Download presentation
Presentation is loading. Please wait.

1
CHAPTER 17 THE FINAL CHALLENGE: DEATH AND DYING

2
Learning Objectives How is death defined? Why is the definition of death controversial? How does the social meaning of death vary across groups? What factors influence life expectancy? Is it possible to extend life expectancy? What is the difference between programmed theories of aging and damage theories of aging? Give an example of each.

3
Matters of Life and Death – What Is Death?
A Harvard Medical School committee has defined biological death in terms of brain functioning Total brain death is an irreversible loss of functioning in the entire brain, both the higher centers of the cerebral cortex that are involved in thought and the lower centers of the brain that control basic life processes such as breathing

4
Matters of Life and Death – What Is Death?
According to the Harvard Medical School definition, to be judged dead, a person must meet the following criteria Be totally unresponsive to stimuli, including painful ones Fail to move for 1 hour and fail to breathe for 3 minutes after being removed from a ventilator Have no reflexes (for example, no eye blink and no constriction of the eye’s pupil in response to light) Register a flat electroencephalogram, indicating an absence of electrical activity in the cortex of the brain As an added precaution, the testing procedure is repeated 24 hours later
 Register a flat electroencephalogram, indicating an absence of electrical activity in the cortex of the brain. As an added precaution, the testing procedure is repeated 24 hours later.")
5
Matters of Life and Death – What Is Death?
The term euthanasia refers to hastening the death of someone suffering from an incurable illness or injury Euthanasia means “happy” or “good” death Active euthanasia, also called “mercy killing,” is deliberately and directly causing a person’s death (e.g., by administering a lethal dose of drugs to someone in the late stages of cancer) Passive euthanasia means allowing a terminally ill person to die of natural causes (e.g., by withholding extraordinary life-saving treatments)
 Passive euthanasia means allowing a terminally ill person to die of natural causes (e.g., by withholding extraordinary life-saving treatments)")
6
Matters of Life and Death – Life and Death Choices
Assisted suicide is another means by which death is hastened Assisted suicide makes available to a person who wishes to die the means by which she may do so (e.g., writing a prescription for sleeping pills for a person with the knowledge that she likely will take an overdose)
")
7
Matters of Life and Death – Life and Death Choices
Medical personnel and the general public support passive euthanasia More than 70% of U.S. adults reportedly support a doctor’s right to end the life of a patient with a terminal illness African Americans and other minority group members are generally less accepting of actions to hasten death than European Americans

8
Matters of Life and Death – Life and Death Choices
In most U.S. states it is legal to withhold extraordinary life-extending treatments and to terminate life-support activities when that is the wish of the dying person or when the immediate family can show that such action would be consistent with the dying person’s wishes A living will is a form of advance directive by which people can State that they do not want extraordinary medical procedures applied to them Specify who should make decisions on their behalf if they are unable to do so Direct whether organs should be donated Provide other instructions for actions to be carried out after death

9
Matters of Life and Death – Life and Death Choices
In 1997, Oregon became the first state to legalize physician-assisted suicide Terminally ill adults with 6 or fewer months to live can request lethal medication from a physician Those who have utilized physician-assisted suicide usually had terminal cancer and believed that they faced only hopeless pain and suffering and a loss of dignity with no chance of recovery Forty states have enacted laws against assisted suicide

10
Matters of Life and Death – Life and Death Choices
Death may be universal, and the tendency to react negatively to loss may be too However, the experiences of dying individuals and of their survivors are shaped by the historical and cultural contexts in which death occurs The social meanings attached to death vary widely from historical era to historical era and from culture to culture Different ethnic and racial groups have different rules for expressing grief and different mourning practices

11
Matters of Life and Death – What Kills Us and When?
In the U.S., life expectancy at birth is almost 78 years The average number of years a newborn can be expected to live The life expectancy for white males is almost 76 years The life expectancy for white females is almost 81 years The life expectancy for African-American males is 70 years The life expectancy for African-American females is 77 years

12
Caption: Life expectancy at birth for the world and major areas 1950-2050

13
Matters of Life and Death – What Kills Us and When?
Death rates change over the lifespan Infants are vulnerable, with the U.S. infant mortality rate standing at fewer than 7 out of 1,000 live births We have a relatively small chance of dying during childhood and adolescence Death rates climb steeply and steadily throughout adulthood

14
Matters of Life and Death – What Kills Us and When?
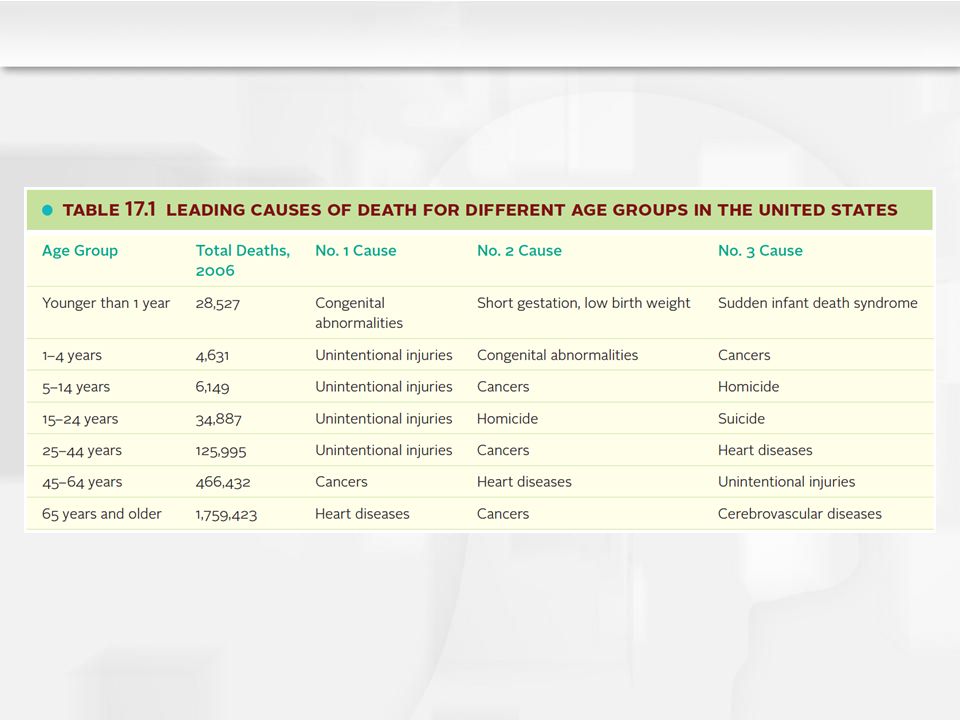
The causes of death change over the lifespan Infant deaths are mainly associated with birth complications and congenital abnormalities Preschool and school-age children’s deaths are caused by unintentional injuries or accidents (especially car accidents but also poisonings, falls, fires, and drownings) The leading killers of adolescents are accidents (especially car accidents), homicides, and suicides
 The leading killers of adolescents are accidents (especially car accidents), homicides, and suicides.")
15
Matters of Life and Death – What Kills Us and When?
The causes of death change over the lifespan (continued) Young adults die from accidents, and cancers and heart diseases also begin to take a toll Among the 45-to-64 age group, cancers are the leading cause of death, followed by heart disease Among adults 65 and older, heart diseases are the leading cause (more than a third of all deaths) followed by cancers and cerebrovascular diseases (strokes)
 Young adults die from accidents, and cancers and heart diseases also begin to take a toll. Among the 45-to-64 age group, cancers are the leading cause of death, followed by heart disease. Among adults 65 and older, heart diseases are the leading cause (more than a third of all deaths) followed by cancers and cerebrovascular diseases (strokes)")
17
Matters of Life and Death – Theories of Aging
Theories to explain why we age and die fall into two categories Programmed theories Emphasize the systematic genetic control of aging Damage theories of aging Emphasize the processes that that cause errors in cells to accumulate and organ systems to deteriorate

18
Matters of Life and Death – Theories of Aging
Each species has its own characteristic maximum lifespan, or a limit on the number of years that a member of the species lives For humans, the longest documented and verified life was 122 years An individual’s genetic makeup combined with environmental factors will influence how rapidly he ages and how long he lives compared with other humans A fairly good way to estimate how long you will live is to average the longevity of your parents and grandparents

19
Matters of Life and Death – Theories of Aging
Researchers have identified specific genes that may be implicated in the basic aging process Many of these genes regulate cell division and become less active with age in normal adults These genes are inactive in children who have progeria, a premature aging disorder caused by a spontaneous (rather than inherited) mutation in a single gene Babies with progeria appear normal at first but age prematurely and die on average just as they are entering their teens, often of heart disease or stroke
 mutation in a single gene. Babies with progeria appear normal at first but age prematurely and die on average just as they are entering their teens, often of heart disease or stroke.")
20
Matters of Life and Death – Theories of Aging
Biological researchers suggest that humans are programmed with an “aging clock” in every cell of our bodies Hayflick (1976, 1994) discovered that cells from human embryos could divide only a certain number of times (50 times, plus or minus 10) This limit is referred to as the Hayflick limit Hayflick also demonstrated that cells taken from human adults divide even fewer times, presumably because they have already used up some of their capacity for reproducing themselves The maximum lifespan of a species is related to the Hayflick limit for that species
 discovered that cells from human embryos could divide only a certain number of times (50 times, plus or minus 10) This limit is referred to as the Hayflick limit. Hayflick also demonstrated that cells taken from human adults divide even fewer times, presumably because they have already used up some of their capacity for reproducing themselves. The maximum lifespan of a species is related to the Hayflick limit for that species.")
21
Matters of Life and Death – Theories of Aging
The mechanism of the cellular aging clock (as suggested by the Hayflick limit on cell division) is believed to be telomeres, the stretches of DNA that form the tips of chromosomes and that shorten with every cell division The progressive shortening of telomeres eventually makes cells unable to replicate and causes them to malfunction and die Thus, telomere length is a yardstick of biological aging Chronic stress is implicated in the rate at which telomeres shorten Chronic stress is linked to shorter than normal white blood cell telomeres, which in turn are associated with heightened risk for cardiovascular disease and death Lack of exercise, smoking, obesity, and low socioeconomic status are also associated with short telomeres
 is believed to be telomeres, the stretches of DNA that form the tips of chromosomes and that shorten with every cell division. The progressive shortening of telomeres eventually makes cells unable to replicate and causes them to malfunction and die. Thus, telomere length is a yardstick of biological aging. Chronic stress is implicated in the rate at which telomeres shorten. Chronic stress is linked to shorter than normal white blood cell telomeres, which in turn are associated with heightened risk for cardiovascular disease and death. Lack of exercise, smoking, obesity, and low socioeconomic status are also associated with short telomeres.")
22
Matters of Life and Death – Theories of Aging
Other programmed theories of aging focus on genetically programmed changes in the neuroendocrine system and the immune system Possibly the hypothalamus serves as an aging clock, systematically altering levels of hormones and brain chemicals in later life so that we die Perhaps aging is related to genetically governed changes in the immune system, associated with the shortening of the telomeres of its cells These changes could decrease the immune system’s ability to defend against potentially life-threatening foreign agents such as infections, cause it to mistake normal cells for invaders (as in autoimmune diseases), and make it contribute to inflammation and disease
, and make it contribute to inflammation and disease.")
23
Matters of Life and Death – Theories of Aging
Damage theories generally propose that death is caused by wear and tear, an accumulation of haphazard or random damage to cells and organs over time Free radicals (toxic and chemically unstable byproducts of metabolism) damage cells and compromise their functioning Free radicals are produced when oxygen reacts with certain molecules in the cells There is an extra, or “free,” electron that reacts with other molecules in the body to produce substances that damage normal cells, including their DNA Over time, the genetic code contained in the DNA of more and more cells becomes scrambled, and the body’s mechanisms for repairing such genetic damage simply cannot keep up with the chaos More cells then function improperly or cease to function, and the organism eventually dies
 damage cells and compromise their functioning. Free radicals are produced when oxygen reacts with certain molecules in the cells. There is an extra, or free, electron that reacts with other molecules in the body to produce substances that damage normal cells, including their DNA. Over time, the genetic code contained in the DNA of more and more cells becomes scrambled, and the body’s mechanisms for repairing such genetic damage simply cannot keep up with the chaos. More cells then function improperly or cease to function, and the organism eventually dies.")
24
Matters of Life and Death – Theories of Aging
“Age spots” on the skin of older people are a visible sign of the damage free radicals can cause Free radicals have also been implicated in some of the major diseases that become more common with age, most notably, cardiovascular diseases, cancer, and Alzheimer’s disease The most concerning effect of free radicals is damage to DNA because the result is more defective cells replicating themselves

25
Matters of Life and Death – Theories of Aging
Research on the basic causes of aging and death may lead to methods for increasing longevity Stem cell researchers may discover ways to replace aging cells or modify aging processes Researchers have also established that the enzyme telomerase can be used to prevent the telomeres from shortening and thus keep cells replicating and working longer However, telomerase treatments could go awry if they also make cancerous cells multiply more rapidly

26
Matters of Life and Death – Theories of Aging
Research on the basic causes of aging and death may lead to methods for increasing longevity (continued) Some researchers are focusing on preventing the damage caused by free radicals Antioxidants such as vitamins E and C (or foods high in them such as raisins, spinach, and blueberries) may increase longevity by inhibiting free radical activity and in turn helping prevent age-related diseases
 Some researchers are focusing on preventing the damage caused by free radicals. Antioxidants such as vitamins E and C (or foods high in them such as raisins, spinach, and blueberries) may increase longevity by inhibiting free radical activity and in turn helping prevent age-related diseases.")
27
Matters of Life and Death – Theories of Aging
Research on the basic causes of aging and death may lead to methods for increasing longevity (continued) At present, the most successful life-extension technique is caloric restriction, a highly nutritious but severely restricted diet representing a 30-40% or more cut in normal total caloric intake Laboratory studies involving rats and primates suggest that caloric restriction extends both the average longevity and the maximum lifespan of a species and that it delays or slows the progression of many age-related diseases Caloric restriction reduces the number of free radicals and other toxic products of metabolism
 At present, the most successful life-extension technique is caloric restriction, a highly nutritious but severely restricted diet representing a 30-40% or more cut in normal total caloric intake. Laboratory studies involving rats and primates suggest that caloric restriction extends both the average longevity and the maximum lifespan of a species and that it delays or slows the progression of many age-related diseases. Caloric restriction reduces the number of free radicals and other toxic products of metabolism.")
28
Learning Objectives What are Kübler-Ross’s stages of dying? How valid and useful is the theory? What is the Parkes/Bowlby attachment model of bereavement? Is there evidence to support this model? What is the dual-process model of bereavement?

29
The Experience of Death – Perspectives on Dying
Psychiatrist Elizabeth Kübler-Ross (1969, 1974) interviewed terminally ill patients and identified a common set of emotional responses to the knowledge that one has a serious, and probably fatal, illness Kübler-Ross’s “stages of dying” called attention to the emotional needs and reactions of dying people
 interviewed terminally ill patients and identified a common set of emotional responses to the knowledge that one has a serious, and probably fatal, illness. Kübler-Ross’s stages of dying called attention to the emotional needs and reactions of dying people.")
30
The Experience of Death – Perspectives on Dying
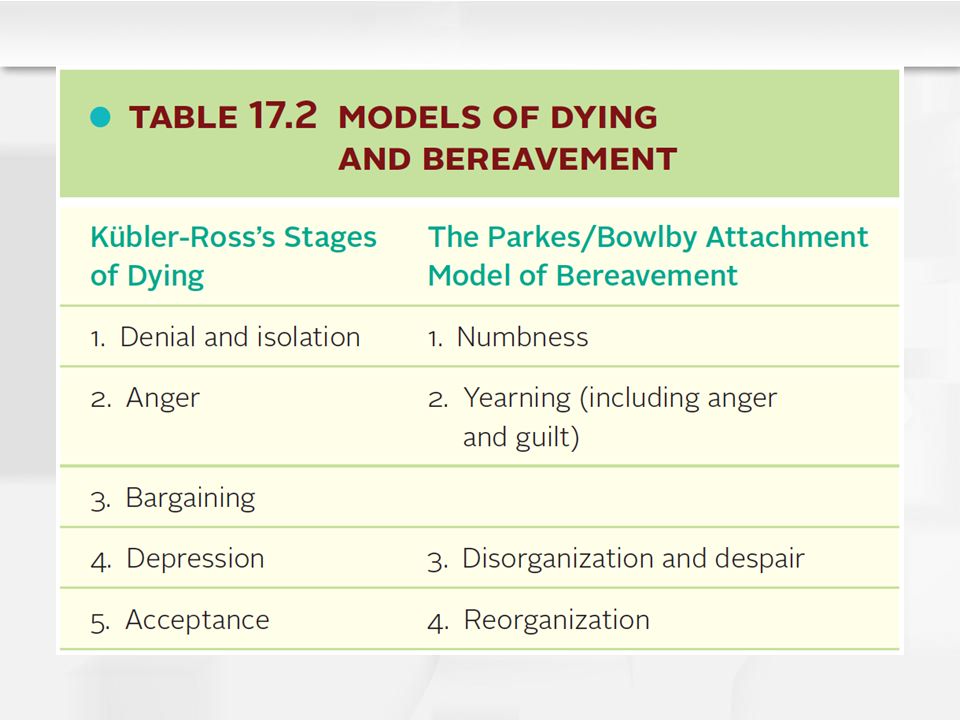
Kübler-Ross’s “stages of dying” are as follows Denial and isolation Anger Bargaining Depression Acceptance Kübler-Ross’s five “stages of dying” are as follows: Denial and isolation. -A common first response to dreadful news is to say, “No! It can’t be!” -Denial is a defense mechanism in which anxiety-provoking thoughts are kept out of, or “isolated” from, conscious awareness. --A woman who has just been diagnosed as having lung cancer may insist that the diagnosis is wrong—or accept that she is ill but be convinced that she will beat the odds and recover. 2. Anger. -Feelings of rage or resentment may be directed at anyone who is handy—doctors, nurses, or family members. 3. Bargaining. -The bargainer begs for some concession from God, the medical staff, or family members—if not for a cure, perhaps for a little more time, a little less pain, or provision for his children. 4. Depression. -As the dying person becomes even more aware of the reality of the situation, depression, despair, and a sense of hopelessness become the predominant emotional responses. - Grief focuses on the losses that have already occurred (for example, the loss of functional abilities) and the losses to come (separation from loved ones, the inability to achieve dreams, and so on). 5. Acceptance. -The inevitability of death may be accepted in a calm and peaceful manner. -Kübler-Ross (1969) describes the acceptance stage this way: “It is almost void of feelings. It is as if the pain had gone, the struggle is over, and there comes a time for ‘the final rest before the long journey,’ as one patient phrased it.”
 and the losses to come (separation from loved ones, the inability to achieve dreams, and so on). 5. Acceptance. -The inevitability of death may be accepted in a calm and peaceful manner. -Kübler-Ross (1969) describes the acceptance stage this way: It is almost void of feelings. It is as if the pain had gone, the struggle is over, and there comes a time for ‘the final rest before the long journey,’ as one patient phrased it.")
31
The Experience of Death – Perspectives on Dying
Kübler-Ross’s theory has been criticized Dying is not stagelike The nature and course of an illness affects reactions to it Individuals differ widely in their emotional responses to dying Personality traits, coping styles, and social competencies vary and influence the experience of dying

32
The Experience of Death – Perspectives on Bereavement
Responses to the death of a loved one may be differentiated Bereavement is a state of loss Grief is an emotional response to loss Mourning is a culturally prescribed way of displaying reactions to death

33
The Experience of Death – Perspectives on Bereavement
Relatives and friends also experience painful emotions before the death They may experience anticipatory grief, grieving before death occurs for what is happening and for what lies ahead Anticipatory grief can lessen later distress and improve outcomes of bereavement if it involves accepting the coming loss However, no amount of preparation and anticipatory grief can entirely eliminate the need to grieve after the death occurs

34
The Experience of Death – Perspectives on Bereavement
The Parkes/Bowlby attachment model of bereavement describes four predominant reactions to loss Numbness A sense of unreality and disbelief Yearning Severe pangs of grief, feelings of panic, bouts of uncontrolled weeping, physical pain Disorganization and despair Depression, despair, and apathy predominate. Reorganization Feel ready for new activities. Identity is revised

35
The Experience of Death – Perspectives on Bereavement
The process of grieving normally takes a year or more for widows and widowers but can take much longer

36
Caption: Peak times for different grief reactions in the Parkes-Bowlby phase model of grief in a sample of adults whose loved ones died of natural causes

38
The Experience of Death – Perspectives on Bereavement
Stroebe and Schut (1999) have suggested a dual-process model of bereavement in which the bereaved move between coping with the emotional blow of the loss and coping with the practical challenges of living, revising their identities, and reorganizing their lives Loss-oriented coping involves dealing with one’s emotions and reconciling oneself to the loss Restoration-oriented coping is focused on managing daily living and mastering new roles and challenges
 have suggested a dual-process model of bereavement in which the bereaved move between coping with the emotional blow of the loss and coping with the practical challenges of living, revising their identities, and reorganizing their lives. Loss-oriented coping involves dealing with one’s emotions and reconciling oneself to the loss. Restoration-oriented coping is focused on managing daily living and mastering new roles and challenges.")
39
The Experience of Death – Perspectives on Bereavement
Stroebe and Schut (1999) have suggested a dual-process model of bereavement (continued) Both processes in the dual-process model can involve positive and negative emotions (happy memories, painful memories) Over time, the emphasis shifts from loss-oriented to restoration-oriented coping As less time and energy need to be devoted to coping with grief, the balance of positive and negative emotions shifts in a positive direction
 have suggested a dual-process model of bereavement (continued) Both processes in the dual-process model can involve positive and negative emotions (happy memories, painful memories) Over time, the emphasis shifts from loss-oriented to restoration-oriented coping. As less time and energy need to be devoted to coping with grief, the balance of positive and negative emotions shifts in a positive direction.")
40
Caption: The dual-process model of coping and bereavement

41
Learning Objective What is the infant’s understanding of separation and death?

42
The Infant Infants lack the concept of death as permanent separation or loss and lack the cognitive capacity to interpret what has happened However, infants develop an understanding of concepts that pave the way for an understanding of death Possibly, infants first form a global category of things that are “all gone” and later divide it into subcategories, one of which is “dead”

43
The Infant Attachment theory provides a means for understanding infants’ reactions to loss of an attachment figure Infants first engage in vigorous protest, yearning and searching for the loved one and expressing outrage when they fail When an infant has not succeeded in finding the loved one, he begins to despair, displaying depression-like symptoms The baby loses hope, ends the search, and becomes apathetic and sad Grief may be reflected in a poor appetite, a change in sleeping patterns, excessive clinginess, or regression to less mature behavior

44
The Infant Attachment theory provides a means for understanding infants’ reactions to loss of an attachment figure (continued) Then the bereaved infant enters a detachment phase, in which he takes renewed interest in toys and companions and may begin to seek new relationships Infants will recover from the loss of an attachment figure most completely if they can rely on an existing attachment figure (for example, the surviving parent) or have the opportunity to attach themselves to someone new
 or have the opportunity to attach themselves to someone new.")
45
Learning Objectives How do children’s conception of death compare to a “mature” understanding of death? What factors might influence a child’s understanding of death? What is a dying child’s understanding of death? How do dying children cope with the prospect of their own death? How do children grieve?

47
The Child – Grasping the Concept of Death
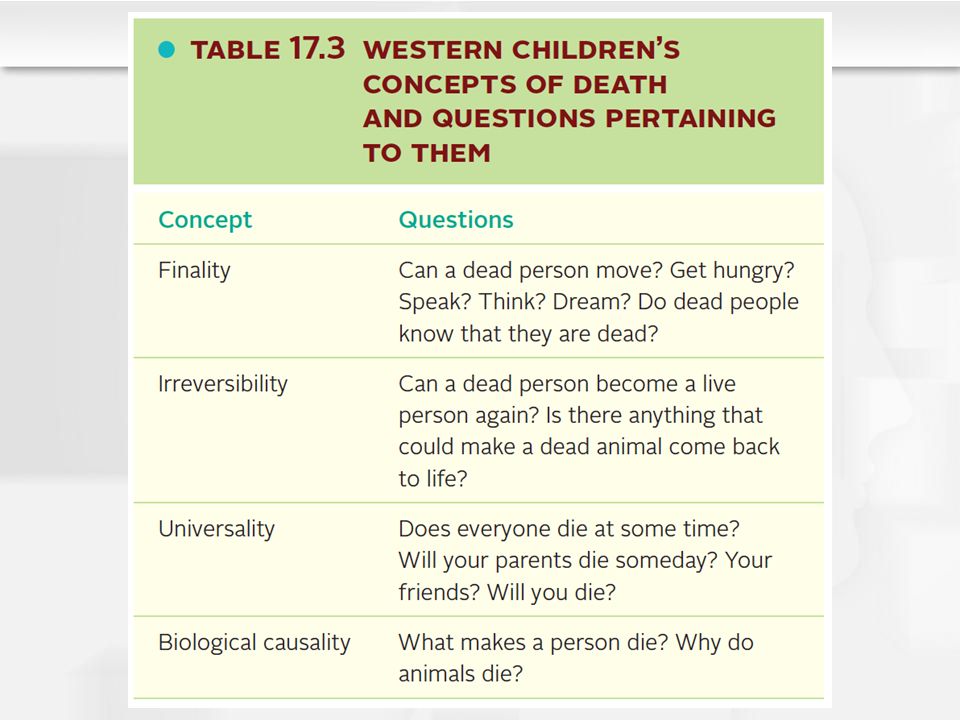
Children between age 3 and age 5 have limited understanding of death, especially its universality They may believed the dead live under altered circumstances and retain some capacities (experience hunger, continue to love) They may see death as reversible (as sleep, as a trip, or something that can be remedied with medical care) They may think death is caused by an external agent
 They may see death as reversible (as sleep, as a trip, or something that can be remedied with medical care) They may think death is caused by an external agent.")
48
The Child – Grasping the Concept of Death
Most children between age 5 and 7 understand that death is characterized by finality (cessation of life functions), irreversibility, and universality By age 10, children understand the biological causality of death The hardest concept of death for children to grasp
, irreversibility, and universality. By age 10, children understand the biological causality of death. The hardest concept of death for children to grasp.")
49
The Child – Grasping the Concept of Death
Children’s concepts of death are influenced by the cultural context in which they live, their life experiences, and the specific cultural and religious beliefs to which they are exposed A mature understanding of death is correlated with IQ

50
The Child – Grasping the Concept of Death
To help children understand death, experts suggest that parents Avoid the use of euphemisms to explain death (“asleep” or “gone away”) Give simple, honest answers to children’s questions Take advantage of opportunities (such as death of a pet) to teach children about death and express their emotions
 Give simple, honest answers to children’s questions. Take advantage of opportunities (such as death of a pet) to teach children about death and express their emotions.")
51
The Child – Grasping the Concept of Death
Research reveals that dying children are more aware of what is happening to them than adults realize Dying children experience many of the emotions that dying adults experience Preschool children may reveal their fears by having temper tantrums or portraying violent acts in their pretend play School-age children understand more about their situation and can talk about their feelings if given an opportunity to do so They may want to maintain a sense of normalcy and control in their lives Terminally ill children particularly benefit from a strong sense that their parents are there to care for them

52
The Child – The Bereaved Child
Four important messages have emerged from studies of bereaved children Children grieve Children may display “cycles of intense distress, emotional withdrawal, anger, and emotional detachment” (Lieberman, 2003)
")
53
The Child – The Bereaved Child
Four important messages have emerged from studies of bereaved children (continued) Children express their grief differently than adults do Preschoolers are likely to manifest it in problems with sleeping, eating, toileting, and other routines Negative moods, dependency, and temper tantrums are also common Older children express their sadness, anger, and fear more directly, although somatic symptoms such as headaches and other physical ailments are also common
 Children express their grief differently than adults do. Preschoolers are likely to manifest it in problems with sleeping, eating, toileting, and other routines. Negative moods, dependency, and temper tantrums are also common. Older children express their sadness, anger, and fear more directly, although somatic symptoms such as headaches and other physical ailments are also common.")
54
The Child – The Bereaved Child
Four important messages have emerged from studies of bereaved children (continued) Children lack some of the coping resources that adults possess Children primarily have behavioral or action coping strategies at their disposal
 Children lack some of the coping resources that adults possess. Children primarily have behavioral or action coping strategies at their disposal.")
55
The Child – The Bereaved Child
Four important messages have emerged from studies of bereaved children (continued) Children are vulnerable to long-term negative effects of bereavement Well beyond the first year after the death, some bereaved children continue to display problems such as unhappiness, low self-esteem, social withdrawal, difficulty in school, and problem behavior Some children develop psychological problems that carry into adulthood, such as overreactivity to stress and stress-related health problems, depression and other psychological disorders, or insecurity in later attachment relationships
 Children are vulnerable to long-term negative effects of bereavement. Well beyond the first year after the death, some bereaved children continue to display problems such as unhappiness, low self-esteem, social withdrawal, difficulty in school, and problem behavior. Some children develop psychological problems that carry into adulthood, such as overreactivity to stress and stress-related health problems, depression and other psychological disorders, or insecurity in later attachment relationships.")
56
The Child – The Bereaved Child
Most bereaved children, especially those who have effective coping skills and solid social support, adapt quite well They are especially likely to fare well If they receive good parenting If caregivers communicate that they will be loved and cared for If they have opportunities to talk about and share their grief. Bereavement with the help of a caring and supportive caregiver is associated with adaptive responses to stress in adulthood Bereaved children who perceive a lack of caring support after the death may have difficulty handling stress later in life

57
Learning Objectives What is the adolescent’s understanding of death? Is an adolescent’s reaction to death different from the reactions of a child or adult?

58
The Adolescent Adolescents understand that death means the irreversible cessation of biological processes Adolescents are able to think in more abstract ways about death as they move from Piaget’s concrete-operational stage to formal-operational thinking Can think about the meaning of death and hypothetical ideas (e.g., the existence of an afterlife)
")
59
The Adolescent The themes of adolescence are likely to be reflected in the concerns of adolescents who become terminally ill Body image Acceptance by peers Autonomy versus necessary dependency upon parents and medical personnel Identity and the future

60
The Adolescent Adolescents’ reactions to the deaths of family members and friends reflect the themes of the adolescent period While still dependent on their parents for emotional support and guidance, adolescents who lose a parent to death may carry on an internal dialogue with the dead parent for years Adolescents are often devastated when a close friend dies, but this grief may not be taken seriously by others

61
The Adolescent Adolescents grieve as adults do However, teens may be reluctant to express their grief for fear of seeming abnormal or losing control and it may instead manifest in delinquent behavior or somatic ailments

62
Learning Objectives How do family members react and cope with the loss of a spouse, a child, and a parent? What factors contribute to effective and ineffective coping with grief? What can be done for those who are dying and for those who are bereaved to better understand and face the reality of death?

63
The Adult – Death in the Family Context
Experiencing the death of a spouse or partner becomes increasingly likely as we age The death of a partner means the loss of an attachment figure and often precipitates other changes such as the need to move, enter the labor force or change jobs, etc. Bereaved partners must redefine their roles, identities, and basic assumptions about life

64
The Adult – Death in the Family Context
Research on widows and widowers younger than age 45 concluded that bereaved adults progress through overlapping phases of numbness, yearning, disorganization and despair, and reorganization The grieving process affects physical, emotional, and cognitive functioning Widows and widowers are at risk for illness and physical symptoms such as loss of appetite and sleep disruption They tend to overindulge in alcohol, tranquilizers, and cigarettes

65
The Adult – Death in the Family Context
The grieving process affects physical, emotional, and cognitive functioning (continued) Cognitive functions such as memory and decision-making are often impaired Emotional problems such as loneliness and anxiety are common Most bereaved partners do not become clinically depressed, but many display increased symptoms of depression in the year after the death Widows and widowers as a group have higher-than-average rates of death
 Cognitive functions such as memory and decision-making are often impaired. Emotional problems such as loneliness and anxiety are common. Most bereaved partners do not become clinically depressed, but many display increased symptoms of depression in the year after the death. Widows and widowers as a group have higher-than-average rates of death.")
66
Caption: Depression symptom scores of five subgroups of elderly widows and widowers an average of 3 years before, 6 months after, and 18 months after the death of their spouse

67
The Adult – Death in the Family Context
Bonanno and colleagues (2008) identified the five most prevalent patterns of adjustment shown by widows and widowers A resilient pattern in which distress is at low levels all along The most common pattern, characterizing almost half the study sample Well-adjusted, happily married people with good coping resources Common grief, with heightened, then diminishing, distress after the loss
 identified the five most prevalent patterns of adjustment shown by widows and widowers. A resilient pattern in which distress is at low levels all along. The most common pattern, characterizing almost half the study sample. Well-adjusted, happily married people with good coping resources. Common grief, with heightened, then diminishing, distress after the loss.")
68
The Adult – Death in the Family Context
Bonanno and colleagues (2008) identified the five most prevalent patterns of adjustment shown by widows and widowers (continued) Chronic grief in which loss brings distress and the distress lingers Chronic depression in which individuals who were depressed before the loss remain so after it A depressed-improved pattern in which individuals who were depressed before the loss become less depressed after the death
 identified the five most prevalent patterns of adjustment shown by widows and widowers (continued) Chronic grief in which loss brings distress and the distress lingers. Chronic depression in which individuals who were depressed before the loss remain so after it. A depressed-improved pattern in which individuals who were depressed before the loss become less depressed after the death.")
69
The Adult – Death in the Family Context
Bonanno and colleagues (2005) studied the bereavement patterns of partners of gay men who died of AIDS About half demonstrated the resilient pattern of coping in which distress is at low levels all along
 studied the bereavement patterns of partners of gay men who died of AIDS. About half demonstrated the resilient pattern of coping in which distress is at low levels all along.")
70
The Adult – Death in the Family Context
Gay and lesbian partners sometimes experience disenfranchised grief Grief that is not fully recognized or appreciated by other people and therefore may not receive much sympathy and support Generally likely to be harder to cope with than socially recognized grief

71
The Adult – Death in the Family Context
Disenfranchised grief is likely when The relationship is not recognized (as when a gay relationship is in the closet) The loss is not acknowledged (as when the loss of a pet is not viewed as a “real” loss) The bereaved person is excluded from mourning activities (as happens sometimes to young children and cognitively impaired elders) The cause of death is stigmatized (as in suicides or drug overdoses)
 The loss is not acknowledged (as when the loss of a pet is not viewed as a real loss) The bereaved person is excluded from mourning activities (as happens sometimes to young children and cognitively impaired elders) The cause of death is stigmatized (as in suicides or drug overdoses)")
72
The Adult – Death in the Family Context
Complicated grief is grief that is unusually prolonged or intense and that impairs functioning. Occurs in a minority of cases, up to about 15% Continues for many years

73
The Adult – Death in the Family Context
No loss seems more difficult for an adult than the death of a child Being unable to make sense of a child’s death is associated with more intense grief

74
The Adult – Death in the Family Context
The death of a child alters the family system The marital relationship is likely to be strained because each partner grieves in a unique way and one may not be able to provide emotional support for the other Strains are likely to be especially severe if the marriage was shaky before the child’s death The odds of marital problems and divorce tend to increase after the death of a child However, most couples stay together and some feel closer than ever

75
The Adult – Death in the Family Context
The death of a child alters the family system (continued) Children are deeply affected when a brother or sister dies, but their grief is often not fully appreciated Their distraught parents may not be able to support them effectively Grandparents grieve following the death of a child, both for their grandchild and for their child, the bereaved parent Grandparents may also experience disenfranchised grief, ignored while all the supportive attention focuses on the parents
 Children are deeply affected when a brother or sister dies, but their grief is often not fully appreciated. Their distraught parents may not be able to support them effectively. Grandparents grieve following the death of a child, both for their grandchild and for their child, the bereaved parent. Grandparents may also experience disenfranchised grief, ignored while all the supportive attention focuses on the parents.")
76
The Adult – Death in the Family Context
Adjusting to the death of a parent is usually not as difficult as adjusting to the death of a romantic partner or child The death of a parent is a normative life transition that we expect and that most of us don’t face until middle age

77
The Adult – Death in the Family Context
Loss of a parent can be a turning point in an adult’s life with effects on his identity and relationships with his partner, children (who are grieving the loss of their grandparent), surviving parent, and siblings Adult children may feel vulnerable and alone in the world when their parents no longer stand between them and death Guilt about not doing enough for the parent who died is common Compared with adults who are not bereaved, adults who have lost a parent in the past 3 years have higher rates of psychological distress, alcohol use, and health problems
, surviving parent, and siblings. Adult children may feel vulnerable and alone in the world when their parents no longer stand between them and death. Guilt about not doing enough for the parent who died is common. Compared with adults who are not bereaved, adults who have lost a parent in the past 3 years have higher rates of psychological distress, alcohol use, and health problems.")
78
The Adult – Challenges to the Grief-Work Perspective
Research on bereavement has been guided by the grief-work perspective, the view that to cope adaptively with death, bereaved people must confront their loss, experience painful emotions, work through those emotions, and move toward a detachment from the deceased This view is widely held in our society by therapists and people in general The grief-work perspective influences what we view as an abnormal reaction to death

79
The Adult – Challenges to the Grief-Work Perspective
Recently the grief-work perspective has been challenged Cross-cultural studies reveal that there are many ways to grieve and suggest that the grief-work model of bereavement may be culturally biased There is little research support for the assumption that bereaved individuals must confront their loss and experience painful emotions to cope successfully

80
The Adult – Challenges to the Grief-Work Perspective
The grief-work perspective has been challenged (continued) The view that we must break our bonds to the deceased to overcome our grief is under attack Bowlby (1980) observed that many bereaved individuals revise their internal working models of self and others and continue their relationships with their deceased loved ones on new terms Recent research supports Bowlby’s observations and suggests that many bereaved individuals maintain their attachments to the deceased indefinitely through continuing bonds They reminisce and share memories of the deceased, derive comfort from the deceased’s possessions, consult with the deceased and feel his or her presence, seek to make the deceased proud of them, etc.
 The view that we must break our bonds to the deceased to overcome our grief is under attack. Bowlby (1980) observed that many bereaved individuals revise their internal working models of self and others and continue their relationships with their deceased loved ones on new terms. Recent research supports Bowlby’s observations and suggests that many bereaved individuals maintain their attachments to the deceased indefinitely through continuing bonds. They reminisce and share memories of the deceased, derive comfort from the deceased’s possessions, consult with the deceased and feel his or her presence, seek to make the deceased proud of them, etc.")
81
The Adult – Challenges to the Grief-Work Perspective
The grief-work perspective has been challenged (continued) Many individuals who continue their bonds benefit from the continuing, but redefined, attachment Other research found that, for some people, continuing bonds was a sign of continued yearning and prolonged or complicated grief When the bonds involved hallucinations and illusions that reflected a continuing effort to reunite with the deceased
 Many individuals who continue their bonds benefit from the continuing, but redefined, attachment. Other research found that, for some people, continuing bonds was a sign of continued yearning and prolonged or complicated grief. When the bonds involved hallucinations and illusions that reflected a continuing effort to reunite with the deceased.")
82
The Adult – Who Copes and Who Succumbs?
Researchers have attempted to determine what risk and protective factors distinguish people who cope well with loss from people who cope poorly Coping with bereavement is influenced by The individual’s personal resources The nature of the loss The surrounding context of support and stressors

83
The Adult – Who Copes and Who Succumbs?
Coping with bereavement is influenced by the individual’s personal resources (continued) Attachment style can be an important resource or it can be a liability Having a secure attachment style is associated with coping relatively well with the death of a loved one Individuals who developed a resistant, avoidant, or disorganized attachment style do not cope well with loss Coping with bereavement is influenced by the individual’s personal resources. Attachment style can be an important resource or it can be a liability. -Having a secure attachment style is associated with coping relatively well with the death of a loved one. -Individuals who have developed a resistant (or preoccupied) style of attachment tend to be overly dependent and display extreme and chronic grief and anxiety after a loss, ruminating about the death and clinging to the loved one rather than revising their attachment bond -Those who have developed an avoidant (or dismissing) attachment style tend to have difficulty expressing their emotions or seeking comfort from other people; they may do little grieving and seem to disengage from or even devalue the person lost -Those who have a disorganized attachment style rooted in unpredictable and anxiety-arousing parenting appear to be especially unequipped to cope with loss; they may turn inward, harm themselves, or abuse alcohol or drugs.
 Attachment style can be an important resource or it can be a liability. Having a secure attachment style is associated with coping relatively well with the death of a loved one. Individuals who developed a resistant, avoidant, or disorganized attachment style do not cope well with loss. Coping with bereavement is influenced by the individual’s personal resources. Attachment style can be an important resource or it can be a liability. -Having a secure attachment style is associated with coping relatively well with the death of a loved one. -Individuals who have developed a resistant (or preoccupied) style of attachment tend to be overly dependent and display extreme and chronic grief and anxiety after a loss, ruminating about the death and clinging to the loved one rather than revising their attachment bond. -Those who have developed an avoidant (or dismissing) attachment style tend to have difficulty expressing their emotions or seeking comfort from other people; they may do little grieving and seem to disengage from or even devalue the person lost. -Those who have a disorganized attachment style rooted in unpredictable and anxiety-arousing parenting appear to be especially unequipped to cope with loss; they may turn inward, harm themselves, or abuse alcohol or drugs.")
84
The Adult – Who Copes and Who Succumbs?
Coping with bereavement is influenced by the individual’s personal resources (continued) Personality and coping style are personal resources that influence how successfully people cope with death Individuals who have difficulty coping tend to have low self-esteem and lack a sense that they are in control of their lives Many also rely on ineffective coping strategies such as denial and escape through alcohol and drugs People who are optimistic, find positive ways of interpreting their loss, and use active coping strategies experience less intense grief reactions and are more likely to report personal growth after their losses than other bereaved adults
 Personality and coping style are personal resources that influence how successfully people cope with death. Individuals who have difficulty coping tend to have low self-esteem and lack a sense that they are in control of their lives. Many also rely on ineffective coping strategies such as denial and escape through alcohol and drugs. People who are optimistic, find positive ways of interpreting their loss, and use active coping strategies experience less intense grief reactions and are more likely to report personal growth after their losses than other bereaved adults.")
85
The Adult – Who Copes and Who Succumbs?
Coping with bereavement is influenced by the nature of the loss The closeness of the person’s relationship to the deceased is a key factor The cause of death can also influence bereavement outcomes Children’s deaths may be painful because they are often the result of “senseless” and violent events such as car accidents, homicides, and suicide However, sudden deaths are not necessarily harder to cope with overall than expected deaths from illnesses Possibly because any advantages of being forewarned of death are offset by the stresses of caring for a dying loved one

86
The Adult – Who Copes and Who Succumbs?
Coping with bereavement is influenced by the surrounding context of support and stressors Grief reactions are influenced positively by the presence of a strong social support system Good parenting is especially important for the child or adolescent whose parent dies Family members of all ages recover best when the family is cohesive and family members can share their emotions Friends and colleagues can provide social support Grief reactions are negatively by additional life stressors It is particularly difficult when stressors demand what the dual-process model of bereavement calls restoration-oriented coping Require energy and resources

87
The Adult – Bereavement and Human Development
Scholars are finding that bereavement can have positive consequences and sometimes foster personal growth Many bereaved individuals believe that they have become stronger, wiser, more loving, and more religious people with a greater appreciation of life Many widows master new skills, become more independent, and emerge with new identities and higher self-esteem, especially those who depended heavily on their spouses and then discover that they can manage life on their own

88
Taking the Sting Out of Death – For the Dying
The care of dying people has improved in the past few decades Palliative care is aimed at meeting the physical, psychological, and spiritual needs of patients with incurable illnesses, not at curing disease or prolonging life Hospice is a form of palliative care that supports dying people and their families through a philosophy of “caring” rather than “curing”

89
Taking the Sting Out of Death – For the Dying
Hospice care includes the following features The dying person and his family decide what support they need and want Attempts to cure the patient or prolong his life are deemphasized (death is not hastened) Pain control is emphasized The setting for care is as normal as possible (preferably the patient’s own home or a homelike facility that does not have the sterile atmosphere of many hospital wards) Bereavement counseling is provided to the family before and after the death
 Pain control is emphasized. The setting for care is as normal as possible (preferably the patient’s own home or a homelike facility that does not have the sterile atmosphere of many hospital wards) Bereavement counseling is provided to the family before and after the death.")
90
Taking the Sting Out of Death - For the Dying
An evaluation that compared hospice facility care, at-home hospice care, and conventional hospital care in Great Britain found that hospice patients spent more of their last days without pain, underwent fewer medical interventions and operations, and received nursing care that was more oriented to their emotional needs. Spouses and partners, parents, and other relatives of dying people who received hospice care appear to display fewer symptoms of grief and have a greater sense of well-being 1 to 2 years after the death compared to similar relatives who coped with a death without benefit of hospice care.

91
Taking the Sting Out of Death – For the Bereaved
Most bereaved individuals deal with death as a normal life transition on their own and with support from significant others However, there are many treatment options intended to prevent problems before they arise and interventions designed to treat serious psychological disorders precipitated by a loss Bereaved individuals at risk for complicated grief or depression can benefit from therapy or counseling aimed at preventing or treating debilitating grief

92
Taking the Sting Out of Death – For the Bereaved
Because death takes place in a family context, family therapy can help bereaved parents and children communicate more openly and support one another Family therapy also can help parents deal with their own emotional issues so that they can provide the warm and supportive parenting that can be so critical in facilitating their children’s recovery

93
Learning Objective What are the major themes of lifespan development that have been covered throughout the text?

94
Major Developmental Themes
Nature and nurture truly interact in development We are whole people throughout the lifespan The developmental domains are interrelated Development proceeds in multiple directions with both continuity and discontinuity There is much plasticity in development

95
Major Developmental Themes
We are diverse individuals and become even more so as we age We develop in a cultural and historical context We are active in our own development Development is a lifelong process Development is best viewed from multiple perspectives

Similar presentations








 2012 The McGraw-Hill Companies, Inc. Chapter 17 Death, Dying, and Grieving PowerPoints developed by Nicholas Greco IV, College of Lake County, Grayslake,>")










