Download presentation
Presentation is loading. Please wait.

1
NHSN Surveillance: What’s New for 2013 Andrea Alvarez, MPH Carol Jamerson, RN, BSN, CIC Virginia Department of Health

2
Objectives Review some of the changes to 2013 NHSN protocols Demonstrate some new data entry and analysis functionality in NHSN Direct users to additional NHSN resources/training Provide an open forum for Q&A

3
Changes to Key Terms Healthcare-Associated Infection (HAI) Device-Associated Transfer Rule Date of Event
 Device-Associated Transfer Rule Date of Event")
4
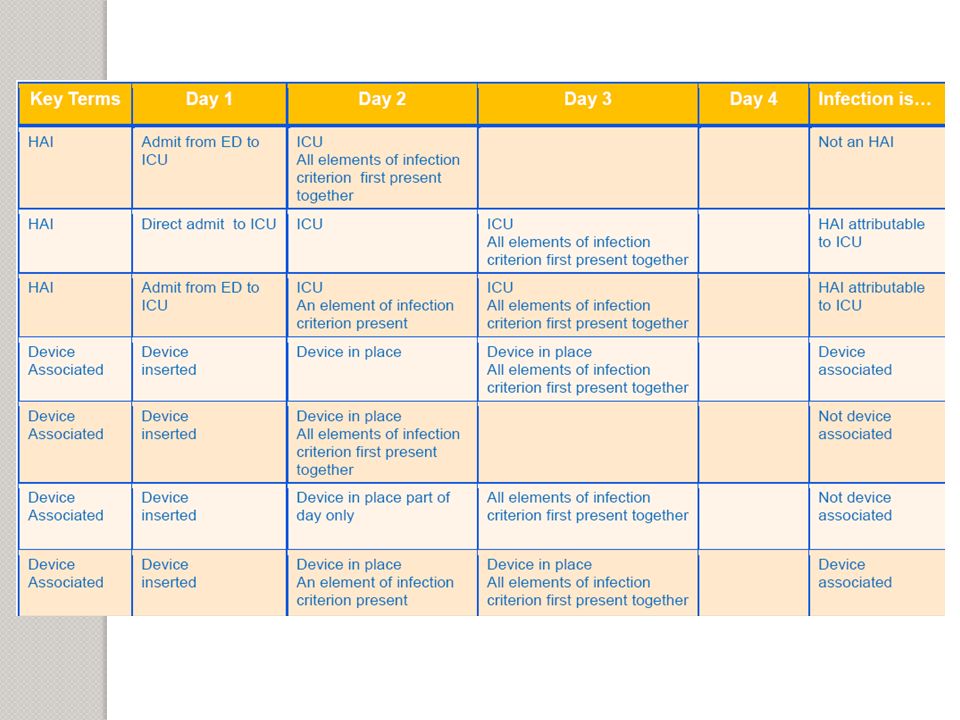
HAI and Device-Associated Infection Healthcare-associated Infection (HAI): ◦ Localized or systemic condition resulting from an adverse reaction to the presence of an infectious agent(s) or its toxin(s) that was not present on admission. ◦ All elements of a CDC/NHSN site-specific infection criterion first present together on or after the 3rd hospital day (day of hospital admission is day 1). ◦ An element of the infection criterion may be present during the first 2 hospital days as long as it is also present on or after day 3. ◦ All elements used to meet the infection criterion must occur within a timeframe that does not exceed a gap of 1 calendar day between elements. Device-associated Infection: ◦ Device was in place for >2 calendar days when all elements of a CDC/NHSN site-specific infection criterion were first present together. ◦ HAIs occurring on the day of device discontinuation or the following calendar day are considered device-associated HAIs if the device had been in place already for >2 calendar days.
. ◦ An element of the infection criterion may be present during the first 2 hospital days as long as it is also present on or after day 3. ◦ All elements used to meet the infection criterion must occur within a timeframe that does not exceed a gap of 1 calendar day between elements. Device-associated Infection: ◦ Device was in place for >2 calendar days when all elements of a CDC/NHSN site-specific infection criterion were first present together. ◦ HAIs occurring on the day of device discontinuation or the following calendar day are considered device-associated HAIs if the device had been in place already for >2 calendar days..")
6
Transfer Rule If all elements of an HAI were present within 2 calendar days of transfer from one inpatient location to another in the same facility (i.e., on the day of transfer or the next day), the HAI is attributed to the transferring location. If all elements of an HAI were present within 2 calendar days of transfer from one inpatient facility to another, the HAI is attributed to the transferring facility. Receiving facilities should share information about such HAIs with the transferring facility to enable reporting.

8
Transfer Rule: Question from the Field Q: Patient is seen in the ED, central line is placed, and patient is moved to the medical ICU. She receives IV medications and line care. On day 3, fever and chills are present. Two sets of blood cultures are collected and sent to the lab. On day 5, cultures come back positive for S. epidermidis. Insertion site is clean and free from inflammation and no other documented signs of infection. Where do we attribute the infection? A: This patient meets the definition for lab- confirmed bloodstream infection 2. Infections cannot be attributed to a location where patients are not housed overnight (like an OR or ED). The infection should be attributed to the next inpatient location; in this case the MICU.
. The infection should be attributed to the next inpatient location; in this case the MICU..")
9
Date of Event Also known as infection date, date of infection For HAIs [excluding Ventilator-Associated Events (VAE)]: the date when the last element used to meet the CDC/NHSN site-specific infection criterion occurred. For VAE: the date of onset of worsening oxygenation (i.e., the first calendar day in which the daily minimum worsening oxygenation threshold value occurs). Ex. CAUTI ◦ Seen in ED 2/11/13 ◦ Admitted to medical ICU; urinary catheter inserted 2/12/13 ◦ Develops fever 2/14/13 ◦ Urine specimen collected 2/15/13 (positive for E. coli, 10 5 organisms) ◦ What is date of event? 2/15/13
![Date of Event Also known as infection date, date of infection For HAIs [excluding Ventilator-Associated Events (VAE)]: the date when the last element used to meet the CDC/NHSN site-specific infection criterion occurred.](http://images.slideplayer.com/22/6400408/slides/slide_9.jpg "For VAE: the date of onset of worsening oxygenation (i.e., the first calendar day in which the daily minimum worsening oxygenation threshold value occurs). Ex. CAUTI ◦ Seen in ED 2/11/13 ◦ Admitted to medical ICU; urinary catheter inserted 2/12/13 ◦ Develops fever 2/14/13 ◦ Urine specimen collected 2/15/13 (positive for E. coli, 10 5 organisms) ◦ What is date of event. 2/15/13.")
10
Vital Signs and Fever If a specific value for a vital sign is not stated in a CDC/NHSN HAI definition criterion, the facility should use the vital sign parameters as stated in its policies and procedures for clinical documentation. ◦ For example, if a facility has a policy to adjust temperature readings to reflect core temperatures, then the adjusted temperature value used for clinical decision making should be used for its HAI surveillance as well. When assessing infection criteria (ex. for CAUTI and VAP), “with no other recognized cause” phrase removed for fever/hypothermia. o Fever/hypothermia are non-specific findings and can be caused by more than one infectious/non-infectious process.
, with no other recognized cause phrase removed for fever/hypothermia. o Fever/hypothermia are non-specific findings and can be caused by more than one infectious/non-infectious process..")
11
Central Line-Associated Bloodstream Infection (CLABSI) Changes Mucosal barrier injury laboratory-confirmed BSI ◦ Pertains to patients who are post allogeneic hematopoietic stem cell transplant or severely neutropenic CLABSI rates in this population inflated by misclassification of BSI resulting from translocation of intestinal organisms These BSIs not impacted by CLABSI prevention measures and not associated with the central line ◦ Will not be removed from CLABSI case counts for CMS purposes in 2013 Updated secondary bloodstream infection guide (see Appendix 1 of CLABSI protocol) ◦ Note: this guide is not applicable to VAE
 Changes Mucosal barrier injury laboratory-confirmed BSI ◦ Pertains to patients who are post allogeneic hematopoietic stem cell transplant or severely neutropenic CLABSI rates in this population inflated by misclassification of BSI resulting from translocation of intestinal organisms These BSIs not impacted by CLABSI prevention measures and not associated with the central line ◦ Will not be removed from CLABSI case counts for CMS purposes in 2013 Updated secondary bloodstream infection guide (see Appendix 1 of CLABSI protocol) ◦ Note: this guide is not applicable to VAE")
12
CLABSI: MBI-LCBI Definitions Intestinal organism (see list in protocol) or viridans group strep identified, with no other organisms identified AND At least one of the following: ◦ Allogeneic hematopoietic stem cell transplant recipient with one of two documented clinical symptoms/manifestations ◦ Neutropenia Slight modification of definition for infants (MBI-LCBI Criterion 3)
 or viridans group strep identified, with no other organisms identified AND At least one of the following: ◦ Allogeneic hematopoietic stem cell transplant recipient with one of two documented clinical symptoms/manifestations ◦ Neutropenia Slight modification of definition for infants (MBI-LCBI Criterion 3)")
13
CLABSI: Question from the Field Q: I have a patient who was admitted to the medical/surgical ICU with an implanted port-a-cath. On day 4, criteria were met for a LCBI. What do I consider the first day for the line since it was in place on admission? A: If admitted or transferred to a facility with a central line in place (e.g., tunneled or implanted central line), the day of first access is day 1.
, the day of first access is day 1..")
14
SSI Changes No more information collected on implants New post-discharge surveillance time periods for deep incisional and organ/space SSIs ◦ 30-day: AAA, AMP, APPY, AVSD, BILI, CEA, CHOL, COLO, CSEC, GAST, HTP, HYST, KTP, LAM, LTP, NECK, NEPH, OVRY, PRST, REC, SB, SPLE, THOR, THYR, VHYS, XLAP ◦ 90-day: BRST, CARD, CBGB, CBGC, CRAN, FUSN, FX, HER, HPRO, KPRO, PACE, PVBY, RFUSN, VSHN

15
SSI Changes: Primary Closure Closure of all tissue levels, regardless of the presence of wires, wicks, drains, or other devices or objects extruding through the incision. If there is nothing extruding from the incision but the skin edges are not fully reapproximated for the entire length of the incision (e.g., is loosely closed with gaps between suture/staple points), the incision is not considered primarily closed and therefore the procedure would not be considered an operation.
, the incision is not considered primarily closed and therefore the procedure would not be considered an operation..")
16
SSI: Question from the Field Q: Patient had a colectomy and the skin was closed with sutures in the operating room. A penrose drain was woven in- between the suture line. Is this considered a primary closure? A: Yes. In this instance, all tissue levels were closed. The presence of the drain does not affect whether it is a primary closure.

17
New VAE Protocol Replaces prior VAP event definitions (PNEU) – those are now for patients <18 yrs VAE protocol for adult patients in acute care, long-term acute care, or inpatient rehab Three tiers of VAE definitions - hierarchical ◦ Ventilator-Associated Condition (VAC) ◦ Infection-related Ventilator-Associated Complications (IVAC) ◦ Possible and Probable Ventilator-Associated Pneumonia (VAP)
 – those are now for patients <18 yrs VAE protocol for adult patients in acute care, long-term acute care, or inpatient rehab Three tiers of VAE definitions - hierarchical ◦ Ventilator-Associated Condition (VAC) ◦ Infection-related Ventilator-Associated Complications (IVAC) ◦ Possible and Probable Ventilator-Associated Pneumonia (VAP)")
19
IVAC: Infection-related Ventilator- Associated Complication Patient meets criteria for VAC and on or after calendar day 3 of mechanical ventilation and within 2 calendar days before or after the onset of worsening oxygenation, the patient meets both of the following criteria: ◦ Temperature >38°C or <36°C OR white blood cell count ≥12,000 cells/mm 3 or ≤ 4,000 cells/mm 3 and ◦ A new antimicrobial agent is started and continued for ≥ 4 calendar days

20
VAE Calculator No patient identifiers required Does not store any data that you enter Does not report any data that you enter or any VAE determinations to NHSN Cannot export data entered into the calculator, although you can print screen shots if that is helpful to you http://www.cdc.gov/nhsn/VAE- calculator/index.html http://www.cdc.gov/nhsn/VAE- calculator/index.html

21
Overview of LabID Reporting Reporting of proxy infection measures of MDRO and C. difficile healthcare acquisition, exposure burden, and infection burden by using primarily laboratory data ◦ Never include results from active surveillance testing Less labor-intensive means to track MDROs & CDI NHSN application classifies whether an event is community- onset (CO) or healthcare-onset (HO) based on inpatient admission date and specimen collection date ◦ NHSN will report HO events to CMS, excluding duplicates and recurrent CDI events (collected >2 weeks and ≤8 weeks after the most recent CDI labID event for that patient) For C. diff, community-onset healthcare facility-associated (CO-HCFA) events are from patients who are discharged from the facility ≤4 weeks prior to the stool specimen collection date
 or healthcare-onset (HO) based on inpatient admission date and specimen collection date ◦ NHSN will report HO events to CMS, excluding duplicates and recurrent CDI events (collected >2 weeks and ≤8 weeks after the most recent CDI labID event for that patient) For C. diff, community-onset healthcare facility-associated (CO-HCFA) events are from patients who are discharged from the facility ≤4 weeks prior to the stool specimen collection date.")
22
Pre-populated Auto-populated

23
MDRO Module Notes SIR reports available for MRSA bacteremia and C. difficile (acute care hospitals only) ◦ Baseline: 2010-2011 FacWideIn labID data ◦ Calculated for 2012 data and forward ◦ SIRs specific to CMS IPPS reporting available for 2013 and forward (limited to in-plan) ◦ Adjusts for medical school affiliation, facility bedsize, community-onset prevalence rate, & test type (CDI only) A note about denominators – facility-wide inpatient reporting is required for CMS ◦ Report single denominators for entire facility, not by unit Separate counts for MRSA and CDI Minus baby locations for CDI (NICU, specialty care nursing, well baby locations)
 ◦ Baseline: FacWideIn labID data ◦ Calculated for 2012 data and forward ◦ SIRs specific to CMS IPPS reporting available for 2013 and forward (limited to in-plan) ◦ Adjusts for medical school affiliation, facility bedsize, community-onset prevalence rate, & test type (CDI only) A note about denominators – facility-wide inpatient reporting is required for CMS ◦ Report single denominators for entire facility, not by unit Separate counts for MRSA and CDI Minus baby locations for CDI (NICU, specialty care nursing, well baby locations).")
24
If your facility has no events for the month, indicate this on the summary data record If LabID events have already reported, the “Report No Events” box will be disabled, preventing it from being checked. Reporting No Events

25
MRSA Bacteremia LabID event CLABSI Identified with MRSA as a Pathogen

26
Demo of NHSN Data entry New reports

27
Resources NHSN protocols and resources for hospital users o http://www.cdc.gov/nhsn/acute-care-hospital/index.html http://www.cdc.gov/nhsn/acute-care-hospital/index.html ***NHSN training – Oct 2012 slides*** o http://www.cdc.gov/nhsn/training/ (see New Training box on right side of page) http://www.cdc.gov/nhsn/training/ North Carolina-Virginia Hospital Engagement Network VAE webinar o http://www.ncqualitycenter.org/nocva/vap.lasso (see Webinar box on the right side of the page – January 16, 2013) http://www.ncqualitycenter.org/nocva/vap.lasso VAE calculator o http://www.cdc.gov/nhsn/VAE-calculator/index.html http://www.cdc.gov/nhsn/VAE-calculator/index.html Patient Safety analysis resources o http://www.cdc.gov/nhsn/PS-Analysis-resources/index.html http://www.cdc.gov/nhsn/PS-Analysis-resources/index.html CMS requirements o http://www.cdc.gov/nhsn/cms/index.html http://www.cdc.gov/nhsn/cms/index.html
 North Carolina-Virginia Hospital Engagement Network VAE webinar o (see Webinar box on the right side of the page – January 16, 2013) VAE calculator o Patient Safety analysis resources o CMS requirements o")
28
Contact Us! Andrea Alvarez – Program Coordinator Andrea.Alvarez@vdh.virginia.gov Carol Jamerson – Nurse Epidemiologist Carol.Jamerson@vdh.virginia.gov ◦ For Andrea or Carol – 804-864-8141 April Achter – new HAI Epi! April.Achter@vdh.virginia.gov 757-683-2479 www.vdh.virginia.gov/epidemiology/surveillance/hai

Similar presentations









 Richard Rodriguez, MPH Connecticut Department of Public Health 4/9/2014 Thank you to CDC.>")




, CIC Infection Preventionist Consultant.>")


 in 2015>")



