Download presentation
Presentation is loading. Please wait.

1
Outpatient Management of Diabetes Mellitus Gary L. Francis, MD, PhD Professor and Associate Chair for Research USUHS

2
The Face of IDDM In 1920 was not Encouraging

3
1921 – Banting and Best Began to Isolate the “Internal Secretion of the Pancreas”

6
1923 Banting and Best Awarded Nobel Prize for Discovery And Use of Insulin in the Treatment of IDDM

7
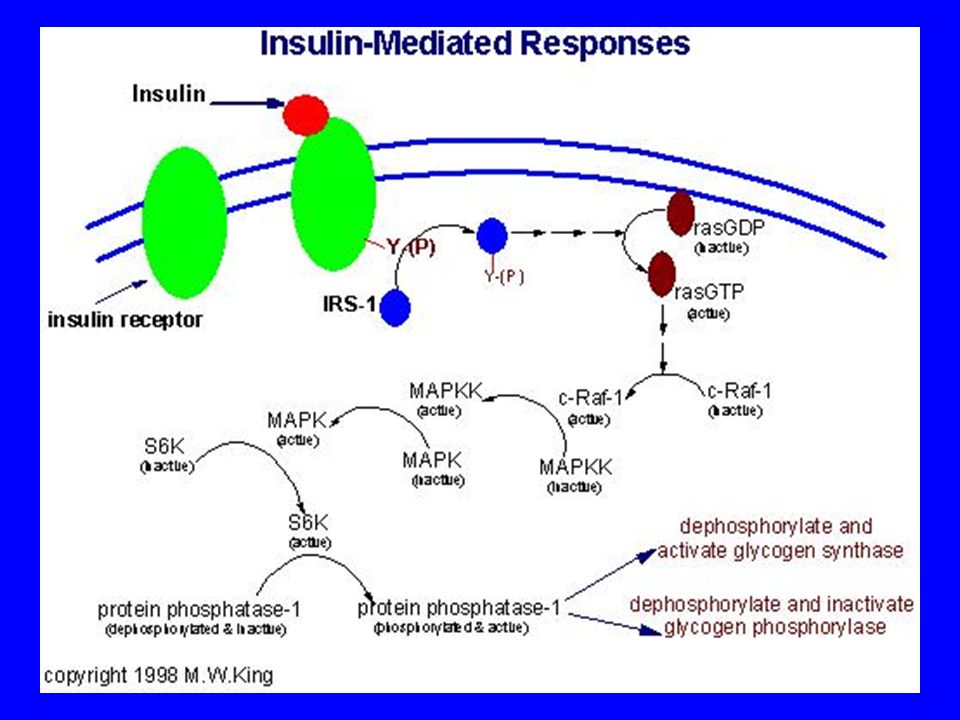
Islets of Langerhans -cell destruction Insulin Deficiency Adipo- cytes Muscle Liver Decreased Glucose Utilization Glucagon Excess Increased Protein Catabolism Increased Ketogenesis Gluconeogenesis IncreasedLipolysis Hyperglycemia Ketoacidosis Polyuria Volume Depletion Ketonuria

9
Classification of Different Forms of Diabetes Mellitus

10
Type 1 DM Autoimmune destruction of the pancreatic islet cell Hallmark = lymphocytic infiltration of islets Progresses over years Leads to insulin deficiency Later may also be associated with glucagon deficiency

11
Progression to Type 1 DM Autoimmune destruction “Diabetes threshold” Honeymoon 100% Islet loss Autoimmune markers (ICA, IAA, GAD

12
Disease-Free Survival is Shortened with More Numerous Antibodies

13
EPIDEMIOLOGY –Most common metabolic disease in childhood –Annual incidence 15 new cases per 100,000 in children < 18 yrs –Frequency increases with increasing age. –1: 1400 at age 5 yrs –1: 400 at age 16 yrs – Males and females equally affected – No correlation with socioeconomic status

14
IDDM RISK OF CONCORDANCE Offspring of IDDM parent: 2-5% overall risk Offspring of diabetic mother: 2% risk Offspring of diabetic father: 5% risk

15
Type I - IDDM 1.9/100,000 school age children 1/1430@ 5 yr of age 1/360 @ 16 yr of age ID twins –50% concordance risk Dizygotic twins –20% concordance risk Two shared HLA haplotypes (DR3 + DR4) –12-20% risk One shared HLA haplotype (DR3 or DR4) –5-7% risk No shared HLA haplotypes –1-2% risk HLA DQ(beta) Asp 57 –virtual protection HLA DQ(beta) non-Asp 57 –100 X increased risk
 –12-20% risk One shared HLA haplotype (DR3 or DR4) –5-7% risk No shared HLA haplotypes –1-2% risk HLA DQ(beta) Asp 57 –virtual protection HLA DQ(beta) non-Asp 57 –100 X increased risk")
16
DIABETES MELLITUS CLINICAL MANIFESTATIONS Classic Presentation: –Polyuria –Polydipsia –Polyphagia –Weight loss. Insidious –Onset of lethargy and weakness. –Duration of symptoms usually < 1 month.

17
DIABETES MELLITUS - TYPE I Body Systems Involved GU Urinary frequency GI Nausea, vomiting, constipation abdominal pain Respiratory Acidosis, Kussmaul breathing Cardiovascular Vascular collapse, dehydration tachycardia CNS Cerebral edema Musculoskeletal Glycogen depletion, K loss muscle weakness

18
DIABETES MELLITUS - TYPE 1 THERAPEUTIC OBJECTIVES Achieve metabolic control Maintain normal growth and sexual Maturation Prevent acute and chronic complications Prevent ketoacidosis

19
IDDM: OPTIMIZING GLYCEMIC CONTROL Hypoglycemia: –May be unaware –School grades –Early am symptoms Headache Nightmares –Look for at camp Reduce dose 10% Hyperglycemia: –Few symptoms –Nocturia –Dawn phenomenon –Adolescent insulin resistance Increase dose 10%

20
Treatment of T1 DM Insulin 1 u/kg/day – 1.3 u/kg/day in puberty –Standard 2 – 3 injections (NPH / Reg) / day Intensive Therapy –long acting at bedtime + short acting at meals –4 – 6 shots / day Insulin Pump Diet – adequate calories / limit fat / complex CHO Exercise GOAL – Optimal glycemic control
 / day Intensive Therapy –long acting at bedtime + short acting at meals –4 – 6 shots / day Insulin Pump Diet – adequate calories / limit fat / complex CHO Exercise GOAL – Optimal glycemic control")
21
DIABETES MELLITUS - TYPE 1 MONITORING STRATEGIES Self Blood Glucose Monitoring – 4-6 / day Urine Testing – Ketones - PRN Glycosylated Hemoglobin - HbA1 C - quarterly Blood lipids - annually Thyroid function – annually Urine microalbumin – quarterly after 5 yr Dilated fundoscopic – age 10 yr + 3-5 yr Hx

22
TYPE I - DIABETES MELLITUS MONITORING STRATEGIES Glycosylated hemoglobin - HbA1c – Average blood glucose 3-4 months – Affected by anemia, hemoglobinopathy Age dependent target range – Probably HbA1c < 8% for most – school age children – adolescents Beware of hypoglycemia (80% risk in DCCT)
")
23
Definition of Various Levels of Glycemic Control

24
DIABETES MELLITUS-TYPE I COMPLICATIONS AcuteChronic HypoglycemiaNeuropathy HyperglycemiaRetinopathy KetosisNephropathy Ketoacidosis

25
Hyperglycemia: Microangiopathic complications Hypoglycemia: Neuronal loss Poor school performance seizures

26
Microangiopathic complications from DM can occur by the time of diagnosis but typically 10 – 15 yr

27
Nephropathy Diabetes #1 cause of end-stage renal disease (ESRD) 1 st manifestation = microalbuminuria (low but abnormal, 30 mg/day or 20 µg/min urine albumin) Without intervention –In 80% albumin excretion increases 10–20% / year to overt nephropathy (albumin = 300 mg/24 h or 200 µg/min) over 10–15 yr Once nephropathy occurs –GFR falls over several years (2–20 ml · min -1 · year -1 ). –ESRD develops –in 50% of type 1 DM with nephropathy within 10 years –and in 75% by 20 yr. Microalbuminuria is rare with short duration of type 1 DM Screening in type 1 DM should begin after 5 yr of disease

28
Retinopathy After 20 yr, nearly all patients with T1 DM and >60% with T2 DM have some retinopathy In patients with T1 DM 3.6% of young-onset patients (aged <30 yr at dx) were legally blind –86% of blindness was due to diabetic retinopathy 1.6% of old-onset patients (aged 30 yr at dx) were legally blind. Vision-threatening retinopathy almost never occurs with T1 DM in the first 3–5 years of diabetes or before puberty. Dilated funduscopic – age 10 yr + 3-5 yr Hx

30
Typical Split-Dose NPH-REG BID Regimen

31
BID NPH / REG AM NPH / REG DINNER REG HS NPH

32
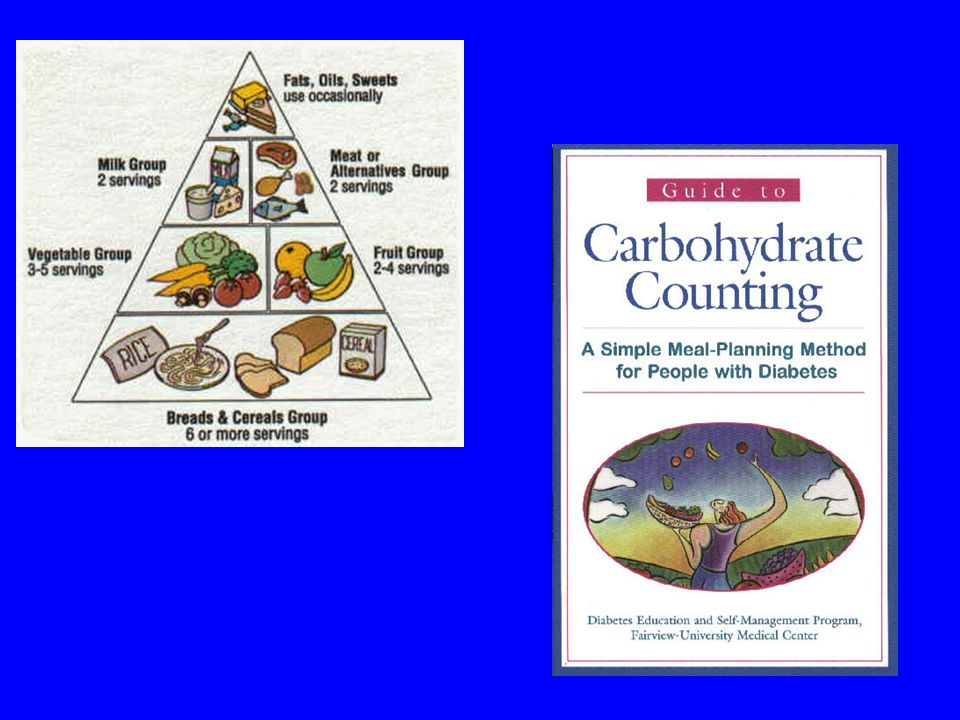
OPC Management Tools School Individual treatment plan Glucagon Administer for severe low BG Nutrition 55% CHO –Complex CHOs 30% FAT –< 10% Saturated 15% Protein

33
SICK DAY MANAGEMENT 1. NEVER omit your insulin, even if you can't eat. 2.Test your blood sugar every 4 hours. If you need help, ask for it! 3.If you have T1 DM, test your urine for ketones every 4 hours. 4.Drink clear liquids (at least ½ cup / hr), and eat light foods 5.Rest. Do not exercise during an illness. 6.Call your doctor or diabetes educator if: You have an obvious infection Your illness lasts longer than 2 days You have vomiting or diarrhea more than 8 hours Your blood sugar is over 400 mg in two consecutive tests All urine tests are positive for large amounts of sugar You have moderate to large urine ketones with a blood glucose level over 200 mg for more than 8 hours You feel very ill or experience pain You have extreme fatigue, shortness of breath, or dizziness
, and eat light foods 5.Rest. Do not exercise during an illness. 6.Call your doctor or diabetes educator if: You have an obvious infection Your illness lasts longer than 2 days You have vomiting or diarrhea more than 8 hours Your blood sugar is over 400 mg in two consecutive tests All urine tests are positive for large amounts of sugar You have moderate to large urine ketones with a blood glucose level over 200 mg for more than 8 hours You feel very ill or experience pain You have extreme fatigue, shortness of breath, or dizziness.")
34
For blood sugar over 150 mg/dl, add 10% of your total daily dose as Regular insulin every 4-6 hours. Here is an example: Blood sugar is 210 mg and urine ketones are negative. Total usual AM dose of insulin NPH Regular 22 units 4 units Total usual PM dose of insulin NPH Regular 10 units 4 units GRAND TOTAL:40 Units 10% of the total dose = 4 units. Add 4 units regular insulin to usual dose every 4-6 hours, when blood sugar is over 150 mg.

35
For blood sugar over 150 mg/dl PLUS moderate to large ketones in the urine, add 20% of your total daily dose as Regular insulin every 4-6 hours. Example: Blood sugar is 300 mg, urine ketones - positive. Total usual AM dose of insulin NPH Regular 14 units 2 units Total usual PM dose of insulin Regular4 units Total usual bedtime dose of insulin NPH10 units GRAND TOTAL:30 Units 20% of the total dose = 6 units. Add 6 units regular insulin to usual dose every 4-6 hours, when blood sugar is over 150 mg and urine ketones are positive.

36
DCCT Study Findings Lowering blood glucose reduces risk: Eye disease 76% reduced risk Kidney disease 50% reduced risk Nerve disease 60% reduced risk The DCCT is a clinical study conducted from 1983 to 1993 by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). The study showed that keeping blood glucose levels as close to normal as possible slows the onset and progression of eye, kidney, and nerve diseases caused by diabetes. NEJM 342:381-389, 2000

37
RS is a 12 yr old female with T1 DM for 6 yrs. A1C = 7.3, insulin dose is AM: 8 Reg / 18 NPH; Dinner: 7Reg; HS: 20 NPH. BGs

38
Continuous Glucose Monitor - Overnight Unsuspected and Asymptomatic Hypoglycemia – Common up to 85% of episodes are nocturnal

39
Continuous Glucose Monitoring Device Worn like the pump Inserted with similar tubing and catheter Records continuously for three days Downloaded to your computer Data not yet available for patient use Chase et al Pediatrics 107: 222 (2001) –5 patients, 10 – 17 yr old, DM 3.8 – 9.3 yr –12.8 hypoglycemic episodes / patient / month –85% asymptomatic nocturnal –15% symptomatic nocturnal
 –5 patients, 10 – 17 yr old, DM 3.8 – 9.3 yr –12.8 hypoglycemic episodes / patient / month –85% asymptomatic nocturnal –15% symptomatic nocturnal")
40
Continuous Glucose Monitoring in Children with IDDM Majority have unsuspected, nocturnal hypoglycemia Current insulin regimens are non- physiologic despite what we teach the residents We need to develop new paradigms that incorporate designer insulins and pumps into management strategies for our patients

41
BG Breakfast Lunch Dinner Insulin

42
Currrent Insulins NPH Precipitated with protamine Requires 45 inversions to mix and achieve same bioavailability Peak 4 – 10 hr Lasts 12-18 hr Patient and site variability Regular Supposed to be “fast” Onset is ½ - 1 hr Peak 2 – 3 hr Lasts 6 – 8 hrs Hexamers in bottle delay absorption Mis-match meal – insulin results in lows

43
BID Split-Dose / Mixed NPH / REG Induces fasting hyperinsulinemia and frequent hypoglycemia Requires between meal snacks Predisposes to obesity Can NOT mimic pancreatic ß-cell insulin secretion Limited day-to-day variability

44
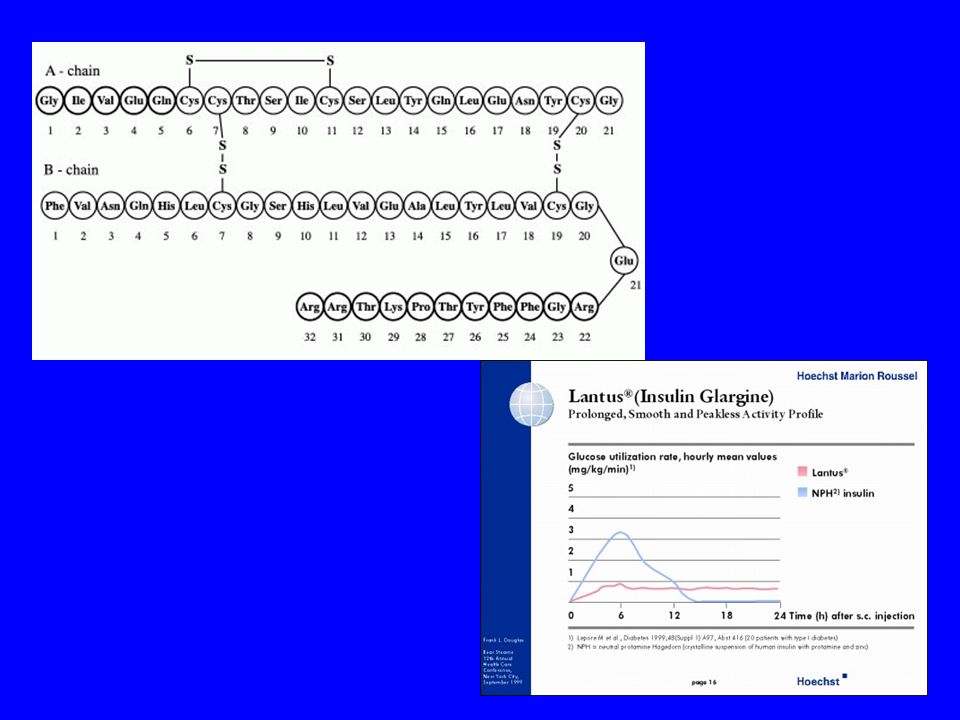
“Designer” Insulins Glargine GLY 21 /ARG 31 /ARG 32 Ultra-long acting No “peak effect” Could be used to provide “basal” insulin secretion like pump therapy Lispro Invert lysine/proline Currently in use Ultra-short acting Onset 15 minutes Duration – < 4 hrs Excellent for meal bolus, “correction” bolus, bedtime highs, toddlers

47
Glargine / Lispro Avoids fasting hyperinsulinemia and hypoglycemia Can mimic pancreatic ß- cell insulin secretion 36% had hypoglycemia vs 50% on NPH

49
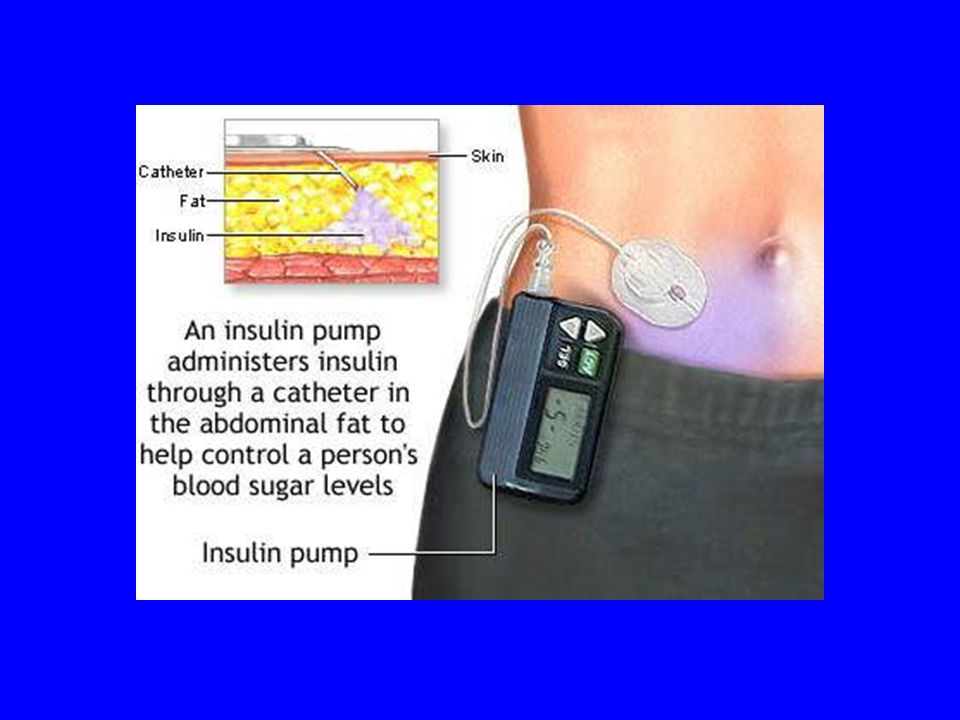
Insulin Pump Therapy 6,500 in 1990 – 46,500 in 1998 Uses Lispro Insulin ONLY NO DEPOT –Reduces hypoglycemia –Shortens time to DKA Can mimic pancreatic ß- cell insulin secretion Improves life-style variability Reduces need for snacks

50
INSULIN PUMP THERAPY IN CHILDREN First US Attempts: Yale University – 1970s –Increased short term mortality –Presumed: unrecognized hypoglycemia –Abandoned for several years Problems: –Patients selected for poor compliance –Limited home BG technology –Regular insulin infused

52
Contemporary Insulin Pump Therapy in Children Most studies have highly selected patients –Motivated, educable, adult supervision –Learn carbohydrate counting, insulin adjustment –Ideal: intensive Rx with MDI for 3-6 months first Lispro Insulin –No depot to induce hypoglycemia –No depot to protect from ketoacidosis Target glucose range MUST be individualized –Age appropriate –Adjusted for day-to-day changes in activity Maniatis et al Pediatrics 107:351 (2001) –CSII in Routine DM Management works for most patients 10 / 17 with A1c > 9 did poorly tended to be male and skipped meal bolus shots
 –CSII in Routine DM Management works for most patients 10 / 17 with A1c > 9 did poorly tended to be male and skipped meal bolus shots")
53
Components

54
Typical Insulin Calculations BASAL –Total daily dose – 25% –½ that is basal –Divide into equal 24 hr infusion rate BASAL –TDD = 40 units/day –40 – 25% = 30 units/day –½ = 15 units basal –15 / 24 = 0.6 units/hr

55
Meal and Correction Bolus Meals –CHO gms/meal –Divide by CHO factor –400 / TDD = gm CHO / unit insulin –400 / 30 = 13 gm CHO / 1 unit insulin “Correction” –Insulin sensitivity factor = 1500 / TDD –1500 / 30 = 50 mg/dl drop in BG for 1 unit insulin

57
RS typical insulin pump Rx TDD = 40 units / day Basal 40 – 25% = 30 30 / 2 = 15 units/day 15/24 = 0.6 units/hr Breakfast BG = 180 Meal plan calls for 60 gm CHO Meal Bolus –400 / 30 = 13 gm CHO / unit insulin –60 gm / 13 = 4.6 units Correction Bolus –1500 / 30 = 50 mg/dl drop / unit insulin –180 – 120 (target) = 60 –60 / 50 = 1.2 units Pre-Breakfast dose = 4.6 + 1.2 = 5.8 units
 = 60 –60 / 50 = 1.2 units Pre-Breakfast dose = = 5.8 units")
58
PUMP THERAPY IN CHILDREN PRO AND CON PROs –Mimic pancreatic secretion –Adjustable to lifestyle –Accurate dosing (syringe is +/- 52%) –Lower insulin levels –Hypoglycemia (Risks are lower than with MDI dosing) CONs –No depot ketoacidosis can begin in 2-4 hours –Expense - $6,000 –Motivated, educated family and patient –Labor intensive start-up takes about 1 month
 –Lower insulin levels –Hypoglycemia (Risks are lower than with MDI dosing) CONs –No depot ketoacidosis can begin in 2-4 hours –Expense - $6,000 –Motivated, educated family and patient –Labor intensive start-up takes about 1 month")
59
DIABETES MELLITUS CLASSIFICATION Type 1 (IDDM) –Typical symptoms - glycosuria, ketonemia –Random Plasma Glucose > 200 mg/dl –Fasting plasma glucose > 127 mg/dl Type 2 (NIDDM) –Typical symptoms –Fasting plasma glucose > 127 mg/dl –2 hr post prandial glucose > 200 mg/dl
 –Typical symptoms - glycosuria, ketonemia –Random Plasma Glucose > 200 mg/dl –Fasting plasma glucose > 127 mg/dl Type 2 (NIDDM) –Typical symptoms –Fasting plasma glucose > 127 mg/dl –2 hr post prandial glucose > 200 mg/dl")
60
Different Forms of MODY

61
Type 2 Diabetes Mellitus in Children Historically - Incidence 8-10% of children with DM PIMA Indians 1960s –Positive F-Hx –Obesity related –Increased Insulin and C-peptide –First US population with T2-DM > T1-DM –5% incidence 15-19 yr old vs 0.33% T1-DM New Cases/100,000/yr (San Diego, LA, Cincinnati)
")
62
TYPE 2 DM IN CHILDREN Among 10 – 19 yr olds in the US T2 DM accounts for 33% of all new cases –African Americans – 42% –Caucasians – 10%

63
Obesity Acanthosis Nigricans Adolescence

65
T2 DM vs T1 DM T2 - DMT1 - DM Polyuria/dypsia++ Ketonuria+ / - DKA+ / - Autoimmunity+ / -+ Initial insulinOften requiredRequired Honeymoon++ Worse @ illness++

66
T2 DM vs T1 DM T2 DMT1 DM Obesity95% > 85%tileNot Common + Family Hx T272 – 85%Not Common Acanthosis Nigricans 60 – 86%7% all school aged children Maternal Gestational DM +Not Common IUGR+Not common

67
Pathophysiology of T2 DM Multifactorial Disease Genetic Twin studies –50 – 90% concordance PIMA Indians –AD Single gene 4q Mexican-Americans –Susceptibility locus 2 Insulin resistance –African Americans 30% less insulin sensitive than Caucasians Environment Insulin Resistance –Obesity –Inactivity –High fat CHO diet –Mean age of onset = 13 yr –30% higher insulin requirement in puberty Decline in insulin –“glucose toxicity” IUGR –Impaired insulin sensitivity high insulin levels reduced GLUT-1 transporter

68
Diagnosis of T1 vs T2 DM Obese Adolescent High risk ethnic group C-Peptide + Insulin –Elevated = T2 DM –Not-Elevated –Immune Markers Thin Adolescent Pre-adolescent Low risk ethnic group Immune Markers –Positive = T1 DM –Negative –C-Peptide and Insulin

69
CO is a 9 yr 6 mo male with “IDDM” for 3 yr Dx hyperglycemia no DKA No hospital admits since Rx insulin: –24 units / 56.7 kg –AM 3 R / 9 N –PM 5 R / 7 N A1C = 6.5 BGs –AM 146 – 143 –Noon 94 – 116 –PM 106 - 167 African American Obesity Acanthosis Family history T2 DM Type I or Type II? Should he be Rx with –Insulin? –Metformin? –Both?

70
Treatment of T2 DM in Children Decreased caloric intake Decreased insulin resistance Screen for microangiopathic complications Drug Treatment Insulin –Only approved drug for use in children Metformin –Biguanide –Suppresses hepatic glucose production

71
Therapy of T2 DM in Children Reduce calories – weight loss –NOT T1 DM diet with high complex CHO No Between meal snacks –NOT T1 DM where hypoglycemia is frequent Reduce CHO intake Reduce fat intake Exercise – increase healthy life style NOT USUALLY EFFECTIVE Drug treatment early

Similar presentations




















 Diabetes Mellitus.>")



>")

