that case–control and cohort studies show improved fertility and a reduction in obstetrical complications such as gestational diabetes, macrosomia and hypertensive disorders of pregnancy, but the incidence of intra-uterine growth restriction appears to be increased. No conclusions could be drawn regarding the risk of preterm labor and miscarriage [14].

18
consensus was reached in the British Fertility Society guidelines that fertility treatment should be deferred in the general population of women who are morbidily obese, until they have lost weight to below a BMI of 35 kg/m2 [16]. The results of pregnancies achieved after bariatric surgery have recently been reviewed [17]. The review supports the conclusion that the risk of adverse maternal and neonatal outcome could be reduced in women who are morbidly obese with PCOS by bariatric surgery before pregnancy. However, the review also identifies the lack of high- quality information. Further studies are recommended.
![ consensus was reached in the British Fertility Society guidelines that fertility treatment should be deferred in the general population of women who are morbidily obese, until they have lost weight to below a BMI of 35 kg/m2 [16].](http://images.slideplayer.com/22/6406592/slides/slide_18.jpg " The results of pregnancies achieved after bariatric surgery have recently been reviewed [17]. The review supports the conclusion that the risk of adverse maternal and neonatal outcome could be reduced in women who are morbidly obese with PCOS by bariatric surgery before pregnancy. However, the review also identifies the lack of high- quality information. Further studies are recommended..")
19
Thank you

Similar presentations






>")


 Jahrom university of medical.>")


>")



 is a disorder that causes menstrual and ovulation irregularities, androgen excess, and infertility.>")


 – Are We Wasting Women’s Time? Chima.>")



